Item 7.8 Highland and Island General Practice Specialty Training Programme Out of Hours Guidance Document.
April 2011
1 Background and recent changes to OOH training arrangements in the Highlands and Islands Programme
2 National Guidance Papers
3 Expectations on GPSTs
4 Expectations on Educational Supervisors and Clinical Supervisors in OOH
1 Background and recent changes to OOH training arrangements.
There have been a number of changes in the Out of Hours (OOH) provision for General Practice Specialty Trainees (GPST) in the Highlands and Islands (H and I) programme over the past two years.
Recent (COGPED) Committee of General Practice Education Directors and RCGP guidance has highlighted the importance of this part of GPST training and the importance of appropriate arrangements, supervision and competency demonstration for the safety of both patients and trainees.
Both COGPED and the RCGP have re-affirmed the necessity of demonstrating OOH competency as a pre-requisite for the Certificate of Completion of Training CCT.
Since the commencement of the new training arrangements in 2007 , a number of different models of OOH provision have existed for GPSTs in the H and I programme. These reflect our geographical challenges and the different methods of providing OOH in response to the GP contract, which allows most GPs and GP trainers to opt out of formal responsibility to provide OOH cover.
Currently these models include:
1 The traditional model of GPST accessing OOH with an individual Educational Supervisor (ES) (previously known as GP Trainer) and GP colleagues from a training practice providing clinical supervision. The ES, if appropriate, confirms and signs off the OOHs competency for the GPST.
2 The commonest current model where the GPST accesses OOH within a Primary Care Emergency Centre (PCEC). During these OOHs shifts the GPST has clinical supervision not only by partners or salaried doctors from their host practice but also by GPs from other practices and from employed GPs from the OOH Service. Increasingly, OOH doctors who are not associated with training practices are undertaking formal training in clinical supervision through locally delivered Supporting Clinicians on Training in Scotland (SCOTS) courses.
The Educational Supervisor retains the responsibility to sign off the GPST ’s OOH competence. This requires the ES to liaise with the Clinical supervisors to confirm competence in conjunction with their own knowledge of the GPST’s work undertaken during regular hours.
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 3 Within Inverness and some surrounding practices the GPST’s access OOH through the Integrated Emergency Department which includes GP OOH and Accident and Emergency services. In this setting, the clinical supervision is provided by Emergency Practitioners (EPs) who are dual trained in GP and Accident and Emergency. All the EPs currently providing clinical supervision have been trained through the SCOTS courses.
These arrangements have applied to GPST1’s and GPST3’s, except in the Inverness and surrounding area where the Integrated Department have not been able to provide the clinical supervision requirements for GPST1’s.
The original models remain but two recent changes have occurred.
4 Since August 2010 Some GPSTs from the Inverness and surrounding areas have been able to access OOH through the newly formed East Highland Out of Hours service. This service resembles a more traditional GP cooperative model where a number of practices have formally returned to providing a GP OOH service in conjunction with Highland Health Board. In 2010, four GPSTs undertook their OOH commitments through this method. In distinction to other GPSTs they may not have had any of their host training practice doctors working within the OOH service.
All the doctors within East Highland PCEC providing clinical supervision roles have undertaken the SCOTS course.
The host training practice Educational Supervisor, in conjunction with the OOH CS, remains responsible for OOH competency sign off for the individual GPST.
5 From August 2011, GPST1s from the Inverness and surrounding area will gain some access to OOH experience. GPST1 in this setting will be expected to undertake the following as a minimum during their six month post in general practice - One six hour OOH shift in Scottish Ambulance Service triage centre in Inverness. - One six hour OOH shift in NHS 24 Hub in Inverness. - One (or if possible two) six hour OOH shift in East Highland OOH PCEC.
Clinical supervision in the East Highland OOH shifts will be provided by trained CS.
Most of this experience is likely to be in a supernumery capacity for the GPST1, in view of the unfamiliarity of the clinical setting and lack of continuity of involvement, but where clinical service delivery can be safely delivered through the combined judgement of the clinical supervisor and the GPST this will be encouraged.
2 National Guidance Documents in OOH Training
There are two recent relevant papers for Guidance:
1 COGPED Out of Hours (OOH) Training for GP Specialty Registrars Revised Position Paper 2010.
2 RCGP Review of Out of Hours (OOH) Training for GP Specialty Trainees. 2011.
It is important that all Highland and Islands GPSTs and their Educational Supervisors familiarise themselves with both these documents and their requirements.
Link to full COGPED document http://www.cogped.org.uk/document_store/1286375694vGnm_out_of_hours_position_paper_(revis ed_2010).doc
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
Review Out-of-Hours (OOH) Training for GP Specialty Trainees By the RCGP January 2011.
Appendix 1 also available on Moodle GPST and Educational Supervisor sites
I would like to highlight a number of paragraphs from the recent RCGP review and ask for GPSTs and Educational supervisors to ensure that they reflect their current practice.
Royal College of General Practitioners Review Out-of-Hours (OOH) Training for GP Specialty Trainees
1. Executive Summary
“Out-of-hours services present a high risk to both patients and staff. All parties involved in the provision and purchase of out-of-hours services need to ensure that there are sufficient suitably trained and experienced clinical staff, particularly doctors, engaged in planning and delivering these services.”1
2.4 The key out-of-hours competences and their assessment
2.4.1 To obtain their CCT, trainees should demonstrate the six generic competences embedded within the RCGP Curriculum 7 on ‘Care of Acutely Ill People in the provision of OOH care”. These competences are defined as the:2
1. Ability to manage common medical, surgical and psychiatric emergencies in the out-of- hours setting.
2. Understanding of the organisational aspects of NHS out-of-hours care.
3. Ability to make appropriate referrals to hospitals and other professionals in the out-of-hours setting.
4. Demonstration of communication skills required for out-of-hours care.
5. Individual personal time and stress management.
6. Maintenance of personal security and awareness and management of the security risks to others
2.4.2 As a core part of achieving these competences, and thus their Certificate of Completion of Training (CCT), trainees must undertake sessions in an OOH environment. The overall responsibility for the assessment of competences is with the Educational Supervisor but trainees have a duty to keep the record of their experience and to provide reflection and feedback in their ePortfolio.
3 Expectations on GPSTs
GPST3 - GPST3 Trainees in a GP practice need to undertake a minimum of 72 hours Out-of-Hours over the year (or 36 hours in six months). However, you may need to do more in order to achieve your out-of-hours competencies. (This will probably depend on the intensity of workload during the shift).
1 2 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 - Out of hours training is currently an essential part of your GP training without which you cannot qualify. Your educational supervisor takes responsibility for signing you off as competent. However your supervision during shifts can take place in a number of different ways. You should always know who your GP clinical supervisor is during your shift. Initially they will be onsite with you. After a period of usually around three to six months they are then contactable by phone.
- In most areas there are local arrangements for trainees to engage with the OOH service with GPs providing clinical supervision.
- It is the GPST3s responsibility to organise shifts within their local OOH Provision.
- For GPST 3s based in and around the Inverness area, arrangements are in place to undertake your OOH commitments either in the Integrated Accident and Emergency and GP Out of Hours Service in Raigmore Hospital Inverness or alternatively in the East Highland OOH service based in Dingwall and Invergordon.
In both sites trained Clinical Supervisors will be available.
Details of individual GPST’s arrangements can be obtained from Lorna McDermott. Information on East Highland OOH arrangements can be obtained from Dr Gail Haddock. [email protected] [email protected]
GPTS1
Are contracted to provide 36 hours OOH work during the six months in general practice post.
