Orofacial pain
Neuralgia Trigeminal neuralgia Typical Atypical Post herpetic neuralgia Post traumatic neuralgia
Neurovascular Migraine Migrainous neuralgia Giant cell arteritis Cluster headaches Tension headache Trigeminal autonomic SUNCT SUNA
Idiopathic / Persistent Burning mouth syndrome Atypical facial pain Atypical odontalgia
Other cause found
Non classifiable Trigeminal nerve injury
Hospital number Patients sticker
Date examination Date injury Mechanism of injury ID block Surgery (TMS, Biopsy) Implant Other Date repair Improvement Y/N Nerve RMH Comments: Pain Y/N Evoked / Spontaneous Constant / Intermittent What cause? At rest/ taste /movement/cold Pain descriptive Dull / Sharp Burning/Ache Shooting / stabbing Altered sensation Y/N Numbness Paraesthesia pins/needles Allodynia Hyperalgesia Neuralgia Function Eating / tongue biting Drinking Sleeping Speaking Kissing Shaving / makeup Change in taste Y / N no pain worst pain imaginable TESTS CNTs Y/N Questionnaire Y/N EMG Y/N Electrical Y/N Thermal Y/N Capsaicin Y/N Ethyl Chloride Y/N Photo Y/N At rest no pain worst pain imaginable Capsaicin no pain worst pain imaginable Touch no pain worst pain imaginable Spicy foods no pain worst pain imaginable Cranial Nerves I II III IV V a b c VI VII VIII IX X XII Area CNTs Right Left Area % Two point discrimination SO IO UL LL Chin Tongue lat Tongue tip Tongue vent Thermal Semmes Weinstein / Light touch SO IO UL LL Chin Tongue lat Tongue tip Tongue vent Capsaicin EC Sharp/blunt Lip Tongue Hypoalgesia Pain threshold Lip Tongue Palpation LN Pain Neuralgia Papillae count Subjective function Moving point discrimination Static Dynamic Taste Sweet Sour Bitter Salt Allodynia – static/moving - cold - taste - capsaicin TREATMENT HISTORY On the list below, indicate Yes or No for each treatment listed. For each treatment recommended by a health care professional for your facial pain or jaw problem, indicate how helpful you found it. If recommended, how helpful was treatment?
Recommended If recommended, how helpful was treatment? Very Somewhat Not Made Did Not No Yes Helpful Helpful Helpful Worse Do a. Mouth appliance (“bite plate,” 0 1 1 2 3 4 5 “night guard,” “repositioning appliance,” “splint”) b. Physical therapy (heat, cold 0 1 1 2 3 4 5 packs, stretching) c. Relaxation training/biofeedback 0 1 1 2 3 4 5 d. Physical exercise (running, 0 1 1 2 3 4 5 bicycling) e. Stress management/counseling 0 1 1 2 3 4 5 f. Change of diet 0 1 1 2 3 4 5 g. Muscle relaxant medications 0 1 1 2 3 4 5 h. Analgesics or “painkillers” 0 1 1 2 3 4 5 i. Anti-inflammatory medications 0 1 1 2 3 4 5 j. Anti-depressant medications 0 1 1 2 3 4 5 k. Anti-anxiety medications 0 1 1 2 3 4 5 l. Other medications - please describe: 0 1 1 2 3 4 5
0 1 1 2 3 4 5
0 1 1 2 3 4 5
m.Bite adjustment 0 1 1 2 3 4 5 n. Orthodontics 0 1 1 2 3 4 5 o. Dental reconstruction (crowns, 0 1 1 2 3 4 5 bridges) p. Muscle or joint injections 0 1 1 2 3 4 5 q. Surgery 0 1 1 2 3 4 5 r. Chiropractic manipulation 0 1 1 2 3 4 5 s. Evaluation and/or referral 0 1 1 2 3 4 5 t. Other treatment - please describe: Dates Name specialty of clinician 0 1 1 2 3 4 5 0 1 1 2 3 4 5
0 1 1 2 3 4 5 MEDICATION USE Do you require antibiotic medication before dental treatment? List all drugs and medications you are currently taking for any purpose.
Nonprescription Medications Prescription Medications (for example, aspirin, laxatives, antacids, diet pills herbal remedies, marijuana, other “street” drugs) 1. 1.
2. 2.
3. 3.
4. 4.
5. 5.
6. 6.
SPECIALISTS SEEN Type location date and treatment received Type of specialist GMP, Ear Nose Throat, Neurologist, neurosurgeon, maxillofacial, dentist, acupuncture, cranio osteopathy, physio, speech therapist, other Type and date seen Hospital Treatment received / Diagnosis HAD Scale
Doctors are aware that emotions play an important part in illnesses and this questionnaire is designed to help your doctor know how you feel. Read each item and place a firm tick in the box opposite the reply, which comes closest to how you have been feeling in the past week.
Don’t take too long over your replies; your immediate reaction to each item will probably be more accurate than a long thought-out response.
Tick one box only in each section
1 I feel tense or wound up: 8 I feel as if I am slowed down: Most of the time Nearly all the time A lot of the time Very often Time to time, occasionally Sometimes Not at all Not at all 2 I still enjoy the things I used to enjoy: 9 I get a sort of frightened feeling like Definitely as much “butterflies” in the stomach: Not quite so much Not at all Only a little Occasionally Hardly at all Quite often Very often 3 I get a sort of frightened feeling as if something awful is about to happen: 10 I have lost interest in my appearance: Very definitely and quite badly Definitely Yes, but not too badly I don’t take so much care as I should A little, but it doesn’t worry me I may not take quite as much care Not at all I take just as much care as ever 4 I can laugh and see the funny side of 11 I feel restless as if I have to be on the things: move: As much as I always could Very much indeed Not quite so much now Quite a lot Definitely not so much now Not very much Not at all Not at all 5 Worrying thoughts go through my mind: 12 I look forward with enjoyment to things: A great deal of the time As much as I ever did A lot of the time Rather less than I used to From time to time bur not too often Definitely less than I used to Only occasionally Hardly at all 6 I feel cheerful 13 I get sudden feelings of panic: Not at all Very often indeed Not often Quite often Sometimes Not very often Most of the time Not at all 14 I can enjoy a good book or radio or TV 7 I can sit at ease and feel relaxed: programme: Definitely Often Usually Sometimes Not often Not often Not at all Very seldom McGill Questionnaire NAME: DATE: Circle the word that describes how your pain feels right now:
Nil Mild Moderate Severe Most severe
Circle the words below that best describe your current pain. Use only one word in each group. Leave out any group if the words are unsuitable.
