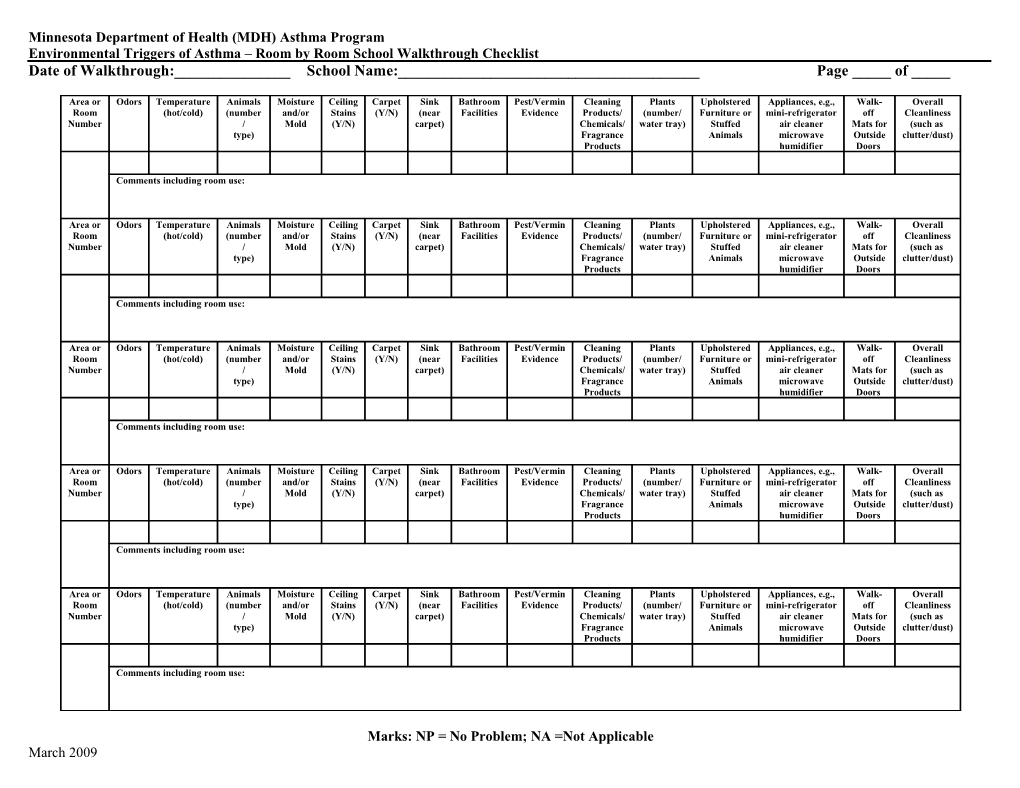
Minnesota Department of Health (MDH) Asthma Program Environmental Triggers of Asthma – Room by Room School Walkthrough Checklist Date of Walkthrough:______School Name:______Page _____ of _____
Area or Odors Temperature Animals Moisture Ceiling Carpet Sink Bathroom Pest/Vermin Cleaning Plants Upholstered Appliances, e.g., Walk- Overall Room (hot/cold) (number and/or Stains (Y/N) (near Facilities Evidence Products/ (number/ Furniture or mini-refrigerator off Cleanliness Number / Mold (Y/N) carpet) Chemicals/ water tray) Stuffed air cleaner Mats for (such as type) Fragrance Animals microwave Outside clutter/dust) Products humidifier Doors
Comments including room use:
Area or Odors Temperature Animals Moisture Ceiling Carpet Sink Bathroom Pest/Vermin Cleaning Plants Upholstered Appliances, e.g., Walk- Overall Room (hot/cold) (number and/or Stains (Y/N) (near Facilities Evidence Products/ (number/ Furniture or mini-refrigerator off Cleanliness Number / Mold (Y/N) carpet) Chemicals/ water tray) Stuffed air cleaner Mats for (such as type) Fragrance Animals microwave Outside clutter/dust) Products humidifier Doors
Comments including room use:
Area or Odors Temperature Animals Moisture Ceiling Carpet Sink Bathroom Pest/Vermin Cleaning Plants Upholstered Appliances, e.g., Walk- Overall Room (hot/cold) (number and/or Stains (Y/N) (near Facilities Evidence Products/ (number/ Furniture or mini-refrigerator off Cleanliness Number / Mold (Y/N) carpet) Chemicals/ water tray) Stuffed air cleaner Mats for (such as type) Fragrance Animals microwave Outside clutter/dust) Products humidifier Doors
Comments including room use:
Area or Odors Temperature Animals Moisture Ceiling Carpet Sink Bathroom Pest/Vermin Cleaning Plants Upholstered Appliances, e.g., Walk- Overall Room (hot/cold) (number and/or Stains (Y/N) (near Facilities Evidence Products/ (number/ Furniture or mini-refrigerator off Cleanliness Number / Mold (Y/N) carpet) Chemicals/ water tray) Stuffed air cleaner Mats for (such as type) Fragrance Animals microwave Outside clutter/dust) Products humidifier Doors
Comments including room use:
Area or Odors Temperature Animals Moisture Ceiling Carpet Sink Bathroom Pest/Vermin Cleaning Plants Upholstered Appliances, e.g., Walk- Overall Room (hot/cold) (number and/or Stains (Y/N) (near Facilities Evidence Products/ (number/ Furniture or mini-refrigerator off Cleanliness Number / Mold (Y/N) carpet) Chemicals/ water tray) Stuffed air cleaner Mats for (such as type) Fragrance Animals microwave Outside clutter/dust) Products humidifier Doors