The recent developments mentioned in 5 above seek to address this contractual requirement, fully recognising that at present we are unable to accommodate the full 36 hours commitment within the Inverness and surrounding area. It is the GPST1s responsibility to organise shifts within the local OOH provision. Any enquiries about the new GPST1 OOH arrangements can be directed to Dr Arun Sharma GP Associate Adviser [email protected]
It is essential that OOH learning experiences are documented within the eportfolio and ,as suggested in the COGPED paper, it seems likely that the RCGP Certification Unit will expect an increasing quality of the OOH competency documentation, currently assessed by the Deanery ARCP panel.
4 Expectations on Educational Supervisors
- as part of their initial educational planning with the GPST ,Educational Supervisors should ensure that appropriate arrangements are in place, for their GPST to complete sessions with the OOH service. The Trainer should ensure that the GPST understands and is informed of the range of learning environments and local opportunities for developing the required competencies.
- Sessions should take place at a time agreed by the trainer and GPST, following a clear evaluation of the GPST’s skills and competencies and learning needs. Normally this evaluation would take place within the first month in GP, during which time the GPST will have been fully inducted into the practice.
It is unlikely to be advisable for GPStRs to undertake any sessions with the OOH provider during this time.
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
- GP Educational Supervisors should ensure that their GPST undertakes an induction to OOH prior to starting.
Most OOH providers now provide a formal induction to GPSTs to allow familiarisation with staff, processes and equipment. This is not only good practice, but is now essential. In addition, the learning set in the local GP Training Programme (‘half-day release’) may also cover important local aspects and the Deanery may run courses for GPSTs, such as OOH communication skills and telephone triage.
- GP Educational Supervisors should ensure that they debrief their GPST following their OOH session and assess not only their learning, and further areas for development, but also the quality of the experience of the OOH session provided to the GPR.
- GP Educational Supervisors should regularly re-evaluate the level of supervision required by the GPST and confirm this with the OOH provider. This will be dependent on the learning environment but the following structure is suggested:
Direct Supervision - the GPST is supervised directly by the Clinical Supervisor [red] and takes no clinical responsibility.
Close Supervision - the GPST consults independently but with the Clinical [amber] Supervisor close at hand e.g. in the same building.
Remote Supervision - the GPST consults independently and remotely from the Clinical Supervisor, who is available by telephone. An example of such a session would include a session ‘in the ‘car’ supervised by another GP ‘at base’ or telephone supervision from a GP based at home. [green]
- It is good practice, carried out by a number of OOH providers, to have a process of formal communication between the GP Educational Supervisor and the OOH provider organisation to facilitate the move into amber or green shifts for the GPST. Educational Supervisors should, review the portfolio on a regular basis with the GPStR and, taking into consideration other feedback from Clinical Supervisors, validate competencies that have been achieved.
Please direct any enquiries concerning the Highlands and Islands OOH Guidance Document to:
Jerry O’Rourke Assistant Director Postgraduate General Practice Education
Jerry.O’[email protected] 01463 255734
April 2011
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
Royal College of General Practitioners Review Out-of-Hours (OOH) Training for GP Specialty Trainees
1. Executive Summary
“Out-of-hours services present a high risk to both patients and staff. All parties involved in the provision and purchase of out-of-hours services need to ensure that there are sufficient suitably trained and experienced clinical staff, particularly doctors, engaged in planning and delivering these services.”3
1.1 A high quality care out-of-hours (OOH) service is important in terms of patient safety and for reducing unnecessary admittance to secondary care and delivering a cost effective NHS. To ensure the OOH service continues to give all users, including patients and carers a high quality service the future workforce needs to be confident and competent in its delivery of OOH Care.
1.2 General Practice Specialty Trainees are required to spend time working in the out-of-hours environment to achieve their training competences in urgent care (Curriculum Statement 7: Care of Acutely Ill People). The Royal College of General Practitioners (RCGP) believes that attainment of these competences will ensure that trainees have demonstrated the necessary skills, knowledge and ability to provide OOH care. We believe that trainees derive enormous benefit from their OOH sessions and gain additional experience of managing patients with urgent and emergency care needs, risk management, isolated working and working with unfamiliar patients and in unfamiliar settings with consultations on the telephone and face to face with other team members. These sessions generally take place outside of their familiar training practice and need to be in environments which are high quality and accredited. These should be environments which will develop the trainee’s knowledge and skills, allowing them to reflect and receive feedback on their work, and which will support them in becoming fit for independent practice as general practitioners who are enabled to work in urgent care services out-of-hours.
1.3 The contractual changes introduced in April 2004 have enabled many GPs to transfer responsibility for the provision of out-of-hours care for their patients to their local commissioning organisation. The majority of trainers are not engaged in working or training out-of-hours, and their trainees undertake their OOH sessions for OOH providers, often under the supervision of a Clinical Supervisor who may not have achieved trainer competences. The provision and implementation of OOH training can, therefore, be more complex and subject to greater variation in quality and availability than in-hours training. High quality training is important because many GPs, once qualified, provide OOH services. If newly qualified GPs are both confident and competent practitioners the risk to patient safety is reduced and it is likely that they will refer to secondary care, and make use of other services, more appropriately. Furthermore, if GP trainees have an encouraging and positive experience of OOH provision during their training they may regard working in OOH as an attractive longer-term prospect, thus contributing to the available OOH GP workforce in the future.
1.4 There have been anecdotal reports that training in OOH is not universally fit-for-purpose and that trainees’ experiences are of variable quality across the UK. One of the recommendations from Steve Field and David Colin-Thomé’s 2010 report -General Practice Out-of-hours Services: Project
3 CQC, Investigation into Out-of-hours services provide by Take Care Now – Summary, July 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 to consider and assess current arrangements is that the RCGP should examine the provision and delivery of OOH training in greater detail.4 In August 2010 a national RCGP Advisory Group, which included representatives from RCGP, Committee of General Practice Education Directors’ (COGPED) and the British Medical Association (BMA), was formed to review this system. A number of Advisory Group members were also involved in formulating the COGPED Position Statement on General Practice Specialty Out-of-hours Training. This COGPED report, which reviews the current OOH training arrangements, was supported by both BMA and RCGP and provides guidance for the different groups and organisations involved in GP Training in the OOH system.
1.5 This review has found that the main issue to be addressed is the inconsistent implementation of the COGPED guidance on the OOH training of GP trainees (appendix 2). The RCGP, therefore, wishes to make recommendations to support and strengthen the COGPED guidance and encourage the tightening up of the quality management process. This review supports the position that any trainee who is not up to standard, and does not attain the competences described in the framework, despite being competent in other areas, should not proceed to a Certificate of Completion of Training (CCT) unless these areas can be addressed.
1.6 At this current time, when the NHS is in the process of great change, we feel the emphasis should be on improving the quality of OOH training overall rather than on just increasing the number of sessions. This is the current position of the COGPED guidance on the number of sessions:
The number of sessions worked by a GP StR to acquire the necessary competencies is likely to be directly related to the quantity of individual patient contacts, and thus the level of workload, provided by a routine OOH shift, in an urban setting, this is likely to require an indicative benchmark of a four to six hour session every four weeks adjusted in other settings on a pro rata basis. 5‘
1.7 This review supports the COGPED guidance as stated above.
Summary of Recommendations The review recommends that:
1. the COGPED Position Statement must be implemented consistently across the UK
2. appropriate emphasis should be placed on OOH within the curriculum and assessment process, including Workplace Based Assessment.
3. educational resources are developed to support OOH and urgent care.
4. the Annual GMC Trainee Survey should consider questions relating to both the in- hours and out-of-hours trainee experience.
5. every GP Trainer needs to ensure that they are familiar with ways in which their trainee will obtain their OOH competences.
6. Clinical Supervisors (who are currently not GP Trainers) must receive mandatory training, which should be agreed and provided by their deanery.