1 2 3 4
Flickering Jumping Pricking Sharp Quivering Flashing Boring Cutting Pulsing Shooting Drilling Lacerating Throbbing Stabbing Beating Lancinating Pounding
5 6 7 8
Pinching Tugging Hot Tingling Pressing Pulling Burning Ithcy Gnawing Wrenching Scalding Smarting Cramping Searing Stinging Crushing
9 10 11 12
Dull Tender Tiring Sickening Sore Taut Exhausting Suffocating Hurting Rasping Aching Splitting Heavy
13 14 15 16
Fearful Punishing Wretched Annoying Frightful Gruelling Blinding Troublesome Terrifying Cruel Miserable Vicious Intense Killing Unbearable
17 18 19 20 Spreading Tight Cool Nagging Radiating Numb Cold Nauseating Penetrating Drawing Freezing Agonizing Piercing Squeezing Dreadful Tearing Torturing SF36 Health Survey INSTRUCTIONS: This set of questions asks for your views about your health. This information will help keep track of how you feel and how well you are able to do your usual activities. Answer very question by marking the answer as indicated. If you are unsure about how to answer a uestion please give the best answer you can. 1. In general, would you say your health is: (Please tick one box.) Excellent _ Very Good _ Good _ Fair _ Poor _ 2. Compared to one year ago, how would you rate your health in general now? (Please tick one box.) Much better than one year ago _ Somewhat better now than one year ago _ About the same as one year ago _ Somewhat worse now than one year ago _ Much worse now than one year ago _ 3. The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much? (Please circle one number on each line.) Activities Yes, Limited A Lot Limited A Little Not Limited At All 3(a) Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports Yes, Limited A Lot Limited A Little Not Limited At All 3(b) Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf Yes, Limited A Lot Limited A Little Not Limited At All 3(c) Lifting or carrying groceries Yes, Limited A Lot Limited A Little Not Limited At All 3(d) Climbing several flights of stairs Yes, Limited A Lot Limited A Little Not Limited At All 3(e) Climbing one flight of stairs Yes, Limited A Lot Limited A Little Not Limited At All 3(f) Bending, kneeling, or stooping Yes, Limited A Lot Limited A Little Not Limited At All 3(g) Waling more than a mile Yes, Limited A Lot Limited A Little Not Limited At All 3(h) Walking several blocks Yes, Limited A Lot Limited A Little Not Limited At All 3(i) Walking one block Yes, Limited A Lot Limited A Little Not Limited At All 3(j) Bathing or dressing yourself Yes, Limited A Lot Limited A Little Not Limited At All 4. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health? Yes No 4(b) Accomplished less than you would like Yes No 4(c) Were limited in the kind of work or other activities Yes No 4(d) Had difficulty performing the work or other activities (for example, it took extra effort) Yes No 5. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (e.g. feeling depressed or anxious)? Yes No 5(a) Cut down on the amount of time you spent on work or other activities Yes No 5(b) Accomplished less than you would like Yes No 5(c) Didn’t do work or other activities as carefully as usual Yes No 6. During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbours, or groups? (Please tick one box.) Not at all _ Slightly _ Moderately _ Quite a bit _ Extremely _ 7. How much physical pain have you had during the past 4 weeks? (Please tick one box.) None _ Very mild _ Mild _ Moderate _ Severe _ Very Severe _ 8. During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)? (Please tick one box.) Not at all _ A little bit _ Moderately _ Quite a bit _ Extremely _ 9. These questions are about how you feel and how things have been with you during the past 4 weeks. Please give the one answer that is closest to the way you have been feeling for each item. (Please circle one number on each line.) 1. All of the Time 2. Most of the Time A Good Bit of the Time 3. Some of the Time 4. A Little of the Time 5. None of the Time 9(a) Did you feel full of life? 1 2 3 4 5 6 9(b) Have you been a very nervous person? 1 2 3 4 5 6 9(c) Have you felt so down in the dumps that nothing could cheer you up? 1 2 3 4 5 6 9(d) Have you felt calm and peaceful? 1 2 3 4 5 6 9(e) Did you have a lot of energy? 1 2 3 4 5 6 9(f) Have you felt downhearted and blue? 1 2 3 4 5 6 9(g) Did you feel worn out? 1 2 3 4 5 6 9(h) Have you been a happy person? 1 2 3 4 5 6 9(i) Did you feel tired? 1 2 3 4 5 6 10. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives etc.) (Please tick one box.) All of the time _ Most of the time _ Some of the time _ A little of the time _ None of the time _ 11. How TRUE or FALSE is each of the following statements for you? (Please circle one number on each line.) Definitely True Mostly True Don’t Know Mostly False DefinitelyFalse 11(a) I seem to get sick a little easier than other people 1 2345 11(b) I am as healthy as anybody I know 1 2 3 4 5 11(c) I expect my health to get worse 1 2 3 4 5 11(d) My health is excellent 1 2 3 4 5 Thank You BPI Temporomandibular Joint pain / Orofacial Pain
Hospital number Patients sticker
Date examination Date started Precipitating episode? Trauma Injury Surgery (TMS, Bx) Implant Other Previously treated Y/N Improvement Y/N Right Left Bilateral Other joint pains? RMH Comments: Pain Y/N Evoked / Spontaneous Constant / Intermittent What cause? At rest/ taste Frequency /movement/cold Pain descriptive Dull / Sharp Burning/Ache Shooting / stabbing Pain centre Radiation to Function Eating Drinking Sleeping Speaking At rest no pain worst pain imaginable Eating no pain worst pain imaginable Opening no pain worst pain imaginable Pain worse Morning / evening Diet altered Y/N Bruxist Gum chewing Clencher TESTS Joint examination Trismus Y/N Opening max (mm) Opening deviation Full lateral movement Swelling / asymmetry R-L Centre line coincident Y/N Max R-L Mandible R-L (mm) Pain on palpation joints Y/N Chin midline Clicking R – L Crepitus Pre Mid Post Locked opening Locked closing Occlusion Ant open bite Class I II III Post open bite Attrition Questionnaire Y/N Cranial Nerves I II III IV V a b c VI VII VIII IX X XII Area TREATMENT HISTORY On the list below, indicate Yes or No for each treatment listed. For each treatment recommended by a health care professional for your facial pain or jaw problem, indicate how helpful you found it. If recommended, how helpful was treatment?
