FOREWORD
Since 1996, AIDS has become the principal cause of death in Namibia. In 1999 it accounted for 2,823 deaths or 28% of all deaths among hospitalised patients. HIV related disease is also a major cause of hospitalisation with a total number of 6878 hospitalisations during the same year. The number of persons diagnosed with HIV increased to over 14,000 new HIV positive diagnoses in 1999. Most of these persons will develop signs and symptoms of HIV disease over the coming years. The number of hospitalisations and deaths due to AIDS will therefore continue to increase considerably.
The provision of appropriate support for the increasing number of patients, families and communities affected by HIV/AIDS is the most important new challenge for the Ministry of Health and Social Services. This support includes counselling, community based and medical care to address the clinical problems of persons with HIV.
These guidelines will ensure a uniform high standard of care. Because treatment is standardised, drug supply can be rationalised and improved. These guidelines, together with other publications prepared by the Ministry on counselling and community based care, should be used by all staff of the Ministry. They also form an ideal basis for capacity building. In order to address the problem of HIV/AIDS, teamwork is essential, because the problems of persons affected with HIV are too complex for individual health or social workers to handle and are emotionally too demanding.
These guidelines will also facilitate the implementation of community based care for patients with HIV and AIDS as they equip health workers of clinics and hospitals with the necessary skills to manage patients, who are referred by community members.
It is my hope that these guidelines will provide a practical tool for all health workers of public and private health facilities, so that they can address the clinical problems of HIV/AIDS with confidence.
Dr. L. Amathila (M.P) MINISTER
i PREFACE
The Ministry of Health and Social Services would like to express sincere thanks and appreciation to the clinicians from the different regions and clinical specialists from the Windhoek Hospital Complex participating in the two workshops organised to draft and revise the guidelines. Special thanks go to Dr. F. Mugala, medical officer and chairperson of the AIDS committee at the Katutura Hospital for her input.
We greatly acknowledge the financial and technical support from the Commission of the European Communities for the organisation of preparatory workshops and production of these guidelines.
Although these guidelines have been developed after broad consultations with the input of experienced clinicians from peripheral hospitals and specialised services and with the use of the latest scientific literature, further adaptations will be needed to incorporate local experience and to include future scientific findings. The Ministry therefore appreciates receiving further contributions from clinical staff to keep these guidelines up to date.
Dr Kalumbi Shangula PERMANENT SECRETARY
ii ABBREVIATIONS
AIDS Acquired Immunodeficiency Syndrome AFB Acid fast bacilli BCG Bacillus Calmette-Guérin: an attenuated strain of tubercle bacilli used for the preparation of a vaccine bd Twice daily CMV Cytomegaly virus EC European Commission ENT Ear nose throat FUO Fever of Unknown Origin Hb Hemoglobin HIV Human Immunodeficiency Virus im Intramuscular iv Intravenous MCV Mean Cell Volume MOHSS Ministry of Health and Social Services NACOP National AIDS Co-ordination Programme OPD Out patient Department ORS Oral Rehydration Salt PCP Pneumocystis carinii pneumonia PID Pelvic Inflammatory Disease PHC & NS Primary Health Care and Nursing Services po Oral PPD Purified Protein Derivate (used for qid Four times daily STD Sexually Transmitted Diseases RBC Red Blood Cells TB Tuberculosis tds Tree times daily TMP-SMX Trimetoprim-Sulfamethoxazole or Co-trimoxazole WHO World Health Organization
