Proliferating Trichilemmal Cyst with Lymphadenopathy: a Discussion of Cutaneous Neoplasms Involving the Scalp
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dermatologists' Perceptions on the Utility and Limitations
RESEARCH/Original Article Journal of Telemedicine and Telecare 2021, Vol. 27(3) 166–173 Dermatologists’ perceptions on the ! The Author(s) 2019 utility and limitations of teledermatology Article reuse guidelines: sagepub.com/journals-permissions after examining 55,000 lesions DOI: 10.1177/1357633X19864829 journals.sagepub.com/home/jtt Mara Giavina Bianchi , Andre Santos and Eduardo Cordioli Abstract Introduction: Few studies have assessed the perception of teledermatologists about the utility and limitations of teledermatology, especially to diagnose a broad range of skin diseases. This study aimed to evaluate dermatologists’ confidence in teledermatology, its utility and limitations for dermatological conditions in primary care. Methods: An analytical study that used a survey for dermatologists who diagnosed 30,916 patients with 55,012 lesions through teledermatology during a 1-year project in S~ao Paulo, Brazil. Results: Dermatologists found teledermatology useful for triage and diagnosis, especially for xerotic eczema, pigmen- tary disorders and superficial infections. Their confidence in teledermatology was statistically higher by the end of the project (p ¼ 0.0012). Limitations included some technical issues and the impossibility to suggest how soon the patient should be assisted face-to-face by a dermatologist. The most treatable group of diseases by teledermatology was superficial infections (92%). The use of dermoscopy images would significantly increase the confidence to treat atypical naevi and malignant tumours (p < 0.0001 and p ¼ 0.0003 respectively). Follow-ups by teledermatology or feedback from primary-care physicians would be desirable, according to the dermatologists. Discussion: We found it interesting that dermatologists became increasingly confident in teledermatology after the project and how they classified teledermatology as useful for triage, diagnosis and even treatment of most types of skin conditions followed at primary care. -

An Institutional Experience
Original Research Article Skin Adnexal Tumors- An Institutional Experience 1 2* 3 4 5 6 Rekha M Haravi , Roopa K N , Priya Patil , Rujuta Datar , Meena N Jadhav , Shreekant K Kittur 1,5Associate Professor, 2Post Graduate Student, 3,4Assistant Professor, 6Professor & HOD, Department of Pathology, Belgaum Institute of Medical Sciences Dr B R Ambedkar Road, Belagavi, Karnataka – 590001, INDIA. Email: [email protected] Abstract Background: Skin adnexal tumors are a wide spectrum of benign and malignant tumors that differentiate towards one or more adnexal structures found in normal skin. The adnexal structures of skin are the hair follicles, sebaceous glands, eccrine and apocrine sweat glands. These skin adnexal tumors are often difficult to diagnose clinically. This retrospective study was undertaken to know the various histomorphological patterns of skin adnexal tumors at our institution and to determine the incidence among the genders and age groups along with the site distribution. Materials and methods: A total of 40 specimens received and diagnosed as skin adnexal tumors in the department of Pathology at Belgaum Institute of Medical Sciences, Belagavi for a period of 6 years from January 2014 to December 2019 were taken for the study. Histopathological slides prepared from tissue blocks retrieved from departmental archives were reviewed and classified according to the WHO classification 2017. Results: Out of the total 40 samples, benign tumors were 36 (90%) and malignant were 4 (10%). Largest group was the benign tumors of apocrine and eccrine differentiation (47.5%) followed by benign tumors of hair follicle differentiation (40%). Malignant tumors of sebaceous differentiation were 5%, malignant tumors of eccrine and apocrine differentiation were 2.5% and malignant hair follicle differentiation tumors were 2.5% of the total. -

