Unit 12, Abnormal Psychology Notes (2011 update for use with Chapter 16 in 2007 Myers text)
Perspectives on Psychological Disorders 563 A. Definition 1. harmful 2. atypical 3. disturbing 4. maladaptive 5. unjustifiable
Is ADHD a disorder? 563 The text provides no answer. The debate continues.
B. Understanding Psychological Disorders 564 What perspectives can help us understand psychological disorders?
The Medical Model a. medical model: diagnose the sickness and cure it 1.Etiology: Causation and developmental of the disorder. 2.Diagnosis: Identifying (symptoms) and distinguishing one disease from another. 3.Treatment: Treating a disorder in a psychiatric hospital. 4.Prognosis: Forecast about the disorder.
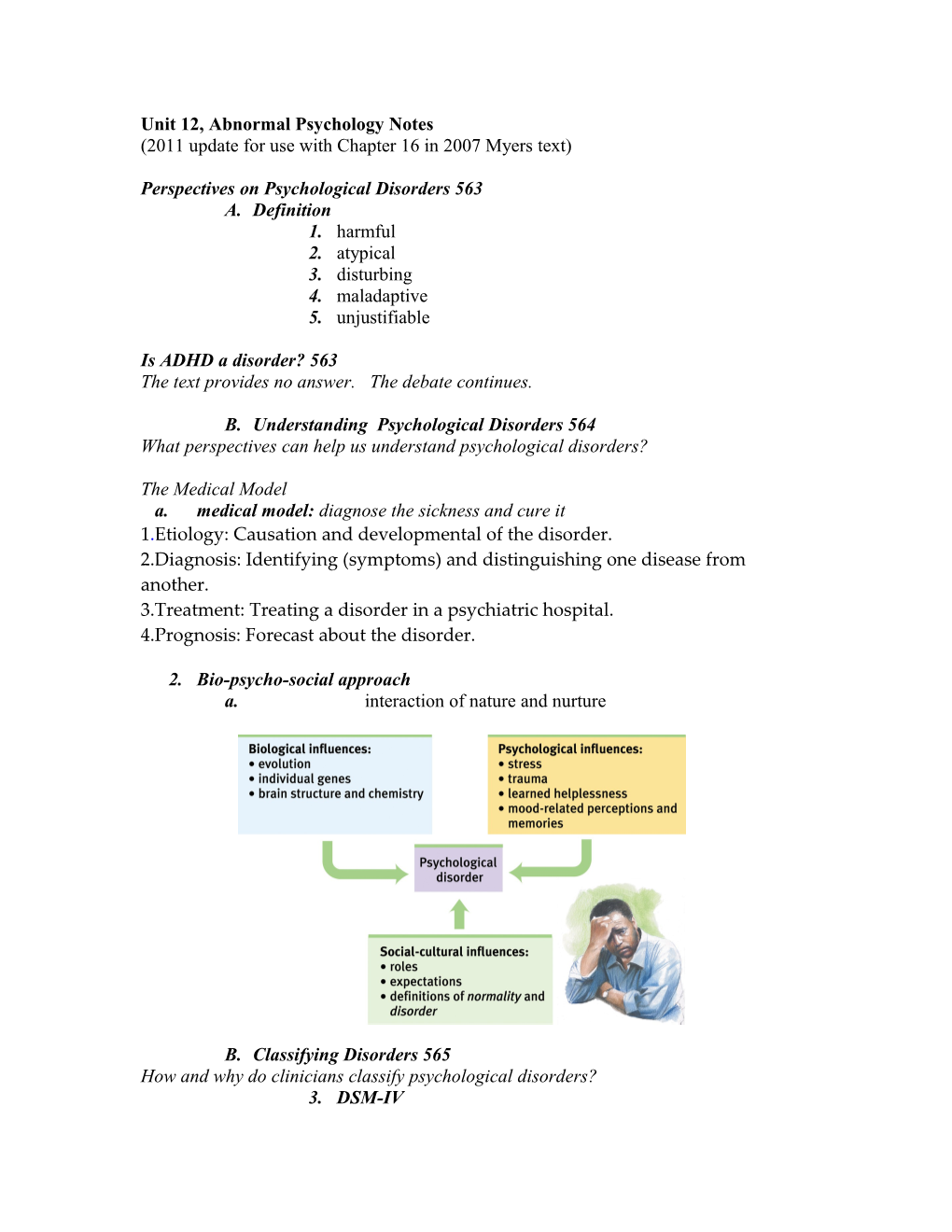
2. Bio-psycho-social approach a. interaction of nature and nurture
B. Classifying Disorders 565 How and why do clinicians classify psychological disorders? 3. DSM-IV a. Used to classify disorders b. Not used to explain causes 4. neurotic disorders: distressing but still can function 5. psychotic disorders: debilitating
Table 16.1 page 645 Axis I Is a Clinical Syndrome Present? Axis II Is a Personality Disorder Present? Axis III Is a General Medical Condition also Present? Axis IV Are Psychosocial or Environmental Problems Present? Axis V What is the Global Assessment of their functioning?