Recommended If recommended, how helpful was treatment? Very Somewhat Not Made Did Not No Yes Helpful Helpful Helpful Worse Do a. Mouth appliance (“bite plate,” 0 1 1 2 3 4 5 “night guard,” “repositioning appliance,” “splint”) b. Physical therapy (heat, cold 0 1 1 2 3 4 5 packs, stretching) c. Relaxation training/biofeedback 0 1 1 2 3 4 5 d. Physical exercise (running, 0 1 1 2 3 4 5 bicycling) e. Stress management/counseling 0 1 1 2 3 4 5 f. Change of diet 0 1 1 2 3 4 5 g. Muscle relaxant medications 0 1 1 2 3 4 5 h. Analgesics or “painkillers” 0 1 1 2 3 4 5 i. Anti-inflammatory medications 0 1 1 2 3 4 5 j. Anti-depressant medications 0 1 1 2 3 4 5 k. Anti-anxiety medications 0 1 1 2 3 4 5 l. Other medications - please describe: 0 1 1 2 3 4 5
0 1 1 2 3 4 5
0 1 1 2 3 4 5
m.Bite adjustment 0 1 1 2 3 4 5 n. Orthodontics 0 1 1 2 3 4 5 o. Dental reconstruction (crowns, 0 1 1 2 3 4 5 bridges) p. Muscle or joint injections 0 1 1 2 3 4 5 q. Surgery 0 1 1 2 3 4 5 r. Chiropractic manipulation 0 1 1 2 3 4 5 s. Evaluation and/or referral 0 1 1 2 3 4 5 t. Other treatment - please describe: 0 1 1 2 3 4 5
0 1 1 2 3 4 5
0 1 1 2 3 4 5 . DURING THE PAST SIX MONTHS, HOW OFTEN HAVE YOU HAD EACH OF THE FOLLOWING JAW SYMPTOMS?
How often… Never Sometimes Often Always
a. Does your jaw CLICK or POP when you open or close 0 1 2 3 your mouth or when chewing? b. Does your jaw make a GRATING or GRINDING noise 0 1 2 3 when it opens and closes or when chewing? c. Do your JAW JOINT NOISES prevent you from doing 0 1 2 3 activities that you would otherwise do? d. Does your jaw ACHE or FEEL STIFF when you wake 0 1 2 3 up in the morning? e. Does your jaw HURT WHEN YOU CHEW or shortly 0 1 2 3 after eating? f. Does ache or pain in your jaw LIMIT YOUR ABILITY 0 1 2 3 TO CHEW to the extent that it is difficult to eat? g. Do you wake up in the morning with HEADACHES? 0 1 2 3 h. Do you have NOISES or RINGING in your ears? 0 1 2 3 i. Do your ears feel CONGESTED? 0 1 2 3 j. Have you been told, or do you notice, that you GRIND 0 1 2 3 your teeth or CLENCH your jaw while sleeping at night? k. Does limited ability to use your jaws PREVENT you 0 1 2 3 from doing ACTIVITIES that you would otherwise do? l. Have you ever had your jaw LOCK or CATCH so that it 0 1 2 3 won’t open all the way? (If Never, go to question “n”) m.Was this locking or catching severe enough to interfere 0 1 2 3 with your ABILITY TO EAT? n. Have you ever had your jaw lock or catch so that YOU 0 1 2 3 CAN’T CLOSE IT ALL THE WAY once it’s open? o. During the day, do you GRIND your teeth or CLENCH 0 1 2 3 your jaw? p. Does your BITE feel UNCOMFORTABLE or unusual? 0 1 2 3 15.Was the CAUSE of your pain or jaw limitation related to any of the following factors? Do any of the following factors make your problem WORSE? For each of the items listed below, circle “C” for CAUSE or “W” for WORSE for each one that applies to your facial pain problem.
Oral Function, Habit and Physical Factors Behavioral Factors Stress-Related Factors C W Dental Treatment C W Chewing, smiling, C W Family, work, school, or Typ yawning, or laughing other stress e Dat e C W Clenching, grinding C W Emotional upset C W Accident Typ C W Nail biting or other C W Worry or anxiety e oral Dat habits e C W Feeling “blue”/depression C W Othe C W Othe r: r: C W Othe r: Date
16. Are your symptoms better or worse at 17. What activities does your present jaw the following times? problem prevent or limit you from doing?