Inherited Skin Tumour Syndromes
CME GENETICS Clinical Medicine 2017 Vol 17, No 6: 562–7 I n h e r i t e d s k i n t u m o u r s y n d r o m e s A u t h o r s : S a r a h B r o w n , A P a u l B r e n n a n B a n d N e i l R a j a n C This article provides an overview of selected genetic skin con- and upper trunk. 1,2 These lesions are fibrofolliculomas, ditions where multiple inherited cutaneous tumours are a cen- trichodiscomas and acrochordons. Patients are also susceptible tral feature. Skin tumours that arise from skin structures such to the development of renal cell carcinoma, lung cysts and as hair, sweat glands and sebaceous glands are called skin pneumothoraces. 3 appendage tumours. These tumours are uncommon, but can Fibrofolliculomas and trichodiscomas clinically present as ABSTRACT have important implications for patient care. Certain appenda- skin/yellow-white coloured dome shaped papules 2–4 mm in geal tumours, particularly when multiple lesions are seen, may diameter (Fig 1 a and Fig 1 b). 4 These lesions usually develop indicate an underlying genetic condition. These tumours may in the third or fourth decade.4 In the case of fibrofolliculoma, not display clinical features that allow a secure diagnosis to be hair specific differentiation is seen, whereas in the case of made, necessitating biopsy and dermatopathological assess- trichodiscoma, differentiation is to the mesodermal component ment. -

The Best Diagnosis Is: H&E, Original Magnification 2
Dermatopathology Diagnosis The best diagnosis is: H&E, original magnification 2. a. adenoid cysticcopy carcinoma arising within a spiradenoma b. cylindroma and spiradenoma collision tumor c. microcysticnot change within a spiradenoma d. mucinous carcinoma arising within a spiradenoma Doe. trichoepithelioma and spiradenoma collision tumor CUTIS H&E, original magnification 100. PLEASE TURN TO PAGE 211 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Amanda F. Marsch, MD; Jeffrey B. Shackelton, MD; Dirk M. Elston, MD Dr. Marsch is from the Department of Dermatology, University of Illinois at Chicago. Drs. Shackelton and Elston are from the Ackerman Academy of Dermatopathology, New York, New York. The authors report no conflict of interest. Correspondence: Amanda F. Marsch, MD, University of Illinois at Chicago, 808 S Wood St, Chicago, IL 60612 ([email protected]). 192 CUTIS® WWW.CUTIS.COM Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Dermatopathology Diagnosis Discussion Trichoepithelioma and Spiradenoma Collision Tumor he coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen Tis unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline muta- tions in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spirad- Figure 1. -

Rippled-Pattern Sebaceoma: a Report of a Lesion on the Back with a Review of the Literature
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of Fukui Repository Rippled-pattern sebaceoma: A report of a lesion on the back with a review of the literature Takahiro Kiyohara, M.D., Masanobu Kumakiri, M.D., Hiroaki Kuwahara, M.D., Atsuko Saitoh, M.D., and Shinichi Ansai, M.D. Department of Dermatology (T.K., M.K.), University of Fukui, Fukui; Division of Plastic Surgery (H.K.), Obihiro-Kousei General Hospital, Obihiro: Sapporo Institute for Dermatopathology (S.A.), Sapporo, Japan Address correspondence and reprint requests to: Takahiro Kiyohara, M.D. Department of Dermatology, University of Fukui 23-3 Shimoaizuki, Matsuoka-cho, Yoshida-gun, Fukui 910-1193, Japan Tel: +81 776 61 3111 Fax: +81 776 61 8112 e-mail: kiyo @ fmsrsa.fukui-med.ac.jp Abstract A 68-year-old Japanese man presented with a tumor that had been present for 5 to 6 years on the right back. Physical examination revealed a dome-shaped, 12x13-mm, dark red tumor. The tumor was excised with a 2 to 3-mm margin. The patient has remained free of disease during 77-months of follow-up. Microscopic examination revealed a bulb-like tumor in the dermis, contiguous with the overlying epidermis. It was composed of small, monomorphous, cigar-shaped basaloid cells in linear, parallel rows, resembling the palisading of nuclei of Verocay bodies, and presenting a rippled-pattern. There were scattered cells showing sebaceous differentiation with vacuolated cytoplasm and scalloped nuclei. There were tiny, duct-like spaces. The tumor revealed characteristics of rippled-pattern sebaceoma. -