7. OOH providers must ensure there is an agreed minimum number of Clinical Supervisors and supervised sessions available to GP trainees. This to be agreed with the local Commissioning Organisation and Deanery.
4 General Practice: Out-of-hours services Project to Consider and assess current arrangements for the provision of out- of-hours care, Steve Field and David Colin-Thomé’, 2010 5 COGPED, Position Statement on General Practice Specialty Out-of-hours Training, Revised version 2010
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 8. OOH providers will continue to have responsibility for the clinical governance and continuing professional development of their staff and may commission support from Deaneries as appropriate.
9. OOH providers must demonstrate that they have acted on feedback received from their GP trainees and are able to share this with the Deanery.
10. the relevant national regulator, as part of its quality assurance of service provision in Primary Care will, when assessing OOH providers, include an assessment of the quality of the educational governance undertaken by that provider in relation to GP trainees.
11. commissioning organisations should ensure that recommendation eight is implemented.
12 organisations responsible for commissioning OOH provision should ensure that requirements for the provision of sessions for GP trainees and the provision, training and continued professional support of Clinical Supervisors are appropriately resourced, and clearly identifiable ring-fenced funding for training is firmly monitored within the OOH budget .
13. it is reaffirmed that it is the role of deaneries to provide training for doctors (who are not previously accredited as GP Trainers) and other appropriate health care professionals to be Clinical Supervisors. This will facilitate the implementation of recommendation six.
14. as part of their quality management process, deaneries should regularly review the provision of OOH training provided to their cohort of GP trainees in line with that applied to other Local Education Providers.
15. as part of their quality management process deaneries should ensure assessors of OOH providers are familiar with OOH. In addition to this deaneries should train those assessors to be systematic and consistent, and to use a common reporting template to produce a report which will be shared with the commissioning organisations.
16. the GMC should be explicit that when it is approving GP Training in a particular deanery they are also approving the totality of training locations including the OOH training component in that training programme.
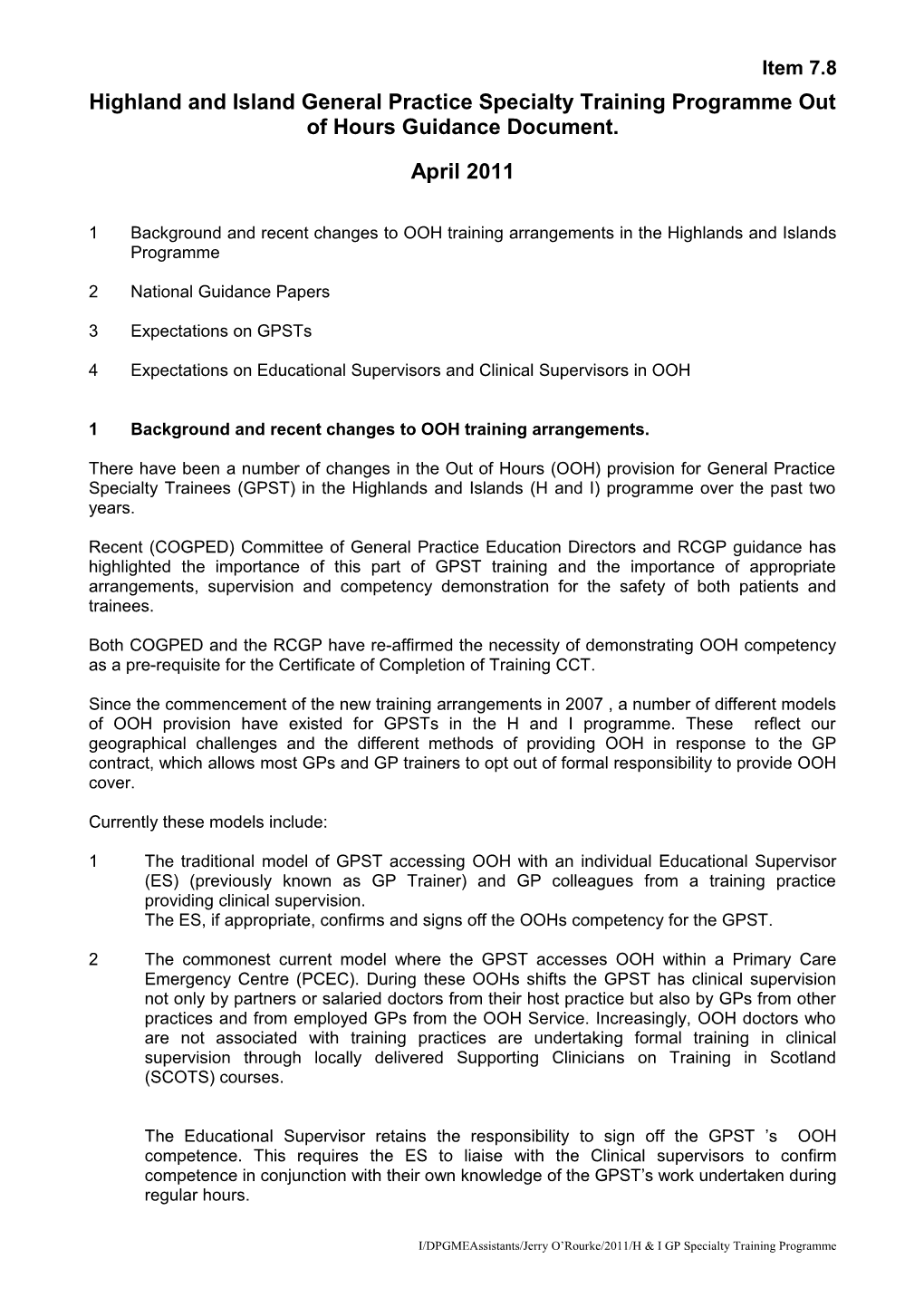
Fig.1 Governance of training delivered within the out-of-hours system
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
Relevant national quality regulator GMC: Approves training posts for e.g. CQC for England: Assures the GP Specialty Training by applying quality of service provision. All OOH their quality assurance framework. providers have to meet standards set by the national Regulator
Local Deaneries: Quality manage training, implementing a quality management framework to meet standards set by the GMC for general practice Specialty Training
Local Education Provider e.g. Out- of-Hours Provider: Quality controls training by ensuring that a set of standards, procedures and policies are in place to deliver the standard of service required
2. Introduction 2.1 Out-of-hours (OOH) is defined as work undertaken between 18.30-08.00, and all day at weekends and on public holidays, for urgent and unscheduled patient contacts. There are a number of organisations involved in the delivery of OOH and unscheduled care services, including GP co- operatives, commercial services, NHS Direct, NHS 24, nurse triage, urgent walk-in-centres, GPs embedded within A&E departments and some practices and practitioners who continue to provide cover for their practice patients OOH care.
2.2 The Government undertook to increase the amount of time during the day that GPs were available to patients and balloted GPs in March 2008. As a result of this, GPs, via the General Practitioners Committee (GPC) agreed to provide ‘extended hours’ under a local or directly enhanced service contract. This allowed GP practices to provide NHS services in the early morning, in the evening and at weekends. In the majority of cases, this has provided additional surgery services for non- urgent pre-booked patient contacts. OOH does not include any experience gained in the GP training practice during extended hours
2.3 The provision of care OOH requires GPs to manage patients with urgent and emergency care needs, manage risk, work in isolated situations and with unfamiliar patients. In addition, consultations may be by telephone or face to face and may be in settings, and involve other team members, that are not familiar. GPs must also be aware that the needs of patients, their families and carers may also be different in an OOH situation. It is for this reason that training GPs to provide care OOH, and to attain the competencies described in Curriculum Statement 7, is so important.