Better Worse No N/A No No Difference Yes Yes Upon 1 2 3 4 0 1 Chewing 0 1 Swallowing awakening During the 1 2 3 4 0 1 Drinking 0 1 Cleaning teeth or day face In the 1 2 3 4 0 1 Exercising 0 1 Yawning evening At work 1 2 3 4 0 1 Eating hard 0 1 Sexual activity foods At home 1 2 3 4 0 1 Eating soft 0 1 Talking foods 0 1 Smiling/laughin 0 1 Having your usual g facial appearance 18.PAIN IMPACT
a. About how many days in the LAST SIX MONTHS have you been kept from your usual activities (work, school, housework) because of facial pain? For example: EVERY DAY = 180 days, EVERY OTHER DAY = 90 days, etc.
Days
b. In the PAST SIX MONTHS, how much has facial pain interfered with your daily activities rated on a scale from 0 to 10 where 0 is “No interference” and 10 is “Unable to carry on any activities”?
0 1 2 3 4 5 6 7 8 9 10 No interference Unable to carry on any activities
c. In the PAST SIX MONTHS, how much has facial pain interfered with your ability to take part in recreational, social and family activities?
0 1 2 3 4 5 6 7 8 9 10 No interference Unable to carry on any activities
d. In the PAST SIX MONTHS, how much has facial pain interfered with your ability to work (including housework)?
0 1 2 3 4 5 6 7 8 9 10 No interference Unable to carry on any activities
e. Based on all the things you do to cope or deal with your facial pain, on an average day, how much control do you feel you have over it?
0 1 2 3 4 5 6 No control Some control Complete control
f. Based on all the things you do to cope or deal with your facial pain, on an average day, how much are you able to decrease it?
0 1 2 3 4 5 6 Can’t decrease it at all Can decrease it somewhat Can decrease it completely 19.GENERAL MEDICAL INFORMATION - PRESENT
Circle the symptoms listed below that you are PRESENTLY experiencing or HAVE EXPERIENCED FREQUENTLY during the past SIX MONTHS.
GENERAL MUSCULOSKELETAL BEHAVIORAL weight loss joint pain anger weight gain swollen joints worry change in appetite muscle cramping sleep difficulties always hungry arm/hand weakness reduced social activities always thirsty problems at work/home/school frequent urination GASTROINTESTINAL tend to feel hot indigestion SKIN CHANGES tend to feel cold reflux/heartburn skin color changes fatigue nausea/vomiting skin itching/burning faint easily constipation other skin problems night sweats diarrhea nail changes bleed easily bruise easily CARDIOVASCULAR NEUROLOGICAL shortness of breath with loss of muscle exertion control/paralysis NOSE/THROAT racing or irregular heart beat numbness/tingling congested/runny nose swollen ankles handwriting changes nose bleeds cold ankles/feet memory changes nasal obstruction chest pain/angina neuropathy sore throat hoarseness/voice changes RESPIRATORY EARS mouth breathing/ snoring coughing spells hearing loss sleep apnea cough up phlegm ringing ears wheezing earaches HEAD & NECK frequent colds dizziness neck pain use more than 2 pillows to pressure/stuffiness in ears sleep neck lump/swelling headache EYES OTHER PAIN facial pain vision changes back pain migraine eye itching abdominal pain shoulder dry eyes arm pain eye pain leg pain other pain Check here if you have none of the symptoms listed above.
20.GENERAL MEDICAL INFORMATION Would you say your health in general is excellent, very good, good, fair, or poor?
1 Excellent 2 Very Good 3 Good 4 Fair 5 Poor
21.How good a job do you feel you are doing in taking care of your health overall?
1 Excellent 2 Very Good 3 Good 4 Fair 5 Poor 22.Has there been a change in your general health in the past year? 0 No 1 Yes
23. Your physician:
Phone Number: — —
24.Date of your last physical examination: / /
25.a. Are you currently being treated by a physician? 0 No 1 Yes
b. Are you currently being treated by a psychiatrist, psychologist or mental health worker? 0 No 1 Yes
26.Do you engage in regular exercise? 0 No 1 Yes
27.HISTORY OF ILLNESS Provide an answer for each item listed below. Check the “N” column for those conditions you have NEVER had, the “C” column for conditions you CURRENTLY have, and “P” column for the conditions you have had in the PAST.
N C P N C P N C P Cancer Injury to face/neck/jaw Kidney disease Genetic (inherited) disease Fractures Bladder disease Leukemia Concussion Urethritis Lymphoma Arthritis Liver disease Organ transplant Headache Rheumatic fever Rheumatoid arthritis Migraine Scarlet fever Lupus Erythematosus Back pain Polio Other systemic arthritic Abdominal pain Strep throat disease Sjogren’s syndrome Mononucleosis Other autoimmune disease Herpes zoster Diabetes Fungal infections Hepatitis Thyroid problems Other skin disease Venereal disease Hormone disorder Genital/anal warts Gastric ulcer Genital herpes High blood pressure Colitis Arteriosclerosis Pacreatitis Psychiatric illness Heart attack/myocardial Gastritis Anxiety/panic attacks infarction Angina/chest pain Crohn’s disease Depression Heart murmur Celiac Sprue Suicide attempt or thoughts Heart valve problems Gall bladder problems Physical/sexual/emotional abuse Other heart disease Splenectomy Irritable bowel syndrome Drug abuse Bleeding disorder Alcohol abuse Anemia Emphysema Pneumonia Prosthetic valve/joint Epilepsy/seizures Bronchitis Head/neck radiation therapy Neuralgia Sinusitis Stroke Hayfever HIV infection Other neurological problems Asthma AIDS Glaucoma Tuberculosis Other immune disease
Check here if there are words in this section you do not understand. 29.WOMEN ONLY Circle any of the following that apply to you.