Proliferating Trichilemmal Cyst of the Scalp: Nine Cases and Literature Review
Otorhinolaryngology-Head and Neck Surgery Research Article ISSN: 2398-4937 Proliferating trichilemmal cyst of the scalp: Nine cases and literature review ElBenaye J1,3*, Sinaa M2,3, Elkhachine Y1,3, Sakkah A1,3, Jakar A1 and Elhaouri M1 1Department of Dermatology, Moulay Ismail Military Hospital, Meknes, Morocco 2Department of Cytopathology, Moulay Ismail Military Hospital, Meknes, Morocco 3Department of Medicine and Pharmacy, Sidi Mohammed Ben Abdellah University (USMBA), Fes, Morocco Abstract Background: proliferating trichilemmal cyst (PTC) is a rare adnexal tumor, primarily sitting on the scalp of elderly women. Its evolution is generally benign despite the rare malignant cases described. We report a series of 9 cases of which one is malignant and metastatic. Material and methods: We retrospectively reviewed data of all patients with PTC seen at department of dermatology in the Meknes military hospital, between January 2013 and December 2017. Results: Nine cases of PTC were diagnosed, which 8 in elderly women, with 62 years mean age. Trauma was found in one third of cases correlated with rapid growth of the tumor. The latter was symptomatic in 2/3 of the cases. Ulceration involved only the malignant case. The size varied from 1,5 to 12 cm. Recurrence after surgery was noted in 2 cases (malignant tumor and multi-cystic tumor). Discussion: PTC appears to have a well-distinguished profile of the simple trichilemmal cyst. Some clinical and histological features may constitute prognostic factors of aggressiveness. Histological and immunohistochemical study is crucial in the management. A large excision remains the only guarantee of complete remission without recurrence or metastasis. -

2016 Essentials of Dermatopathology Slide Library Handout Book
2016 Essentials of Dermatopathology Slide Library Handout Book April 8-10, 2016 JW Marriott Houston Downtown Houston, TX USA CASE #01 -- SLIDE #01 Diagnosis: Nodular fasciitis Case Summary: 12 year old male with a rapidly growing temple mass. Present for 4 weeks. Nodular fasciitis is a self-limited pseudosarcomatous proliferation that may cause clinical alarm due to its rapid growth. It is most common in young adults but occurs across a wide age range. This lesion is typically 3-5 cm and composed of bland fibroblasts and myofibroblasts without significant cytologic atypia arranged in a loose storiform pattern with areas of extravasated red blood cells. Mitoses may be numerous, but atypical mitotic figures are absent. Nodular fasciitis is a benign process, and recurrence is very rare (1%). Recent work has shown that the MYH9-USP6 gene fusion is present in approximately 90% of cases, and molecular techniques to show USP6 gene rearrangement may be a helpful ancillary tool in difficult cases or on small biopsy samples. Weiss SW, Goldblum JR. Enzinger and Weiss’s Soft Tissue Tumors, 5th edition. Mosby Elsevier. 2008. Erickson-Johnson MR, Chou MM, Evers BR, Roth CW, Seys AR, Jin L, Ye Y, Lau AW, Wang X, Oliveira AM. Nodular fasciitis: a novel model of transient neoplasia induced by MYH9-USP6 gene fusion. Lab Invest. 2011 Oct;91(10):1427-33. Amary MF, Ye H, Berisha F, Tirabosco R, Presneau N, Flanagan AM. Detection of USP6 gene rearrangement in nodular fasciitis: an important diagnostic tool. Virchows Arch. 2013 Jul;463(1):97-8. CONTRIBUTED BY KAREN FRITCHIE, MD 1 CASE #02 -- SLIDE #02 Diagnosis: Cellular fibrous histiocytoma Case Summary: 12 year old female with wrist mass. -

Genetics of Skin Appendage Neoplasms and Related Syndromes
811 J Med Genet: first published as 10.1136/jmg.2004.025577 on 4 November 2005. Downloaded from REVIEW Genetics of skin appendage neoplasms and related syndromes D A Lee, M E Grossman, P Schneiderman, J T Celebi ............................................................................................................................... J Med Genet 2005;42:811–819. doi: 10.1136/jmg.2004.025577 In the past decade the molecular basis of many inherited tumours in various organ systems such as the breast, thyroid, and endometrium.2 syndromes has been unravelled. This article reviews the clinical and genetic aspects of inherited syndromes that are Clinical features of Cowden syndrome characterised by skin appendage neoplasms, including The cutaneous findings of Cowden syndrome Cowden syndrome, Birt–Hogg–Dube syndrome, naevoid include trichilemmomas, oral papillomas, and acral and palmoplantar keratoses. The cutaneous basal cell carcinoma syndrome, generalised basaloid hallmark of the disease is multiple trichilemmo- follicular hamartoma syndrome, Bazex syndrome, Brooke– mas which present clinically as rough hyperker- Spiegler syndrome, familial cylindromatosis, multiple atotic papules typically localised on the face (nasolabial folds, nose, upper lip, forehead, ears3 familial trichoepitheliomas, and Muir–Torre syndrome. (fig 1A, 1C, 1D). Trichilemmomas are benign ........................................................................... skin appendage tumours or hamartomas that show differentiation towards the hair follicles kin consists of both epidermal and dermal (specifically for the infundibulum of the hair 4 components. The epidermis is a stratified follicle). Oral papillomas clinically give the lips, Ssquamous epithelium that rests on top of a gingiva, and tongue a ‘‘cobblestone’’ appearance basement membrane, which separates it and its and histopathologically show features of 3 appendages from the underlying mesenchymally fibroma. The mucocutaneous manifestations of derived dermis. -