iii TABLE OF CONTENTS
FOREWORD...... I
PREFACE...... II
ABBREVIATIONS...... III
TABLE OF CONTENTS...... IV
LIST OF TABLES...... VI
LIST OF FIGURES...... VI
INTRODUCTION...... 1
PART I: MANAGEMENT OF HIV DISEASE IN ADULTS...... 11
I.1 DIAGNOSIS OF HIV DISEASE ADULTS...... 11
I.2 PERSISTENT DIARRHOEA ADULTS...... 12
I.3 WEIGHT LOSS, MALNUTRITION AND WASTING ADULTS...... 19
I.4 ORAL MANIFESTATIONS OF HIV DISEASE - LEVEL 1 ADULTS...... 20
I.5 ORAL THRUSH – LEVEL 1 ADULTS...... 24
I.6 RESPIRATORY CONDITION ADULTS...... 28
I.7 OBSTETRICAL AND GYNAECOLOGICAL PROBLEMS...... 35
I.8 FEVER - LEVEL 1 ADULTS...... 38
I.9 HIV ASSOCIATED SKIN DISEASE ADULTS AND CHILDREN...... 42
I.10 LYMPHADENOPATHY – LEVEL 1 ADULTS...... 52
I.11 PAIN IN HIV DISEASE ADULTS...... 56
I.12 STEPWISE TREATMENT OF PAIN ADULTS...... 64
I.13 ANAEMIA IN HIV DISEASE ADULTS...... 66
I.14 GUIDELINES FOR FOLLOW-UP ADULTS...... 69
I.15 MEDICAL MANAGEMENT OF ADVANCED HIV DISEASE ADULTS...... 73
I.16 ANTIRETROVIRAL TREATMENT ADULTS...... 75
iv PART II MANAGEMENT OF HIV DISEASE IN CHILDREN...... 81
II.1 GENERAL CONSIDERATIONS REGARDING HIV INFECTION IN CHILDREN...... 81
II.2 DIAGNOSIS OF HIV DISEASE CHILDREN...... 84
II.3 PERSISTENT DIARRHOEA CHILDREN...... 86
II.4 ORAL THRUSH – LEVEL 1 CHILDREN...... 92
II.5 RESPIRATORY CONDITIONS LEVEL 1 CHILDREN...... 96
II.6 PERSISTENT OR RECURRENT FEVER – LEVEL 1 CHILDREN...... 102
II.7 FAILURE TO THRIVE – LEVEL 1 CHILDREN...... 106
II.8 LYMPHADENOPATHY – LEVEL 1 CHILDREN...... 110
II.9 HIV INFECTIONS AND BREASTFEEDING...... 112
II.10 HIV INFECTION AND IMMUNIZATION...... 113
II.11 PALLIATIVE CARE CHILDREN...... 114
II.12 FOLLOW - UP CHILDREN...... 117
II.13 ANTIRETROVIRAL TREATMENT CHILDREN...... 120
v LIST OF TABLES
Table 1: List of clinical conditions by clinical stage 7 Table 2: Continuum of Care in the Management of HIV Disease and AIDS 9 Table 3: Assessment of dehydration 13 Table 4: Aetiology and treatment of persistent diarrhoea in patients with HIV 18 Table 5: Oral manifestations in HIV disease 22 Table 6: Contraceptive methods and pregnancy failure rate 37 Table 7: CNS Conditions 62 Table 8: Differential Diagnosis of Lower Extremity Symptoms in HIV Infection 63 Table 9: Analgesic drugs recommended for pain in HIV disease 65 Table 10: Treatment of Anaemia in HIV disease 68 Table 11: Advantages and limitations of HAART 76 Table 12 Antiretroviral drug regimes for HAART 77 Table 13 Diagnostic tests for HAART 78 Table 14: HIV paediatric classification system based on CD4 percentage 83 Table 15: HIV paediatric classification system: clinical categories 85 Table 16: Assessment of dehydration in children 87 Table 17: Clinical assessment of respiratory distress 100 Table 18: Immunisation in HIV infected children 113 Table 19: Dosage of analgesic drugs in children 115 Table 20: Recommended doses of Vitamin A in children 118 Table 21: Recommended doses of co-trimoxazole for PCP prophylaxis 119 Table 22: TB Prophylaxis in HIV infected children 119
LIST OF FIGURES
Figure 1: Natural history of HIV disease 4 Figure 2: The interdisciplinary team and its partners 10 Figure 3: Estimated rates and timing of Mother to Child Transmission of HIV 74 Figure 4: CD4 cell counts and viral load in perinatally HIV infected children 83 Figure 5: “Faces scale” used to measure pain effect in children 122
vi INTRODUCTION
1. Purpose of the guidelines The guidelines for clinical management of HIV/AIDS, which are presented here, address the clinical management of the HIV infected person in a simple form. They are meant for different levels of health care to assist health workers in making accurate diagnosis, giving correct treatment and facilitate adequate planning. It is a problem-solving manual that addresses mainly symptomatic problems and clinically identifiable diseases.