C. Labeling Psychological Disorders 567 Why do some psychologists criticize the use of diagnostic labels? 6. David Rosenhan (1973) study revealed the power of labeling the mentally ill 7. stigmatizing 8. stereotyping Labels can serve as “self-fulfilling prophecies”. D. Insanity and responsibility 569 9. Legal definitions a. wrongfulness of actions b. ability to participate in legal defense c. danger to self or others 10. Hinckley case, 1981 11. Dahmer case, 1991 12. Unabomber case 13. Andrea Yates case, 2002
II. Anxiety Type Disorders 569 What are anxiety disorders, and how do they differ from ordinary worries and fears? C. Generalized anxiety 1. State of tension, apprehension, ANS arousal D. Panic disorder 1. sudden, intense dread episode E. Phobias 1. persistent, intense, irrational fear of specific thing ex: agoraphobia—fear of being outside F. Obsessive-Compulsive Disorder (OCD) 1. unwanted thoughts constantly preoccupying you ex: taking ten showers a day to stay clean G. Post Traumatic Stress Disorder 1. Nightmares, insomnia and painful memories 2. Post traumatic growth: finding positive strengths while dealing with PTSD
Understanding Anxiety Disorders 574 1. Learning Perspective Fear conditioning: stimulus generalization after the initial fear producing event, followed by reinforcement to maintain the phobia or compulsion. Observational learning: Susan Minetka (1985) found monkeys transmit their fear of snakes 2. The biological perspective Natural selection: we are prepared to face certain risks Genes: Some studies point to an anxiety gene; other studies implicate glutamate overabundance making the brain more sensitive The Brain: the anterior cingulate cortex is hyperactive in those with OCD
Somatoform disorders 576 What are somatoform disorders? •Physical ailments that cannot be explained by organic causes •Psychosomatic diseases •Have a psychological origin •Symptoms are more imaginary than real
Types •1. Somatization disorder: affects mainly women; a list of minor complaints that may accompany depression or anxiety •2. Conversion disorder: loss of function of a specific organ •3. Hypochondriasis: excessive worry about developing a physical illness (Howard Hughes) Dissociative disorders 577 1. Sudden loss of memory or change in identity 2. Dissociative identity disorder (DID) a. Two or more identities that control a person’s behavior b. evidence includes changes in brain and body states and handedness c. Skeptics counter that it is a cultural phenomenon with few cases outside America 3. Dissociation: a sense of being separated from your body and watching yourself with a sense of detachment 4. Some psychologists find physical evidence for personality changes. a. Massive dissociation of self from ordinary consciousness b. role playing occurs: suggestions and leading by the therapist c.Nick Spanos (1986): dissociation is essentially role playing; Paul McHugh (1995) says the phenomenon is manufactured out of the patient-therapist relationship.