Have you had… Are you… a difficult pregnancy using birth control pills irregular periods PRESENTLY PREGNANT: ______months pregnant menstrual pains going through menopause a hysterectomy postmenopausal ovary(ies) removed using hormone therapy none of the above none of the above
30.MAJOR HOSPITALIZATIONS, SURGERIES, AND BLOOD TRANSFUSIONS
Date Reason
/ / ______
/ / ______
/ / ______
Check here if no hospitalizations, surgeries, or blood transfusions.
31.ALLERGIC OR UNUSUAL REACTIONS Circle any of the following you have had an allergic or other unusual reaction to.
Penicillin Other drugs: Other allergies (food, metals, etc.): Sulfa Aspirin Opiates/codei Local ne anesthesia Iodine Latex
Check here if no allergic or unusual reactions.
32. MEDICATION USE Do you require antibiotic medication before dental treatment? List all drugs and medications you are currently taking for any purpose.
Nonprescription Medications Prescription Medications (for example, aspirin, laxatives, antacids, diet pills herbal remedies, marijuana, other “street” drugs) 1. 1.
2. 2. 3. 3.
4. 4.
5. 5.
6. 6.
Check here if you are taking no prescription or nonprescription medications.
DOCTOR’S USE:
33.CAFFEINE, ALCOHOL AND TOBACCO USE
a. Average number of caffeinated b.Average number of alcoholic beverages you beverages you drink in a DAY. drink in a WEEK.
Coffee 0 1-2 3+ Beer 0 1-2 3-5 6+ Tea 0 1-2 3+ Wine 0 1-2 3-5 6+ Cola 0 1-2 3+ Spirits/other 0 1-2 3-5 6+
c. Have you EVER used tobacco products? 0 No 1 Yes
If Yes, circle the type(s) of tobacco products.
Cigarette Pipe/cigar Smokeless
Do you CURRENTLY use tobacco products? 0 No 1 Yes
If Yes, circle the average number of uses per DAY.
1 Less than 10 times/day 2 11-20 times/day 3 More than 20 times/day
How many years have you used a tobacco product?
1 Less than 5 years 2 6-10 years 3 11-20 years 4 More than 20 years 34. FAMILY MEDICAL HISTORY Mark in either the “Y” for Yes or “N” for No column to indicate any of the following medical problems that have been present in your parents, brothers/sisters, or other close relatives.
Y N Y N Y N cancer (type: allergic disorders TMJ problems ______) asthma genetic (inherited tuberculosis rheumatoid arthritis disease) arthritis lupus erythematosus stomach/intestinal back pain other systemic arthritic problems disease kidney or bladder headache or migraine other immune system problems disease liver disease seizures neurological disease drug abuse diabetes alcoholism high blood pressure anemia heart disease psychiatric illness bleeding disorders stroke anxiety/panic attacks depression suicide or attempted suicide
Check here if no one in your family has ever had any of the problems listed above.
DOCTOR’S USE: 35. PREVIOUS DENTAL CARE a. Circle those items that describe your past dental care.
Circle one: Circle all that apply: Regular dental care Wisdom tooth extractions Bite adjustment Emergency treatment Treatment for jaw trauma/fracture Night only guard/splint Occasional dental care Periodontal (gum) surgery TMJ problems Root canal therapy Facial pain Orthodontics Other: Gum disease (pyorrhea, gingivitis, or periodontal disease)
b. Would you say your ORAL HEALTH in general is:
1 Excellent 2 Very 3 Good 4 Fair 5 Poor Good
c. How good a job do you feel you are doing in taking care of your oral health?
1 Excellent 2 Very 3 Good 4 Fair 5 Poor Good
Date of your last regular dental visit: / /
Name and address of your dentist:
DOCTOR’S USE: 36.SYMPTOM CHECKLIST In the LAST MONTH, how much you have been distressed by: Not at all A little bit Moderately Quite a bit Extremely a. Headaches 1 2 3 4 5 b. Nervousness or shakiness inside 1 2 3 4 5 c. Faintness or dizziness 1 2 3 4 5 d. Loss of sexual interest or pleasure 1 2 3 4 5 e. Feeling easily annoyed or irritated 1 2 3 4 5 f. Pains in the heart or chest 1 2 3 4 5 g. Feeling low in energy, slowed down 1 2 3 4 5 h. Sleep that is restless or disturbed 1 2 3 4 5 i. Trembling 1 2 3 4 5 j. Poor appetite 1 2 3 4 5 k. Crying easily 1 2 3 4 5 l. Feeling of being caught or trapped 1 2 3 4 5 m. Suddenly being scared for no reason 1 2 3 4 5 n. Blaming yourself for things 1 2 3 4 5 o. Pains in the lower back 1 2 3 4 5 p. Feeling lonely 1 2 3 4 5 q. Feeling blue 1 2 3 4 5 r. Worrying too much about things 1 2 3 4 5 s. Feeling no interest in things 1 2 3 4 5 t. Feeling fearful 1 2 3 4 5 u. Heart pounding or racing 1 2 3 4 5 v. Nausea or upset stomach 1 2 3 4 5 w. Soreness of your muscles 1 2 3 4 5 x. Trouble falling to sleep 1 2 3 4 5 y. Difficulty making decisions 1 2 3 4 5 z. Trouble getting your breath 1 2 3 4 5 aa. Hot or cold spells 1 2 3 4 5 bb. Numbness or tingling anywhere 1 2 3 4 5 cc. A lump in your throat 1 2 3 4 5 dd. Feeling hopeless about the future 1 2 3 4 5 ee. Feeling weak in parts of your body 1 2 3 4 5 ff. Feeling tense or keyed up 1 2 3 4 5 gg. Heavy feelings in your arms or legs 1 2 3 4 5 hh. Thoughts of death or dying 1 2 3 4 5 ii. Overeating 1 2 3 4 5 jj. Awakening in the early morning 1 2 3 4 5 kk. Thoughts of ending your life 1 2 3 4 5 ll. Feeling everything is an effort 1 2 3 4 5 mm. Spells of terror or panic 1 2 3 4 5 nn. Feeling so restless you couldn’t sit 1 2 3 4 5 still oo. Feelings of worthlessness 1 2 3 4 5 pp. The feeling that something bad is 1 2 3 4 5 going to happen to you qq. Thoughts and images of a frightening 1 2 3 4 5 nature rr. Feelings of guilt 1 2 3 4 5 ss. The idea that something serious is 1 2 3 4 5 wrong with your body tt. The idea that something is wrong with 1 2 3 4 5 your mind
37.STRESS a. How much stress have you experienced in the PAST MONTH as a result of:
None A little Some A great deal Home or family concerns 0 1 2 3 Work or school concerns 0 1 2 3 Financial concerns 0 1 2 3 Social or personal relationship 0 1 2 3 Health concerns 0 1 2 3 In general, how much stress have 0 1 2 3 you experienced in the past month?