Histopathological Profile of Surgically Excised Scalp and Skull Lesions Asuman Kilitci¹ , Ziya Asan²
DOI: 10.5152/cjms.2018.442 Original Article Histopathological Profile of Surgically Excised Scalp and Skull Lesions Asuman Kilitci¹ , Ziya Asan² 1Department of Pathology, Ahi Evran University School of Medicine, Kırşehir, Turkey ²Department of Neurosurgery, Ahi Evran University School of Medicine, Kırşehir, Turkey ORCID ID of the author: A.K. 0000-0002-5489-2222; Z.A. 0000-0001-8468-9156 Cite this article as: Kilitci A, Asan Z. Histopathological Profile of Surgically Excised Scalp and Skull Lesions. Cyprus J Med Sci 2018; 3: 63-7. BACKGROUND/AIMS Although subcutaneous lesions of the scalp are more common than those of the skull, few studies in literature have assessed the frequency of scalp and skull diseases. The goal of this study was to establish the frequency and main histopathological findings of these lesions. Our study is one of the largest series and shows that the incidence of surgically excised scalp masses includes an array of diseases. MATERIAL and METHODS We reviewed 265 extracranial masses from 173 patients. The mean age of the patients, gender distribution, localization and characteristics of lesions, histopathological type and radiological features were analyzed. RESULTS One-hundred (57.8%) patients were males and 73 (42.2%) were females. The mean age was 42.98 (range, 5-87). In total, 261 were within the scalp, 1 involved the scalp and skull and 3 were within the limits of the skull. Six lesions exhibited malignant features. There were 101 trichilemmal cysts; 74 epidermal cysts; 38 intradermal nevus; 8 verruca vulgaris; -

Histopathology Squamous Cell Carcinoma
Squamous cell carcinoma - Mohs Ron Rapini MD No conflict of interest Josey Chair, Dept Dermatology • I am paid zero to speak at this Univ Texas Medical School at Houston MD Anderson Cancer Center course, other than travel • The tuition helps to run the ASMS programs Duplicate Actinic keratosis Actinic keratosis Rx • Whether you call it a “precancer” or • Treating orAKs is beyond this lecture “squamous cell carcinoma grade 1/2” or • Ill-defined dysplasias – usually a “field-effect” “SCC – AK type”, or “keratinocytic • Trying to eradicate totally is like playing intraepithelial neoplasia = KIN”, it still “whack a mole” so goal is to eradicate most doesn’t need Mohs surgery significant areas • Don’t over-read as invasive squamous cell ca • Cryo, curettage, laser, imiquimod, • AK and squamous cell carcinoma are often fluorouracil, diclofenac, etc multifocal with field effects in margins Keratinocytic intraepithelialDistribute Grading dysplasia in neoplasia = KIN 1, 2, 3 dysplastic nevi is analogous • Analogous to CIN, PIN, VIN 1,2,3 • Really in SKIN with most popular • NIH consensus conference 1992 system, we don’t have a “2”: recommended grading cytology despite Not lack of concordance AK = KIN-1 • I grade only cytology as mild, moderate, SCC in situ (Bowen’s) = KIN-3 Do severe 1 Lack of concordance on grading “dysplasia” in dysplastic nevi Other terms Piepkorn (J Cutan Pathol 6:542, 1992) • Bowenoid AK – “just call it found only 38% agreement SCCis?” Similar situation with KIN-2 (in between • Advanced AK – “beware” AK and SCC in situ) – -