III. Mood Disorders 579 What are mood disorders, and what forms do they take? Lethargic, withdrawn, feeling worthless or unlovable A. Major Depressive Disorder 3. personal worthlessness 4. Dysthymic disorder: less disabling form of depression 5. low levels of norepinephrine 6. more females 7. last less than 3 mos. 8. therapy not need most times to recover 9. research: it’s increasing 10. Reduction of norepinephrine and serotonin has been implicated in depression. Drugs that alleviate mania reduce norepinephrine. B. Bipolar Disorder 11. alternating between lethargy and overexcitement 12. manic episode: overexcitement, hyperactivity, wild optimism
C. Understanding Mood Disorders 582 What causes mood disorders, and what might explain the Western world’s rising incidence of depression among youth and young adults?
Close Up: Suicide 584 1. Higher rates among men 2. Highest rates among older men 3. Depressed have 5x higher rate 4. Few who talk of actually commit 5. Most who commit have talked of it 6. Whites more than blacks 7. Women more likely to attempt 13. The biological perspective a. Genetic influences; heritability of depression is 35 to 40 percent Linkage analysis searchers for the genes responsible b. The Depressed Brain c. neurotransmitters: lower levels of norepinephrine and/or serotonin d. The hippocampus is vulnerable to stress related damage e. The left frontal lobe is less active during depression 14. The socio cognitive perspective a. self-blaming attributions, b. negative thoughts and negative moods interact; women tend to overthink leading to higher rates than men (Susan Nolen-Hoeksema, 2003) c. maladaptive explanations of failure, your explanatory style: stable, internal and global thinkers display this negative approach d. Martin Seligman has describe this pessimistic style of thinking (1991).
IV. Schizophrenia 589 What patterns of thinking, perceiving, feeling, and behaving characterize schizophrenia? H. Symptoms 1. disorganized and delusional thinking Ex: thinking you’re “King of the Universe” (when you’re not) Ex: disordered speech (word salad) 2. Hallucinations: perceiving things that are not there; frequently such hallucinations are auditory and lesser visual, somatosensory, olfactory or gustatory. 3. Inappropriate emotions and actions A schizophrenic person may laugh at the news of someone dying, or show no emotion at all (apathy). Patients with schizophrenia can continually rub an arm or rock a chair or remain motionless for hours (catatonia).
Positive and Negative symptoms + Delusions + Hallucinations + Disorganized speech + Disordered behavior - Lack of expression - Lack of speech - Lack of direction
C. Understanding Schizophrenia 592 What causes schizophrenia? 1. Brain abnormality: excess receptors for dopamine 2. Abnormal brain activity and abnormality: Schizophrenia patients may express morphological changes in the brain like enlargement of fluid filled ventricles. Maternal virus during pregnancy: Schizophrenia has also been observed individuals who contracted viral infection (flu) during the middle of their fetal development. Genetics: predisposition for The likelihood of individuals suffering from schizophrenia is 50% if their identical twins have the disease (Gottesman, 1991). Early warning sign: early physical maturation 4. Psychological factors: early warning signs include emotional issues, poor peer interaction, separation from parents, disruptive behavior, and mother with the disorder. John Nash from A Beautiful Mind as an example V. Personality Disorders 596 What characteristics are typical of personality disorders? Personality disorders: disruptive, enduring behavior patterns that interfere with normal social functioning •A. Antisocial Personality Disorder –1. Disorder in which the person (usually man) exhibits a lack of conscience for wrongdoing, even toward friends and family members –2. May be aggressive and ruthless or a clever con artist Understanding Antisocial Personality Disorder Genes put these people at risk A biology based on fearlessness. B. Narcissistic 2. preoccupied with self importance C. Avoidant i. being withdrawn D. Schizoid i. eccentric and social disengaged E. Histrionic 1. Attention getting behavior; seeking praise
F. Murderous minds 1. frontal cortex has reduced activation failing to check impulses and/or aggression 2. PET scans of 41 murderers revealed reduced activity in the frontal lobes. In a follow-up study repeat offenders had 11% less frontal lobe compared to normals (Raine et al., 1999; 2000).
VI. Rates of Psychological Disorders 599
How many people suffer, or have suffered, from a psychological disorder? Key terms: 602 (see study guide) AP Quiz: 602-603