2.1 Background 2.1.1 In January 2010 the Committee of General Practice Education Directors (COGPED) revised its Position Statement on General Practice Specialty out-of-hours Training (appendix 2).
2.1.2 This report acts as guidance on the way in which General Practice Specialty Trainees should gain experience in out-of-hours care (OOH). This report does not attempt to re-write the recent COGPED position statement, but rather intends to act as a supportive document which will sit alongside it. It should be read in conjunction with the COGPED report as much of the extensive detail and background on the provision of OOH can be found there (see appendix 2).
This review recommends that:
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 1. the COGPED Position Statement must be implemented consistently across the UK
2.2 Reason for review 2.2.1 The request for this review arose from a report by David Colin-Thomé, National Primary Care Director and Steve Field, Chair of the Royal College of General Practitioners on the provision of out-of hours services. This review was published in January 2010 and was prompted by the tragic death of a patient who was administered 100mg of diamorphine by an OOH sessional doctor who was trained outside the UK, and worked during the day out of the UK. The report made several recommendations including that:
The RCGP should review the guidance concerning GP Registrars’ training on out-of-hours and should update this as necessary. This work should involve engagement with the necessary stakeholders including COGPED.6
2.2.2 Following this recommendation, the RCGP received a request from Dr Patricia Hamilton, in her capacity as Director of Medical Education (England) for the Department of Health, that it should lead this review, and work closely with COGPED.
2.2.3 The objective of this review is to examine whether: the Competency Framework is fit for purpose; the current arrangements for OOH training are satisfactorily delivered; there is enough training to produce newly qualified GPs which are competent and suitably confident to provide out-of-hours services.
2.3 Review Process 2.3.1 A group was established to undertake the review and it incorporated key stakeholder views, including representatives from BMA, COGPED, RCGP and the RCGP Patient Partnership Group (appendix 3). To ensure that the review was fully informed about the current OOH training situation across the UK COGPED representation from across the devolved nations was also included.
2.3.2 To gain a more robust evidence base for our conclusions a survey was circulated to PCT Medical Directors, deaneries and OOH providers. This survey asked questions related to the provision of OOH opportunities for GP trainees, the systems in place for monitoring this quality and the competence and confidence of trainees once they qualify.
2.3.3 Due to the nature of the survey, and the short timeframe in which it was delivered, it must be noted that this survey provides only a snapshot view and, therefore, has some limitations as an evidence base. However, nearly all GP Deanery Directors replied and we received over 16 commissioning organisations and 15 OOH providers responses from across the UK, from both rural and urban areas. Within this survey there was enough commonality of opinion from each of the groups to show themes and express consistent points of view. Many of the comments expressed concerns, especially regarding the other groups’ roles in the teaching of OOH competences. These comments were useful to develop themes, issues and recommendations which have been incorporated under the headings within the report below.
2.3.4 The feedback and anecdotal evidence from the review group showed a wide variation of the provision and implementation of OOH Training across the UK. The aim of the recommendations is to attempt to standardise trainees’ experiences so that they are ensured training of equal quality. The delivery of quality training should ensure that trainees are achieving the competences as listed below.
2.4 The key out-of-hours competences and their assessment
6 Field and Colin-Thome, General Practice: Out-of-hours Services. Feb 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
2.4.1 To obtain their CCT, trainees should demonstrate the six generic competences embedded within the RCGP Curriculum 7 on ‘Care of Acutely Ill People in the provision of OOH care. These competences are defined as the:7
1. Ability to manage common medical, surgical and psychiatric emergencies in the out-of- hours setting.
2. Understanding of the organisational aspects of NHS out-of-hours care.
3. Ability to make appropriate referrals to hospitals and other professionals in the out-of-hours setting.
4. Demonstration of communication skills required for out-of-hours care.
5. Individual personal time and stress management.
6. Maintenance of personal security and awareness and management of the security risks to others
2.4.2 As a core part of achieving these competences, and thus their Certificate of Completion of Training (CCT), trainees must undertake sessions in an OOH environment. The overall responsibility for the assessment of competences is with the Educational Supervisor but trainees have a duty to keep the record of their experience and to provide reflection and feedback in their ePortfolio.
2.4.3 This review believes that these competences fit the purpose for which they were designed, which is to deliver a GP who is able to deliver OOH Care proficiently and safely.
2.5 Number of Sessions
2.5.1 This review supports the COGPED guidance below in regard to the number of sessions GP trainees need to undertake to be deemed competent to provide OOH care.
2.5.2 This statement is applicable to whatever length of GP training is undertaken i.e. 12 or 18 months:
The number of sessions worked by a GP StR to acquire the necessary competencies is likely to be directly related to the quantity of individual patient contacts, and thus the level of workload, provided by a routine OOH shift, in an urban setting, this is likely to require an indicative benchmark of a four to six hour session every four weeks adjusted in other settings on a pro rata basis. 8‘
3. Trainees GPStRs should work in the OOH services, under supervision, in order to gain competence and confidence in the delivery of these services as a necessary part of becoming registered as GPs. The work of GP StRs in acquiring OOH competencies will be as part of their normal contract of employment.9
3.1 The length of General Practice Specialty Training is currently three years of which the RCGP recommends 18 months is spent in general practice placements. As a core part of their training programme GP trainees are expected to undertake sessions in OOH Care. The COGPED guidance outlines the responsibilities of trainees and suggests they are responsible, in conjunction with their trainer, for organising their sessions directly with OOH providers, ensuring that the required number of hours are achieved commensurate with the duration of the GP component of their training programme. Trainees have professional responsibilities as part of undertaking OOH 7 http://www.rcgp-curriculum.org.uk/pdf/curr_7_Acutely_ill_people.pdf 8 COGPED, Position Statement, 2010 9 COGPED, Position Statement, 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 training. For example, a trainee should be expected to introduce themselves to their Clinical Supervisor at the beginning of each session and discuss their OOH training needs with them.
3.2 The formal assessment of the GP trainee is the responsibility of the educational supervisor, who is usually their GP Trainer. This assessment is supported by documentation in the trainee’s ePortfolio, as well as feedback from the Clinical Supervisor. The type of evidence included in the ePortfolio includes the GP trainee’s reflection on their clinical encounters, professional conversations with their Clinical Supervisor or even submissions for formal case-based discussions. These are then signed off by their Educational Supervisor following further discussion and reflection. The COGPED guidance recommends the assessment of trainees across red, amber, green capability.
3.3 As stated above this review supports the current competency framework. However, further work could be undertaken to ensure that OOH training is promoted and GP trainees are supported adequately. The RCGP should place more emphasis where appropriate on OOH within the Curriculum and within the assessment process, including Workplace Based Assessment. There is also scope for developing educational resources for OOH and Urgent Care. These resources could include e-learning modules and deanery-approved courses.
3.4 The feedback from the trainee representatives involved in this review suggests there is significant variability in the OOH training experienced across the UK. It would appear that some regions follow COGPED guidance more closely than others. This situation is very complex and in many cases such variation arises as a result of differences in patient / provider / educational need. For example, some rural OOH services see relatively few patients which gives trainees the time to gain education from their mentors while, in contrast, suburban services are often overwhelmed and trainees can often feel as though they are an extra doctor. The responses in the Review Survey show that providers, particularly in urban environments, find that balancing the educational needs of trainees with the needs to see patients quickly and efficiently can be challenging.
3.5 In the past, GP trainees have often experienced difficulty in accessing OOH sessions. However, the feedback from the survey, particularly from the deaneries, suggests that this seems to be improving. This may be due to OOH providers adjusting to the increase in trainee numbers with the introduction of 18 month GP placements. The issue does seem more likely to be that trainees may not get the sessions they would like and this could be due to slots being booked at the last minute or trainees attempting to fit them all in at the end of their ST3 year. To comply with COGPED guidance GP trainees are required to undertake an ’indicative benchmark of a four to six hour session every four weeks.’ However, there is anecdotal evidence that trainees are not able to achieve this for a variety of reasons. The benefit of having sessions at regular intervals across the 18 months of their GP placement is that trainees are better able to show learning progress.