b. Have any of the following events happened to you in the LAST YEAR?
No Yes Change in residence 0 1 Change in marital status (marriage, divorce or separation) 0 1 Change in living arrangement 0 1 Gain or loss of employment 0 1 Retirement of self or spouse 0 1 Birth in the family 0 1 Death of a close friend or relative 0 1 Serious illness or injury of a close family member 0 1 Serious illness of injury of self 0 1 Major change in financial circumstances 0 1 HAD Scale
Doctors are aware that emotions play an important part in illnesses and this questionnaire is designed to help your doctor know how you feel. Read each item and place a firm tick in the box opposite the reply, which comes closest to how you have been feeling in the past week.
Don’t take too long over your replies; your immediate reaction to each item will probably be more accurate than a long thought-out response.
Tick one box only in each section
1 I feel tense or wound up: 8 I feel as if I am slowed down: Most of the time Nearly all the time A lot of the time Very often Time to time, occasionally Sometimes Not at all Not at all 2 I still enjoy the things I used to enjoy: 9 I get a sort of frightened feeling like Definitely as much “butterflies” in the stomach: Not quite so much Not at all Only a little Occasionally Hardly at all Quite often Very often 3 I get a sort of frightened feeling as if something awful is about to happen: 10 I have lost interest in my appearance: Very definitely and quite badly Definitely Yes, but not too badly I don’t take so much care as I should A little, but it doesn’t worry me I may not take quite as much care Not at all I take just as much care as ever 4 I can laugh and see the funny side of 11 I feel restless as if I have to be on the things: move: As much as I always could Very much indeed Not quite so much now Quite a lot Definitely not so much now Not very much Not at all Not at all 5 Worrying thoughts go through my mind: 12 I look forward with enjoyment to things: A great deal of the time As much as I ever did A lot of the time Rather less than I used to From time to time bur not too often Definitely less than I used to Only occasionally Hardly at all 6 I feel cheerful 13 I get sudden feelings of panic: Not at all Very often indeed Not often Quite often Sometimes Not very often Most of the time Not at all 14 I can enjoy a good book or radio or TV 7 I can sit at ease and feel relaxed: programme: Definitely Often Usually Sometimes Not often Not often Not at all Very seldom NAME: DATE:
Circle the word that describes how your pain feels right now:
Nil Mild Moderate Severe Most severe
Circle the words below that best describe your current pain. Use only one word in each group. Leave out any group if the words are unsuitable.
1 2 3 4
Flickering Jumping Pricking Sharp Quivering Flashing Boring Cutting Pulsing Shooting Drilling Lacerating Throbbing Stabbing Beating Lancinating Pounding
5 6 7 8
Pinching Tugging Hot Tingling Pressing Pulling Burning Ithcy Gnawing Wrenching Scalding Smarting Cramping Searing Stinging Crushing
9 10 11 12
Dull Tender Tiring Sickening Sore Taut Exhausting Suffocating Hurting Rasping Aching Splitting Heavy
13 14 15 16
Fearful Punishing Wretched Annoying Frightful Gruelling Blinding Troublesome Terrifying Cruel Miserable Vicious Intense Killing Unbearable
17 18 19 20
Spreading Tight Cool Nagging Radiating Numb Cold Nauseating Penetrating Drawing Freezing Agonizing Piercing Squeezing Dreadful Tearing Torturing SF36 Health Survey INSTRUCTIONS: This set of questions asks for your views about your health. This information will help keep track of how you feel and how well you are able to do your usual activities. Answer very question by marking the answer as indicated. If you are unsure about how to answer a uestion please give the best answer you can. 1. In general, would you say your health is: (Please tick one box.) Excellent _ Very Good _ Good _ Fair _ Poor _ 2. Compared to one year ago, how would you rate your health in general now? (Please tick one box.) Much better than one year ago _ Somewhat better now than one year ago _ About the same as one year ago _ Somewhat worse now than one year ago _ Much worse now than one year ago _ 3. The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much? (Please circle one number on each line.) Activities Yes, Limited A Lot Limited A Little Not Limited At All 3(a) Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports Yes, Limited A Lot Limited A Little Not Limited At All 3(b) Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf Yes, Limited A Lot Limited A Little Not Limited At All 3(c) Lifting or carrying groceries Yes, Limited A Lot Limited A Little Not Limited At All 3(d) Climbing several flights of stairs Yes, Limited A Lot Limited A Little Not Limited At All 3(e) Climbing one flight of stairs Yes, Limited A Lot Limited A Little Not Limited At All 3(f) Bending, kneeling, or stooping Yes, Limited A Lot Limited A Little Not Limited At All 3(g) Waling more than a mile Yes, Limited A Lot Limited A Little Not Limited At All 3(h) Walking several blocks Yes, Limited A Lot Limited A Little Not Limited At All 3(i) Walking one block Yes, Limited A Lot Limited A Little Not Limited At All 3(j) Bathing or dressing yourself Yes, Limited A Lot Limited A Little Not Limited At All 4. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health? Yes No 4(b) Accomplished less than you would like Yes No 4(c) Were limited in the kind of work or other activities Yes No 4(d) Had difficulty performing the work or other activities (for example, it took extra effort) Yes No 5. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of any emotional problems (e.g. feeling depressed or anxious)? Yes No 5(a) Cut down on the amount of time you spent on work or other activities Yes No 5(b) Accomplished less than you would like Yes No 5(c) Didn’t do work or other activities as carefully as usual Yes No