These guidelines are expected to serve the following purposes:
To assist health workers in the diagnosis and clinical management of symptomatic HIV infected persons. To give support to health workers faced with a new dimension of decision making with regard to the severity of the disease and multiplicity of presenting complaints and pathogens. To reduce the economic burden of HIV infection by preventing excessive use of diagnostic tests and inappropriate treatment. To serve as a teaching aid for health workers at different levels.
Realising the differences in the available health care facilities in Namibia, these guidelines have identified two different levels of care:
Level 1: clinics, health centres or hospital out patient (screening) departments, as well as home based care programmes.
Level 2: hospitals or health centres with laboratory services, X-ray and sometimes more advanced diagnostic facilities.
These “levels” are not absolute: sometimes “ Level 1” may have some laboratory facilities or “ Level 2” has to make a diagnosis on clinical grounds only and functions as “Level 1”. It should be realised that “Level 1” can refer patients to “Level 2”. When a patient has been managed at this level and no further diagnostic or therapeutic interventions are required, the patient should be referred back to “Level 1” with adequate advice for further management and follow-up.
The management of HIV disease in children differs in some aspects from the management in adults: some clinical manifestations are specific for children (such as failure to thrive) the aetiology of clinical manifestations may be different (such as Lymphocytic Interstitial Pneumonitis in children) the dose of drugs should usually be adapted to the weight or age of the child.
Where appropriate the guidelines are presented in the form of flow-charts or algorithms to facilitate decision-making.
Introduction 1 2. How to use clinical algorithms or flow charts
Clinical algorithms or flow charts are maps, which read from top to bottom of the page and from left to right. The maps use only the three following symbols:
Clinical condition
Clinical state or problem definition box: This box defines the clinical state or problem. It has only exit path and may or may not have an entry path. This type of box always appears at the beginning of an algorithm.
Decision box
Diagnostic decision box: This box contains information necessary for some sort of branching decision. It always has an entry path and at least two exit paths.
Action box
Action box: This box indicates an action: Usually the action is therapeutic, sometimes it is diagnostic, e.g. microscopic stool examination.
Continuation Box
Continuation Box: This box indicates a continuation of a previous flow-chart.
Capital letters in brackets within a box refer to the annotations or comments on the facing page. These are an essential part of the algorithm, since not all of the information needed to use it can be provided in graphic form or within the boxes. The boxes are also numbered for easy reference.
A careful history should always be taken and a physical examination carried out before an algorithm is applied.
Introduction 2 The reader is advised to make use of the following techniques in studying the algorithms:
Read the algorithm through without reading the annotations in order to understand the logic flow. A clinician experienced in managing HIV infections should not expect to agree with everything in the algorithms, as there are often more ways than one in which it can be written.
Read the algorithm again slowly, paying careful attention both to the annotations and the endpoint of each branch.
Apply the algorithms to your practical experience in the clinical setting in order to learn how it works.
Test the clinical algorithms in the clinical setting. It may be useful to focus first on one clinical problem (such as diarrhoea) and compare if there are differences with the way you are used to handle this problem. Make annotations.
Encourage regular consultations and discussions on practical implications of applying the guidelines with colleagues and at relevant meetings.
Clinical care of HIV disease will continue to change as a result of new scientific findings. Guidelines will need to be refined to incorporate the results of future operational studies on the aetiology and treatment of common HIV related problems in different parts of the country. Users of these guidelines are therefore invited to give feedback to the National AIDS Co-ordination Programme about any issues needing clarification or updating.
Introduction 3 3. The natural course of HIV disease in adults
The virus spreads from one person to another usually through sexual intercourse, direct exposure to contaminated blood, or transmission from a mother to her unborn child or suckling infant. In the body, HIV invades certain cells of the immune system--including CD4, or helper T lymphocytes--replicates inside them and spreads to other cells. (These lymphocytes, named for the display of a molecule called CD4 on their surface, are central players in immunity.)