3.6 One of the most successful methods of obtaining robust evidence about the quality of training is via trainee feedback. Some deaneries already undertake surveys of their trainees. This report supports using this method to discover the opportunities and experiences trainees have had and identify any areas that give cause for concern. However, increasingly trainees are being over- surveyed and may not be responsive to surveys. This report recommends that questions about out-of-hours experiences, in addition to in-hours, should be included in the GMC annual mandatory Survey of Postgraduate Trainees. This would provide more evidence-based conclusions regarding UK variation and how trainees view their OOH experiences.
3.7 A substantial number of GP trainees feel that acquiring 72 hours OOH experience per year can put them under additional pressure as the final ARCP takes place approximately two months before the end of training, so in fact they are seeking to undertake all of the required sessions within 10 months. However, normally ARCP panels will sign off trainees with outstanding sessions provided that the sessions have already been booked and the competences have been met. An added pressure for trainees is adhering to the European Working Time Directive (EWTD). The maximum period of work currently allowed is 13 hours and with a minimum rest of 11 hours. The definition of ‘work’ includes educational sessions as well as clinical ones. This means that if GP Registrars are to do out-of-hours sessions on weekdays, they may need to be given some of the morning off on
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 the day of, and the day after, the out-of-hours session. If a doctor is performing a night shift they should not be expected to work in the practice 11 hours before or after the shift. However, there have been several comments from the Associates in Training (AiT) Committee that trainees have not complied with EWTD, and have not wanted to ‘rock the boat.’ There is a strong feeling from GP trainees that training practices prefer them to undertake OOH in their study time or at the weekend rather than in sessions which would take time out of in-hours work. GP trainees should be encouraged to complete a mixed bag of sessions, including weekends, to gain a range of different experiences. Equally training practices have an obligation to their trainees and, ultimately, to patient safety, to ensure that GP Registrars reach the competences required to achieve a CCT. GP trainees, GP Trainers and GP training practices need to engage in OOH early in the GP training placement.
3.8 The recommendations within the review are focused on improving training with the aim to produce a confident and competent GP capable of working in the OOH environment. There is, arguably, a potential mismatch between what educators and society expect of newly qualified GPs and what their own intentions are. Currently, there are fewer younger GPs undertaking OOH. This review understands that the GP workforce is changing and this may impact on the future of newly qualified GPs entering OOH, for example the impact of the increasing feminisation of the workforce. If they enter OOH it is often only for a short time while they are finding permanent employment. To incentivise newly qualified GPs, as well as experienced GP Trainers, there need to be stronger incentives to participate in OOH services. This may go beyond the scope of this report but we would suggest that the Government and professional bodies should consider ways of supporting and encouraging participation in OOH by newly qualified and established GPs.
This review recommends that:
2. appropriate emphasis should be placed on OOH within the curriculum and assessment process, including Workplace Based Assessment.
3. educational resources are developed to support OOH and urgent care.
4. the Annual GMC Trainee Survey should consider questions relating to both the in- hours and out-of-hours trainee experience.
4. GP Trainers – Education Supervisor ‘GP Trainers undertake the overall educational supervision of the individual trainee’s learning experience; they manage the process, commission learning opportunities and are responsible for the delivery of formative assessment in the workplace and preparing the GP trainee for the other elements of the MRCGP examination. Other educators, such as Clinical Supervisors are expected to provide detailed information to inform these processes.10’
4.1 The COGPED report sets clear guidance as to what arrangements GP Trainers should put in place to support their trainees when training in OOH. Consistent feedback from GP Trainers suggests that the COGPED guidance has been an extremely useful tool. However qualitative evidence from the group and from the survey has indicated that the COGPED guidance is not always being followed consistently by all parties involved in implementing and delivering training. It is increasingly being reported that there is a growing disconnect between in-hours training and out-of hours training.
4.2 Since the 2004 GMS contract the majority of GPs have opted-out from providing cover OOHs, therefore the majority of GP Trainers have stopped working in out-of-hours services. The lack of exposure to OOH can mean that some GP Trainers have little detailed understanding of the
10 COGPED Position Statement I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 operation of OOH services or experience of working in a modern OOH service. In addition, they may sometimes be unaware of the OOH training situations and environments which will most effectively allow their trainee to achieve the required competences. This is important particularly as GP Trainers have to sign off trainees on competency two (see section 2.5). As educational supervisors, GP Trainers should be aware of local training opportunities which can deliver required competences; these might include undertaking a course in telephone triage, working in an OOH/ Walk in centre or undertaking home visits for an OOH service.
4.3 With fewer GP Trainers being involved in OOH care there is a risk that OOH may not be highlighted as important to trainees. Consequently, those trainees may not see urgent care and OOH as an important part of a generalist’s role. Anecdotal feedback has suggested that some GP Trainers may not always insist that their trainees undertake additional sessions to acquire necessary competences, particularly if their trainee does not intend to undertake OOH work in the future.
4.4 In their role as Educational Supervisors, GP Trainers are responsible for signing off their trainee as being competent in OOH as part of their final review. A GP trainee cannot, therefore, apply for their Certificate of Completion of Training (CCT) without the OOH competence being signed off. Trainees collect evidence of their OOH sessions in their ePortfolio, and the Educational Supervisor reviews this to decide if progress has been satisfactory. There are several options for strengthening the governance surrounding the signing off of OOH training. For example, deaneries could review their processes for Trainer accreditation and re-accreditation to ensure that trainers are sufficiently informed about OOH to be able to sign off competences. In addition, deaneries could periodically audit ePortfolios to ensure standards are being achieved.
4.5 It is recommended that all GP Trainers should take active steps to ensure that they retain current knowledge and understanding of OOH provision, the detail of its implementation, and the learning experience and challenge that it can provide. This report does not seek to prescribe how this knowledge should be obtained but suggests that trainers avail themselves of a number of learning opportunities as part of the deanery Training Development Programme, and their further CPD as a GP Trainer. One option might be for a Trainer to attend an appropriate OOH provider Induction Course with their trainee every few years.
4.1 Trainer Groups 4.1.1 To ensure that there is a joined up approach to training a stronger connection needs to be established between OOH and in-hours supervision and assessment. In many areas GP Trainers groups do not have any direct input or involvement in the training and assessment of GP trainees in OOH. A suggestion within this report is that GP Trainers groups’ agendas could include OOH training to ensure that this component of training remains a high priority area. Local trainers groups might also wish to meet or communicate with OOH providers at a time and frequency to be agreed in order to share significant events and audit results from the service, or be involved in auditing OOH trainee consultations.
This review recommends that:
5. every GP Trainer needs to ensure that they are familiar with ways in which their trainee will obtain their OOH competences.
5. Clinical Supervisors It is desirable for the clinical supervisor to have additional skills to that of being a proficient professional and these will include the ability to teach, observe, assess and feedback to learners.11
5.1 At its most basic, clinical supervision is a clinical governance issue ensuring the quality of care and patients’ safety.