6. During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbours, or groups? (Please tick one box.) Not at all _ Slightly _ Moderately _ Quite a bit _ Extremely _ 7. How much physical pain have you had during the past 4 weeks? (Please tick one box.) None _ Very mild _ Mild _ Moderate _ Severe _ Very Severe _ 8. During the past 4 weeks, how much did pain interfere with your normal work (including both work outside the home and housework)? (Please tick one box.) Not at all _ A little bit _ Moderately _ Quite a bit _ Extremely _ 9. These questions are about how you feel and how things have been with you during the past 4 weeks. Please give the one answer that is closest to the way you have been feeling for each item. (Please circle one number on each line.) 1. All of the Time 2. Most of the Time A Good Bit of the Time 3. Some of the Time 4. A Little of the Time 5. None of the Time 9(a) Did you feel full of life? 1 2 3 4 5 6 9(b) Have you been a very nervous person? 1 2 3 4 5 6 9(c) Have you felt so down in the dumps that nothing could cheer you up? 1 2 3 4 5 6 9(d) Have you felt calm and peaceful? 1 2 3 4 5 6 9(e) Did you have a lot of energy? 1 2 3 4 5 6 9(f) Have you felt downhearted and blue? 1 2 3 4 5 6 9(g) Did you feel worn out? 1 2 3 4 5 6 9(h) Have you been a happy person? 1 2 3 4 5 6 9(i) Did you feel tired? 1 2 3 4 5 6 10. During the past 4 weeks, how much of the time has your physical health or emotional problems interfered with your social activities (like visiting with friends, relatives etc.) (Please tick one box.) All of the time _ Most of the time _ Some of the time _ A little of the time _ None of the time _ 11. How TRUE or FALSE is each of the following statements for you? (Please circle one number on each line.) Definitely True Mostly True Don’t Know Mostly False DefinitelyFalse 11(a) I seem to get sick a little easier than other people 1 2345 11(b) I am as healthy as anybody I know 1 2 3 4 5 11(c) I expect my health to get worse 1 2 3 4 5 11(d) My health is excellent 1 2 3 4 5 Thank You! On the next 3 pages we would like you to tell us how often you have had problems with your mouth, teeth or gums in the last 3 months. Never Hardly ever Occasionally Fairly often Very often 1. Have you had trouble pronouncing any words because of problems with your teeth, mouth or dentures?
2. Have you felt that your sense of taste worsened because of problems with your teeth, mouth or dentures?
3. Have you had painful aching in your mouth?
4. Have you found it uncomfortable to eat any foods because of problems with your teeth, mouth or dentures?
5. Have you been self conscious because of problems with your teeth, mouth or dentures?
6. Have you felt tense because of problems with your teeth, mouth or dentures?
7. Has your diet been unsatisfactory because of problems with your teeth, mouth or dentures?
8. Have you had to interrupt meals because of problems with your teeth, mouth or dentures?
9. Have you found it difficult to relax because of problems with your teeth, mouth or dentures?
10. Have you been a bit embarrassed because of problems with your teeth, mouth or dentures?
11. Have you been irritable with other people because of problems with your teeth, mouth or dentures?
12. Have you had difficulty doing your usual jobs because of problems with your teeth, mouth or dentures?
13. Have you felt that life in general was less satisfying because of problems with your teeth, mouth or dentures?
14. Have you been totally unable to function because of problems with your teeth, mouth or dentures?
1. Do you have altered sensation on the affected side of your lip?
2. What type of sensation do you get on the affected side of your lip? numbness tingling more sensitive discomfort pain other describe
3. What causes these pain sensations in your lip? eating touching the affected area speaking temperature change brushing teeth just spontaneous other comment
4. How bad is the pain? This is a way of recording your pain. A mark at the no pain end of the line means you are completely free of pain. Marks along the line means gradually worse pain, until you get to the other end where your pain is unbearable. Please could you put a mark through the line at the place appropriate for your pain now.
No pain Unbearable pain
Never Hardly ever Occasionally Fairly often Very often 4. What causes these tingling sensations in your lip? eating touching the affected area speaking temperature change brushing teeth just spontaneous other comment
5. What causes these sensations of discomfort in your lip? eating touching the affected area speaking temperature change brushing teeth just spontaneous other comment