Comments including room use:
Marks: NP = No Problem; NA =Not Applicable March 2009 How to Complete the MDH Asthma Program Room by Room School Walkthrough Checklist*
Odors: Does the room have a noticeable odor including food, mold and fragrances (Y/N)? Record the type of odor.
Temperature: Is the room too hot or cold?
Animals: Does the classroom have animals? If yes, record the type of animal and how many. Is the cage or habitat well maintained? If fish are kept in the room, is the tank near or on carpeting or another porous material?
Moisture/Mold: Does the room have visible mold or a noticeable mold odor (Y/N)? Record the location of the mold.
Ceiling Stains: Does the ceiling have water stains (Y/N)? If yes, record the approximate number and size.
Carpet: Is the room carpeted (Y/N)?
Sink: Does the room have a sink (Y/N)? If yes, is the sink located near carpeting or other porous materials?
Bathroom: Does the room have bathroom facilities (Y/N)? If yes, is the bathroom clean? Is there a noticeable odor?
Pests: Is there evidence of mice, cockroaches, ants, flies or other pests (Y/N)? What type of pest? Do you see traps or baits?
Cleaning Products/Chemicals/Fragrance Products: Do you see cleaning products/chemicals/scented products (Y/N)? Is yes, are they district purchased or approved. Scented products include air fresheners, diffusion sticks, and scented candles.
Plants: Are live plants in the room (Y/N)? If yes, how many and does each container have a solid bottom or tray to catch water.
Upholstered Furniture/Stuffed Animals: Do you see upholstered furniture, pillows, throw rugs or stuffed animals (Y/N)? If yes, record the type and number.
Appliances: Does the room have appliances such as mini-refrigerators, portable air cleaners, microwaves, or humidifiers (Y/N)? If yes, record the type and number. Also record if the appliance is located on or near carpeting.
Walk-off Mats: If the room has an outside door, is there a walk-off mat?
Cleanliness: Is there excessive clutter or dust in the room (Y/N)? If yes, record whether it is clutter, dust or both and the location.
*The emphasis is on issues with a low to no cost solution. For more information on the MDH Asthma Program school walkthrough project including a summary fact sheet, a sample reporting form and the walkthrough forms, go to http://www.health.state.mn.us/asthma/schools.html.
March 2009