11 COGPED, Position Statement, 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
5.2 The GMC definition of a Clinical Supervisor is: “A trainer who is selected and appropriately trained to be responsible for overseeing a specified trainee’s clinical work and providing constructive feedback during a training placement. Some training schemes appoint an educational supervisor for each placement. The roles of clinical and educational supervisor may then be merged.12”
5.3 The quality of OOH training is likely to be related to the quality of Clinical Supervision. Evidence suggests that the quality of training provided is related to the quality of patient care given by that organisation. Anecdotal evidence from trainees has shown that there is a variation in the quality of Clinical Supervisors, particularly for those who are not GP Trainers. Many OOH providers have shown a preference for GP Trainers to become Clinical Supervisors, however for various reasons many Clinical Supervisors in OOH are not GP Trainers. The review survey shows that there is a variation in the engagement of Clinical Supervisors in providing constructive feedback and working with the educational supervisor to assess the training level of the trainee. A suggestion within this report is that data concerning the performance of doctors who work for OOH could be provided as additional feedback to Educational Supervisors in order to support the educational development of their trainees.
5.4 To raise the quality of clinical supervision in OOH there needs to be mandatory training which is agreed and provided for by the deanery. Deaneries already provide training for Clinical Supervisors, but there may be a need for greater discussion by COGPED to decide a more uniform approach to training Clinical Supervisors in OOH to ensure a consistent standard. This training would need to be accredited and re-accredited by deaneries, and this should already be a part of the deaneries’ quality management process.
This review recommends that:
6. Clinical Supervisors (who are currently not GP Trainers) must receive mandatory training, which is agreed and provided by the deanery.
6. OOH Provider It is expected that services will follow care pathways and patient journey/s, delivered in multi-professional settings, which will include GPs, nurses, paramedics, and A&E staff etc. and will continue to develop models of care that reduce the burden of unscheduled admissions to secondary care.13
6.1 OOH providers can provide a wide range of training opportunities for GP trainees. However, due to the cost, capacity implications and the challenge of delivery, it can be difficult for providers to offer quality learning opportunities for trainees. OOH providers have to balance their educational responsibilities with the need to see patients quickly and efficiently. The additional pressure put on OOH providers in supporting GP Registrar training can be significant especially during periods of peak demands. This puts an increasing pressure upon the clinical and non-clinical staff working within the service. However, these unexpected situations, such as the H1N1 pandemic, may increase the burden on OOH services but they provide excellent training opportunities for the trainee.
6.2 The majority of the feedback we received from OOH providers showed they were fully engaged with delivering high quality training. It is difficult to analyse how objective or typical this feedback is, or whether the comments we received were only from OOH providers who were committed to fulfilling their obligations. The majority of OOH providers reported having little difficulty with
12 GMC – Quality Framework Operational Guide, April 2010 http://www.gmc-uk.org/Quality_Framework_Operational_Guide.pdf_31301293.pdf
13 COGPED Position Statement, 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 providing sessions. Any difficulty reported tended to be due to providing extra capacity with GP placement training expanding from 12 to 18 months.
6.3 The main issue with providing sessions is the availability of appropriate Clinical Supervisors. In some areas across the UK the recruitment of Clinical Supervisors has been reported as being extremely difficult. This report recommends that OOH providers need to agree minimum numbers of Clinical Supervisors for any given OOH provider to ensure that sessions are being delivered. This agreement would need to be made with the commissioning organisations and deanery and would ensure that locally-specific decisions were being made and all parties understand the challenges which face them. The feedback from deaneries is that trainees are more likely to have their training needs met when there is active communication not just between the Clinical Supervisor and the Educational Supervisor, but between representatives of each stakeholder.
6.4 A number of OOH providers have reported that they are improving their session capacity by forward planning and being creative. A substantial number are actively encouraging and canvassing interested OOH doctors to attend the Teaching OOH Course to become OOH supervisors. Another provider which was having difficulty with capacity and space has negotiated successfully with their local deanery to have two trainees per Clinical Supervisor who was also working a shift. These decisions need to be taken locally with the emphasis on ensuring a quality training experience for trainees.
6.5 OOH providers have a responsibility for the clinical governance of their staff, including Clinical Supervisors. They are ultimately responsible for ensuring patient safety is not compromised and that trainees are only put in situations which are appropriate to their need. OOH providers should routinely gain feedback from their trainees, and act on that feedback if necessary. One option could be for OOH providers to survey a particular cohort of trainees annually during sessions. The feedback could be used to improve the quality of the teaching sessions and could be shared with the deanery.
6.6 OOH providers should also invest in their workforce, including Clinical Supervisors, in a similar way to in-hours GP practices. If they wish to develop the CPD of Clinical Supervisors they should be able to commission support from deaneries as appropriate. It is extremely important for trainees to see high quality OOH Care and best practice as this is more likely to influence a continued interest in OOH care.
6.7 OOH providers, as employers, are the group most qualified to judge whether GPs once qualified are ready to be independent OOH practitioners. The statement below appears to sum up the response from OOH providers, and perhaps employers generally:
‘’Trainees vary in ability and confidence and that while many are excellent and ready to work, others are not ready to work autonomously.’’
6.8 Our survey of OOH providers has indicated that whilst the majority of newly qualified GPs are competent, many feel they are not confident. Some feedback suggests that inexperienced doctors struggle and lack confidence and refer too readily to A&E. Several OOH providers have a policy in place whereby they will not employ newly qualified GP’s and require them to have more experience. This seems to strongly relate to the results of the Extended GP Training Survey, which highlighted that newly qualified trainees believe they are competent but not always confident.14 The OOH environment is one in which GPs may be working in unfamiliar environments and have less support from their peers or the wider practice team, and so higher levels of confidence are needed OOH than in-hours, even in the competent doctor.
6.9 A substantial number of OOH GPs have commented that out-of-hours care provision should be a sub-specialty in its own right, with its own qualifications and diplomas. If the length of training was extended trainees would have greater opportunity to experience OOH and this increased exposure could allow GP trainees to begin to develop more specialised skills in this area.
14 RCGP Review of Specialty Training, January 2010 http://www.rcgp.org.uk/gp_training/extended_gp_specialty_training.aspx I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
This review recommends that:
7. OOH providers must ensure there is an agreed minimum number of Clinical Supervisors and supervised sessions available to GP trainees. This to be agreed with the local commissioning organisation and deanery.
8. OOH providers will continue to have responsibility for the clinical governance and continuing professional development of their staff and may commission support from deaneries as appropriate.
9. OOH providers must demonstrate that they are acting on feedback received from their GP trainees and are able to share this with the deanery.
7. National Quality Regulators
7.1 All providers of services to the NHS, including OOH providers, will need to be registered with the quality regulator. The UK regulators are Care Quality Commission in England (CQC), HealthCare Inspectorate (HIW) in Wales, Quality Improvement Scotland (QIS) in Scotland and the Regulation and Quality Improvement Authority (RQIA) in Northern Ireland. These regulators register and inspect a wide range of health and social care services, including OOH providers.
7.2 As part of the process of OOH providers being registered and reviewed the appropriate national regulator needs to look at the governance of GP training together with other aspects of quality and safety. There is a strong link between good clinical supervision and patient safety. OOH providers should recognise this as a marker of quality to include in their published ‘Quality Accounts’, This has the potential to be a lever to increase and improve OOH training opportunities to GP trainees.
This Review recommends that:
10. the relevant national regulator, as part of its quality assurance of service provision in Primary Care will, when assessing OOH providers, include an assessment of the quality of the educational governance undertaken by that provider in relation to GP trainees.
8. Commissioning Organisations ‘PCTs should review whether recruitment, induction and mentoring requirements for the out-of hours provider are set out adequately in their contract with the provider, and satisfy themselves that these are passed through to any sub-contractor or agency, which the provider engages.’15
8.1 Currently commissioning organisations, such as PCOs and Health Boards, are mandated to secure OOH services by commissioning from appropriate organisations or consortia of organisations or, less frequently, by direct provision. The Coalition government has just issued a White Paper – Equity and Excellence: Liberating the NHS: Department of Health. This paper proposes that the Government should abolish SHAs and PCOs and devolve power for commissioning services to health care professionals and providers.16 In the future Consortia of GP practices will be given the opportunity to commission OOH Care, and the recommendations in this report will be equally valid.