6. Do you bite or burn the affected side of your lip?
7. If you are a man, is your shaving affected by the changed sensation of your lip?
8. Do you have problems with dribbling due to the changed sensation of your lip?
9. Is your speech affected by the changed sensation of your lip?
10. Is your kissing affected by the changed sensation in your lip?
11. Any other comment?
Tick only positive ones
Provoking Factor Relieving Talking Eating Brushing teeth Shaving/washing Brushing hair/touching temples Cold/wind Warmth Foods cold or hot Pressure on teeth/biting Opening wide Stooping/bending Stress/tension/relaxing Sleep/rest Lying down Fatigue Distraction Working Alcohol Other please specify Associated factors: tick if present Presence Factor Presence Factor Altered/poor taste Clicking joint Disturbed salivation Bruxism Altered sensation/numbness Cheek clenching Sleep disturbance Unable to open wide Waking due to pain Ringing in the ears Colour change tissues/redness Deafness Swelling of face Headaches Nasal stuffiness/post nasal Dizziness drip Double or blurred vision Migraine with or without aura Excessive tearing of eyes Neck pain Excessive dryness of eyes Back pain Visual disturbances Irritable bowel Eye redness Nausea Fatigue/loss strength Abdominal pain/menstrual Stiffness of joints Impaired concentration Reduced appetite Other please specify
PAST TREATMENTS: Drugs Daily Dosage/ time Side effects Efficacy used
Previous surgery Other treatments: splints dental-cons endodontics, extraction, Alternative medicine, acupuncture/low intensity laser/TENS/homeopathy
Previous consultations/number: GP dentist oral surgeon neurologist psychiatrist ENT surgeon neurosurgeon psychologist pain specialist counsellor other EFFECT OF PAIN AND COPING:
Effect of pain on quality of life: none mild moderate considerable What changes have occurred in your life as a result of the pain:
Have you taken time off work: No/Yes how much:
How do people respond to your pain/is it helpful:
Do you feel anxious: no yes In the last month have you felt a lack of pleasure in life: no yes In the last month have you felt depressed: no yes Do you have: feeling of worthlessness/guilt/disturbed sleep/early am wakening/ appetite changes
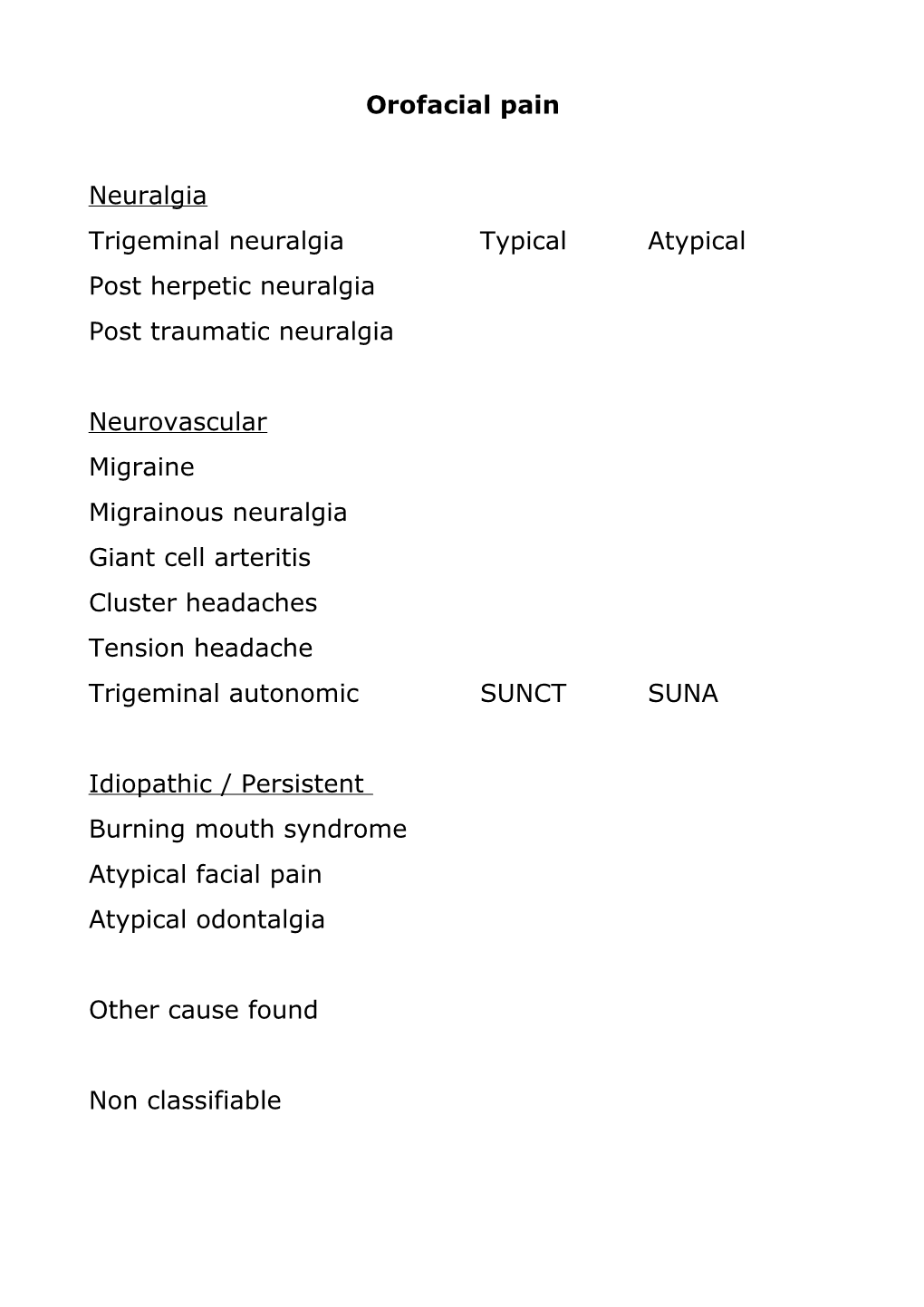
What do you think has caused the pain and what do you think I can do: Timing/Pattern of pain
Refractory period of no pain observed after a paroxysm of pain for few minutes
Sharp ,shooting
pain free paroxysm period al pain Refractory period of no pain observed after a mixture of sharp shooting and dull (burning) pain dull, burning
burni refractory Sharp ng pain free , period shooti ng
Continuous (persistent) dull aching pain in between each sharp attack
sharp Dull pain achin backgroug ndachin shootin g g Continuous low-grade dull pain aching or burning pain