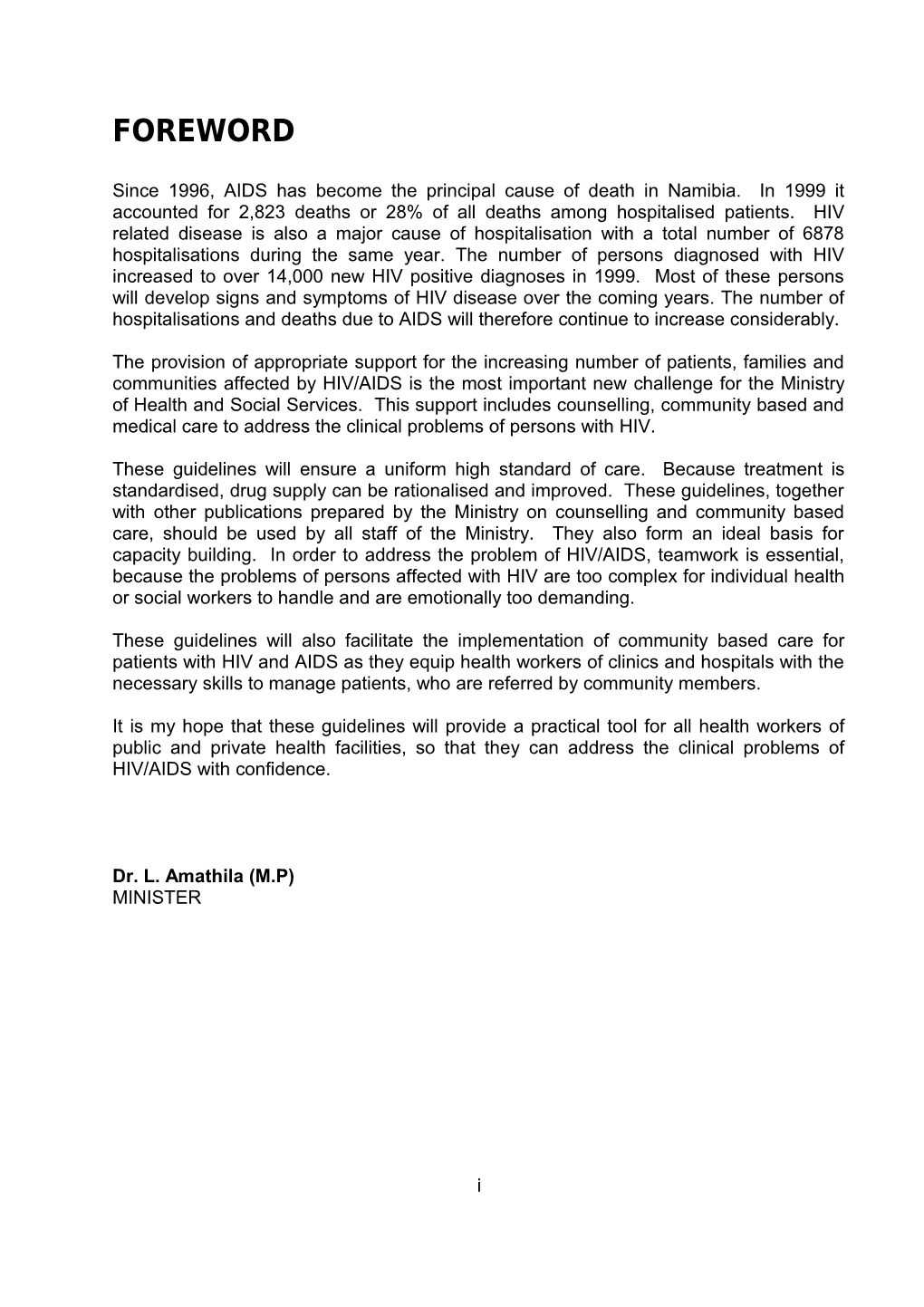
The following 3 phases can be distinguished during the natural course of HIV infection (see fig 1). 1. Early infection and sero-conversion (2-4 months). At this stage the viral peaks. The number of CD4 T cells, the immune cells most damaged by the HIV virus, drops. Antibodies are not yet present. The person might therefore be highly infective, while the HIV blood test is negative. 2. Chronic phase of about 8-10 years. During this period most patients have no symptoms. Some curable infections may occur during this stage. Some of these illnesses may be life threatening if they are not adequately treated. 3. The virus gains the upper hand when the CD4 T cell level drops below 200 cells per ml of blood1. Opportunistic infections and other complications usually occur only when CD4 levels have dropped to about 50-100 cells/ml. The clinical diagnosis of AIDS is usually made at this final stage.