15 Field and Thome, Provision of Out-of-hours Report, 2010 16http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_117353
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 8.2 The COGPED guidance encourages commissioning organisations to work closely with the postgraduate deaneries to establish clinical and educational governance standards for training in OOH and to assure the quality of training in the OOH organisations. These commissioning organisations also need to discuss with their local GP postgraduate deanery the increase in OOH opportunities that are needed for GP trainees and take measures to ensure they can be delivered through current OOH arrangements. Comments from deaneries about the relationship with their commissioning organisations suggests that there are varying levels of engagement, and more partnership working on all sides is required to implement and deliver training.
8.3 Commissioning organisations have not always prioritised training as an aspect of OOH care. Deaneries are not always involved in this commissioning process. Our review survey suggested that some commissioning organisations are unclear that they are responsible for the clinical governance of out-of-hours GP Registrar training, whilst the deanery is responsible for the educational governance. There have been a number of comments from deaneries that commissioning organisations have changed contracts with OOH providers without involving them. This can leave deaneries to rearrange attachments and train new supervisors at short notice. World Class Commissioning required commissioning organisations to commission sustainable services, which means taking into account the need of the service to train and replenish its workforce.
8.4 In December 2009 a directional letter was sent to all PCT Chief Executives in England by Clare Chapman, the Department of Health’s Director for Workforce, to draw attention to PCTs’ responsibility to commission increased GP out-of-hours (OOH) training to reflect the extension of training undertaken in GP practices from 12 to 18 months. The purpose of the letter was to inform PCTs that capacity needs to increase by 50% as GP Directors had reported that this increase has not been realised. The action required from PCOs:
‘ PCTs will need to discuss with their local GP Postgraduate Deanery the increase in OOH opportunities that are needed for GP Registrars (GPRs) and take measures to ensure they can be delivered through arrangements currently in place to provide OOH services.’17.
8.5 There has been no letter in Scotland. Feedback has shown that some PCTs in England have ignored this directive. Others have negotiated with OOH provider to provide additional slots.
8.6 In commissioning and quality assuring OOH services the commissioning organisation needs to ensure that each OOH provider is able to provide the necessary training opportunities, has a sufficient number of trained Clinical Supervisors in their organisation and that these supervisors are appropriately trained and supported. Commissioners, as part of their clinical governance responsibility, should provide funding to ensure that Clinical Supervisors in the OOH service are adequately remunerated, with sufficient training and professional support structures and processes. These provisions should be reflected in the service level agreement with the provider and commissioning organisations need to be appropriately resourced with clearly identifiable ring- fenced funding for training within the OOH budget, and this should be a firm and monitored part of the OOH providers process. These arrangements should be routinely reviewed as part of the contract monitoring process.
8.7 Commissioning organisations need to have a more strategic and long-term view of OOH training. If training is prioritised, and trainees are trained comprehensively and consistently in the delivery of out-of-hours services, then doctors will have the necessary skills to work safely in this high-risk area. Furthermore, if trainees have a robust, structured and enjoyable training experience in an area where good relationships exist between the commissioning organisation, provider and deanery they would be empowered and encouraged to continue to work in the service once qualified. This will ensure that local, suitably skilled doctors are working in the out-of-hours service, and should reduce the need for providers to offer intensive induction for doctors who are not familiar with the local area, the unique nature of out-of-hours care, or both.18
17 http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_110330.pdf 18 Field and Thome. Provision of Out-of-Hours Report, 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 This review recommends that:
11. commissioning organisations should ensure that recommendation eight is implemented.
12 organisations responsible for commissioning OOH provision should ensure that requirements for the provision of sessions for GP trainees and the provision, training and continued professional support of Clinical Supervisors are appropriately resourced, and clearly identifiable ring-fenced funding for training is firmly monitored within the OOH budget .
9. Postgraduate Deaneries
The aim of the training is to enable GP StRs to learn, develop, practice and maintain their competencies in OOH working.19
9.1 The deanery will need to work with commissioning organisations and OOH providers to develop mechanisms to ensure that suitable quality training is available and that incentives are in place to encourage and support the provider in delivering and monitoring training.
According to the COGPED guidance the quality assurance of the GP training programme in OOH will include assessment of:
The induction processes for the initial exposure of GP StRs training in the OOH setting.
The placement’s level of workload, educational facilities and the overall quality of the learning environment.
The Clinical Supervisor’s ability (which must include skills in observation and the ability to give feedback).
The capability and capacity of the OOH organisation to deliver the clinical supervisory process.20
9.2 Postgraduate deaneries will expect all GP Specialty Trainees to obtain the necessary OOH experience and training to achieve the competences as described in the GP curriculum and required for the MRCGP. The curriculum sets out clearly that ‘GPs must be competent to provide out-of-hours by demonstrating the ability to manage certain conditions in the out-of-hours setting’. In addition to this deaneries fund, and are responsible for, the programmes of training and skills development of Clinical Supervisors. As referred to earlier in the Clinical Supervisor section (section five) we recommend the reaffirmation of the role of deaneries to provide training for doctors (who are not previously accredited as GP Trainers) and other appropriate health care professionals to be Clinical Supervisors.
9.2 There is some anecdotal evidence from providers that deaneries do not fully understand the processes within an OOH provider. The complaint from providers is that they are expected to organise high quality training sessions for trainees, often with constraints on time and resources. The relationship between deaneries, who provide educational governance, and the provider, who is responsible for clinical governance, is important to deliver high quality training. As mentioned before, where there is evidence of a good working relationship and operational procedures in place then OOH training seems to be implemented more successfully. An example of effective cross working could be an arrangement where trainees can book shifts online.
19 COGPED Position Statement, 2010 20 COGPED Position Statement, 2010 I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 9.3 An effective partnership between deanery, OOH providers and the relevant commissioning organisation is extremely important to implement and deliver quality training. Good communication and the sharing of relevant and appropriate information are also crucial. Across the UK there are examples of good practice that deaneries may wish to implement. This includes bi-annual OOH meetings for deaneries, commissioning organisation, and OOH providers to focus on education and training issues, deaneries sharing relevant issues from GP registrar exit surveys with commissioners and providers and the sharing of deanery assurance reports with the relevant commissioning organisation.
9.4 The main issues for deaneries concern the application of their Quality Management Framework (QMF) to OOH. Qualitative evidence suggests that there is a variation in the effectiveness of deanery quality management frameworks across the UK. To aid consistency deaneries should regularly review the provision of OOH training provided to their cohort of GP trainees in line with that applied to other Local Education Providers. It is recommended that the QMF should include core elements, such as the capacity of provision of OOH training provided, that such training is overseen suitably trained Clinical Supervisors and that the training provided meets the requirements of the GP curriculum. As part of their quality management process deaneries should also ensure that those individuals who assess the provision and support of GP training by OOH providers are familiar with the structure and delivery of OOH care. Some of the earlier examples of gaining familiarity with the OOH service referred to in the Trainer section of this document might also be applicable here. In addition to this, deaneries should ensure that their assessors of OOH providers use systematic and consistent approaches with a common reporting template, and provide reports that can be shared with the commissioning organisations. The review recognises that further discussions need to take place at COGPED for this to be agreed.
This review recommends that:
13. it is reaffirmed that it is the role of deaneries to provide training for doctors (who are not previously accredited as GP Trainers) and other appropriate health care professionals to be Clinical Supervisors. This will facilitate the implementation of recommendation six.
14. as part of their quality management process, deaneries should regularly review the provision of OOH training provided to their cohort of GP trainees in line with that applied to other Local Education Providers.