12 IJBMRF20131339 Dr Sindhoori Komma
Int J Biol Med Res. 2013; 4(4): 3707-3709 Int J Biol Med Res www.biomedscidirect.com Volume 3, Issue 1, Jan 2012 Contents lists available at BioMedSciDirect Publications International Journal of Biological & Medical Research BioMedSciDirect Journal homepage: www.biomedscidirect.com International Journal of Publications BIOLOGICAL AND MEDICAL RESEARCH Case Report An Interesting Case Of Proliferating Trichilemmal Cysts And Lipoma Of The Scalp Sindhoori .K*a, Kishore Kumar B.N b, Prem Sai Reddy.B c, Sreeramulu.P Nd, Udaya Kumar.Me. aPost graduate department of Radiology, Sri Devaraj Urs Medical College, Kolar, Karnataka.pin code-563101 bProf and HOD, Radiology, Sri Devaraj Urs Medical College, Kolar, Karnataka.563101 cPost graduate, Radiology, Sri Devaraj Urs Medical College, Kolar, Karnataka.563101 dProf and unit chief, Surgery, Sri Devaraj Urs Medical College, Kolar, Karnataka.563101 eProfessor, Pathology, Sri Devaraj Urs Medical College, Kolar, Karnataka.563101 A R T I C L E I N F O A B S T R A C T Keywords: A 60 year old male patient presented with multiple slow growing lesions on scalp for past Trichilemmal cysts 25years. Patient was evaluated with radiographs and computed tomography (CT). Patient Radiographs underwent simple excision of the lesions and the diagnosis was confirmed on histopathology as Computed tomography proliferating trichilemmal cysts and lipoma of the scalp. KEY WORDS: Lipoma CTscan. c Copyright 2010 BioMedSciDirect Publications IJBMR -ISSN: 0976:6685. All rights reserved. 1. Introduction Proliferating trichilemmal cysts(PTCs) also known as pilar Figure 1- photograph of patients scalp with multiple soft cyst is a benign adnexal tumor of skin, related to the isthmus of the tissue swelling hair follicle1. -
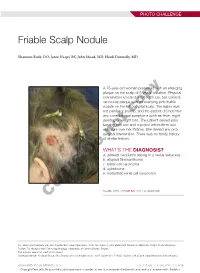
Friable Scalp Nodule
PHOTO CHALLENGE Friable Scalp Nodule Shannon Buck, DO; Jaree Naqvi, BS; John Moad, MD; Heidi Donnelly, MD A 75-year-old woman presented with an enlarging plaque on the scalp of 5 years’ duration. Physical examination revealed a 5.6×2.9-cm, tan-colored, verrucous plaque with an overlying pink friable nodule on the left occipital scalp. The lesion was not painful or pruritic,copy and the patient did not have any constitutional symptoms such as fever, night sweats, or weight loss. The patient denied prior tanning bed use and reported intermittent sun exposure over her lifetime. She denied any prior surgicalnot intervention. There was no family history of similar lesions. WHAT’S THE DIAGNOSIS? Doa. adnexal neoplasm arising in a nevus sebaceus b. atypical fibroxanthoma c. basal cell carcinoma d. cylindroma e. metastatic renal cell carcinoma CUTIS PLEASE TURN TO PAGE E20 FOR THE DIAGNOSIS Drs. Buck and Donnelly are from Dayton Skin Care Specialists, Ohio. Mr. Naqvi is from Boonshoft School of Medicine, Wright State University, Dayton. Dr. Moad is from Dermatopathology Laboratory of Central States, Dayton. The authors report no conflict of interest. Correspondence: Shannon Buck, DO, Dayton Skin Care Specialists, 3025 Governor’s Pl Blvd, Dayton, OH 45409 ([email protected]). WWW.MDEDGE.COM/DERMATOLOGY VOL. 105 NO. 1 I JANUARY 2020 E19 Copyright Cutis 2020. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. PHOTO CHALLENGE DISCUSSION THE DIAGNOSIS: Adnexal Neoplasm Arising in a Nevus Sebaceus iopsy of the lesion showed a proliferation of basa- secondary neoplasms, 88% of which were benign.2 The loid-appearing cells with focal ductal differentiation origins of these neoplasms can be epithelial, sebaceous, Band ulceration consistent with poroma (Figure 1).