Figure 1: The natural course of HIV disease
Seroconversion Infection Death
1200
1000 106 ) d o
o 800 l Antibodies to HIV 5 b
10 f T o
N r
U CD4 cells e t O e C
m 600 i
L 4 l
l Viral load L i 10 E m
C
c i 4 b D u C c 400 3 r
e 10 p
s l l e C ( 200 102
0 0 4wks 8wks 12wks 1yr 2yrs 3yrs 4yrs 5yrs 6yrs 7yrs 8yrs 9yrs 10yrs 11yrs 12yrs ACUTE PHASE CHRONIC PHASE AIDS Clinical stages Stage 1 Stage 2 Stage 3 Stage 4
Introduction 4 Early infection and sero-conversion At the start of an infection, hefty viral replication and the killing of CD4 T cells cause high levels of HIV in the blood and a dramatic drop in CD4 T cell concentrations from the normal level of at least 800 cells per ml of blood. About three weeks into this acute phase, about half of the people have flue-like symptoms, such as fever, muscle pain and headaches. These usually disappear within one to three weeks, as the immune system starts to gain some control over the virus: Cytotoxic (or CD8) T cells are stimulated to increase the killing of infected, virus-producing cells. The body produces antibody molecules, which bind to free HIV particles (outside the cells). HIV tests, which are based on the detection of these antibodies, now become positive. The body speeds up the production of CD4 cells and the CD4 T-cell count rebounds.
Chronic phase By about three to six months a new balance has been reached and the disease enters into its chronic stage. In this prolonged, chronic stage, most people feel good and show few, if any, symptoms. This second stage accounts for about 80 percent of the time between HIV infection and death. The rate of viral replication reaches a lower, but relatively steady, state that is reflected in the maintenance of viral levels at a kind of "set point." To maintain this steady state, about 100 to 1,000 million virus particles must be produced and cleared each day2. This set point varies greatly from patient to patient and dictates the subsequent rate of disease progression. The body continues to produce high numbers of CD4 T cells, so that levels remain high enough to respond to other pathogens. Opportunistic infections do not occur during this period. Over time, however, CD4 T cell concentrations gradually fall. On average, eight to ten years pass before a major HIV-related complication develops.
Severe immunodeficiency and AIDS When the CD4-level drops below 200 cells per ml of blood, the occurrence of opportunistic infections and other complications increases. This laboratory finding is used by the US Centres for Disease Control as a definition for AIDS. It is also an indicator to start prophylactic treatment. As levels dip under 100, the balance of power shifts away from the immune system. HIV levels increase rapidly, and microbes that the immune system would normally control begin to multiply extensively, giving rise to the potentially deadly opportunistic infections (such as Pneumocystis carinii pneumonia and Toxoplasmosis encephalitis). Opportunistic infections may occur before the CD4 T cell level falls under 200. The appearance of these infections leads to a clinical diagnosis of AIDS, regardless of the CD4 T cell level.
During the final phase of HIV disease, the concentration of HIV virus particles in the blood increases. CD4 levels drop further and antibody levels decline and HIV serologic tests may even become negative.
Introduction 5 Variation in the course of HIV disease Although patients typically survive HIV infection for 10 or 11 years, the course can vary enormously. Some die within two years after contracting the virus, whereas an estimated 4 to 7 percent maintain fully normal CD4 T cell counts for eight years or more and survive beyond 20 years. Some patients remain free of serious symptoms and complications until they have reached an advanced stage of immuno-suppression, while others suffer debilitating malaise and fatigue or frequent non-life threatening complications throughout their infection.
The natural course of HIV infection is influenced by several factors, including:
The host: Age of the infected person: disease progresses slower in young patients. Genetic factors: some persons are less susceptible to the virus or their immune system reacts more effectively. The virus: Some viral strains are more virulent than other Multiple re-infections may speed-up the progression of the disease. Environmental factors: Exposure to other infections and malnutrition speed up disease progression. Prevention and early treatment of infections and good nutrition help to sustain the immune system.