15. as part of their quality management process deaneries should ensure assessors of OOH providers are familiar with OOH. In addition to this deaneries should train those assessors to be systematic and consistent, and to use a common reporting template to produce a report which will be shared with the commissioning organisations.
10. General Medical Council
10.1 The General Medical Council approves all training posts for GP Specialty Training by applying their Quality Assurance Framework. The GMC's Quality Framework (QF) emphasises deanery input to quality management at local and national level. The purpose of the QF is to: Provide public and professional reassurance about the standards and quality of specialty in the UK through a robust, rigorous set of processes; Reflect fully the principles of good regulation, demonstrate value for money and be fit for purpose; Enable improvement and enhancement of the quality of specialty training; and
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 Ensure specialty training focus is maintained at local and national level by working with the Academy of Medical Royal Colleges (AoMRC), Colleges/Faculties and postgraduate deaneries.21 10.2 The GMC must be explicit when it is approving GP training programmes, that it is also approving the OOH training programme which is an integral part of this. This recommendation could be supported by an explicit statement from the GMC that explains that the deanery QMF should also be applied to OOH training, and that evidence to support this should be provided as part of the GMC visiting process. Existing GMC processes could also be utilised to ensure that training posts providing OOH training are approved. Already, OOH training is included within the Annual Specialty Report that the College makes to the GMC and this reporting system could be built upon. For example, on the approval training form there could be greater expansion of box 14 on form (B).
This review recommends that:
16. the GMC should be explicit that when it is approving GP training in a particular deanery that they are also approving the OOH training component in that training programme.
11. Conclusion 11.1 It is important that patients, their families and carers who need to use out-of-hours services have contact with competent GPs. All users accessing OOH services want to be seen by a GP who is competent and confident, familiar with local healthcare delivery and services, and also understands the wider health and social care system. As Steve Field and David Colin-Thomé make clear in their report, this can partly be remedied by ensuring that trainees have access to high quality OOH education provision.
11.2 It is essential that the profession reinforces the importance of OOH exposure and experience during training to produce high-quality GPs who are adequately prepared to undertake all aspects of the generalist’s role. By supporting the provision of OOH experiences within training we hope to raise the status of OOH provision and to enable trainees to attain the competences required by the GP Specialty Curriculum.
11.3 The review found that the competency framework does not need to be altered. The focus for change and improvement is the implementation and quality management of OOH training; in particular ensuring training is of a consistently high standard throughout the UK. Trainees that are signed off as competent by their educational supervisors should be fit for practise in OOH settings. However, the signing off of all trainees against the competency framework needs clear evidence (and thus congruent processes to deliver this evidence), especially in regard to the bench-marking of standards and ensuring GP Trainers are familiar with the delivery of OOH. It is important that trainees who do not attain the OOH competences within the normal period of their training programme, despite achieving all other competences, must not proceed to certification without this learning aspect being robustly addressed.
11.4 This review found that the number of sessions, as stated in the COGPED guidance, does not need to be increased. Currently given capacity issues for the OOH service, and the challenges faced by the trainee to complete the curriculum and training requirements, an increase in number of sessions could weaken both OOH training and the development of the other essential GP competences. The number of sessions recommended in the COGPED guidance should be regarded as the minimum required by most trainees to attain the necessary competences, however this must remain a competency assessed process, and if necessary, some trainees might require more sessions that the minimum indicated to be both competent and confident.
21 Taken from GMC Quality Framework I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 11.5 The Review did find that despite the COGPED guidance and improvements taking place across the system there is still variation in the implementation and quality of the training currently on offer within the UK. Therefore not all trainees are given the opportunities or preparation that they need to ensure they become properly confident. It is essential that quality management of OOH training takes place throughout every level of the system and GMC approval of training programmes must encompass OOH as well as in-hours training. The recommendations within this report are intended to strengthen the COGPED position and improve the quality management process surrounding OOH training.
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8 APPENDIX 1: Membership of OOH Training Review
Name Title Organisation Bill Reith Chair Postgraduate Training Board RCGP
Agnelo Clinical Champion Urgent and Emergency Care RCGP Fernandes
Janet Hall Vice-Chair Elect RCGP
Greg Irving AiT Chair RCGP
Simon Plint GP Liaison DH
David Sharp Rep RCGP Patient Partnership Group RCGP
David Bruce Director of Postgraduate Education East Scotland COGPED
Phil Matthews Deputy Director School of Postgraduate Education for General COGPED Practice Wales Claire Loughrey Director of Postgraduate General Practice Northern Ireland COGPED
Ian McLean Head of KSS School of General Practice COGPED
Terry John Chairman of the Education, Training and Workforce BMA subcommittee James Parsons Deputy Chair Trainee Committee BMA
Beth GPC Negotiator BMA McCarron-Nash
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
Staff:
Fiona Erasmus Head of Professional Standards RCGP Laura Hatchard Policy Officer, Policy and Public Affairs Team RCGP
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme Item 7.8
Appendix 2
East Highland OOH induction
Contact [email protected] with contact details for both you and your trainer. You will then be given contact details for your named OOH Clinical Supervisor and usually you’ll have a chat by phone before the first shift to arrange a slightly earlier start so you can be familiarized with the Adastra computer system and the layout of the PCECs and bags. East Highland runs from two Primary Care Emergency Centres (PCECS) at the Ross Memorial Minor Injuries Unit in Dingwall and the County Community Hospital in Invergordon covering 60,000 patients from Tain to Beauly. There is sometimes some overlap from East Sutherland and Inverness, with the Hub redirecting calls if one patch is busy.
Most people start their shifts in Dingwall, but one or two weekend shifts (and a couple of the Supervisors who are based in the North of the patch) have an Invergordon start. There is a driver in East Highland for home visits, but occasionally there are two doctors on for weekend daytimes, and you may be required to use your own car for carefully selected visits eg: Care Homes. There are also four Unscheduled Care Practitioners working from Invergordon at the weekend with nurse prescribing, and they can see some of the more straightforward problems eg: UTIs, minor injuries and go out on some home visits where appropriate. You will also be responsible for any inpatient problems at the RMH, the Rheumatology Unit, Fyrish long stay psychiatry ward and CCHI. This is not usually as onerous as it sounds, although you do get the occasional poorly patient.
Your Clinical Supervisor will supervise most, but not all, of your shifts, as we will try to give you a variety of shifts including evenings, weekends and one or two overnights, but these will all be with GPs who have completed the Clinical Supervisors Course, or are already GP trainers themselves. The Clinical Supervisor will contact your trainer before you start your shifts and after a few months to decide when you are ready to ‘go solo’ with remote supervision by telephone.
Please let Mrs Jo Donald, Practice Manager, Cromarty Medical Practice, Allan Square, Cromarty, IV11 8YF [email protected] of your availability for the year, so she can give you your year’s timetable. Any that you then find unable to do, we’d ask that you first try to swap with other Registrars working in East Highland, before contacting Jo for alternative shifts. As you need to be signed off by the end of May/beginning of June, and need a couple of weeks to settle in with your practice, we need to fit your 72 hours minimum in from end August to end of May. We’d usually expect you to work one or two Bank Holiday daytimes, as this gives a quite different experience, but we would not put any Registrar on for more than one of the Bank Holiday periods (unless it suited). We wont put you on Christmas Day.
Contact the Hub [email protected] or 01463667574 for your Adastra password. You may already have one for access to special notes and ACPA in your practice, but it also needs to be authorized for use in Out of Hours. If you do not have one and need an AR1 form then send the request to Jo Donald.
We hope you enjoy your time working in East Highland Out of Hours, which provides a good variety of experience in a friendly atmosphere.
I/DPGMEAssistants/Jerry O’Rourke/2011/H & I GP Specialty Training Programme