The following measures allow the natural course of HIV disease to be slowed down and help to sustain the immune system: Prevention of HIV re-infection (abstinence or condom use during sexual intercourse) Prevention of infections (for example: using safe drinking water, prevention of other sexually transmitted infections) Screening and treatment of latent infections (for example latent syphilis) Supportive measures (adequate nutrition, rest, vitamin supplements) Early treatment of common infections (skin infections, respiratory infections) Early treatment of opportunistic infections Prophylactic treatment for opportunistic infections (for example for Pneumocystis carinii pneumonia, Toxoplasmosis, tuberculosis,) Antiretroviral treatment with a combination of at least 3 drugs.
Clinical stages The phases of HIV disease are mainly based on a combination of laboratory data (CD4 cells, viral load) and clinical findings. There is a correlation of CD4 cell counts with different infectious and non-infectious complications. Based on this correlation, a clinical staging system for HIV disease has been developed by WHO which may be useful to assess the progress of disease in the absence of facilities for CD4 testing (see Table 1). The clinical manifestations of advanced HIV disease (including those foreseen in the Namibian AIDS case definition) usually develop around CD4 levels below 100 cells/ml. The median time from severe immuno-depression (as defined by CD4<200 cells/ml) to an AIDS-defining clinical diagnosis is about 12-18 months.
Introduction 6 Table 1: List of clinical conditions by clinical stage Clinical stage 1 1. Asymptomatic infection 2. Persistent generalised lymphadenopathy 3. Acute retroviral infection Performance scale 1: asymptomatic, normal activity. Clinical stage 2 4. Unintentional weight loss, < 10% of body weight 5. Minor mucocutaneous manifestations (e.g. seborrheic dermatitis, prurigo, fungal nail infections, oropharyngeal ulcerations, angular cheilitis) 6. Herpes zoster, within the previous 5 years 7. Recurrent upper respiratory tract infections (e.g. bacterial sinusitis) and/or Performance scale 2: symptoms, but nearly fully ambulatory. Clinical stage 3 8. Unintentional weight loss, > 10% of body weight 9. Chronic diarrhoea, > 1 month 10.Prolonged fever (intermittent or constant) > 1 month 11.Oral candidiasis (erythematous or pseudomembranous) 12.Oral hairy leukoplakia 13.Pulmonary tuberculosis (typical or atypical), within the previous year 14.Severe bacterial infections (e.g. pneumonia, pyomyositis) 15.Vulvovaginal candidiasis, chronic (> 1 month) or poorly responsive to therapy and/or Performance scale 3: in bed < 50% of normal daytime, but > normal, during previous month. Clinical stage 4 16.HIV wasting syndrome 17.Pneumocystis carinii pneumonia 18.Toxoplasmosis of the brain 19.Cryptosporidiosis with diarrhoea, > 1 month 20.Isosporiasis with diarrhoea, > 1 month 21.Cryptococcosis, extrapulmonary 22.Cytomegalovirus disease of an organ other than liver, spleen or lymph node 23.Herpes simplex virus infection, mucocutaneous (> 1 month) or visceral (any duration) 24.Progressive multifocal leukoencephalopathy 25.Any disseminated endemic mycosis (e.g. histoplasmosis, coccidioidomycosis) 26.Candidiasis of the oesophagus, trachea, bronchi or lungs 27.Atypical mycobacteriosis, disseminated 28.Non-typhoid Salmonella septicaemia 29.Extrapulmonary tuberculosis 30.Lymphoma 31.Kaposi’s sarcoma 32.HIV encephalopathy and/or Performance scale 4: in bed > 50% of normal daytime during previous month.
Introduction 7 4. Continuum of care in the Management of HIV disease
The transition from active to palliative care is not something that happens at a single point in time. It is a process and its dynamics are different in every patient. Palliative care is most successful when it is initiated early in the disease process, as the necessary relationships take time to develop.
Some patients may die as a consequence of their first HIV manifestation, such as cryptococcal meningitis. Most persons with HIV infection, however, will experience an increasing frequency of health problems and finally reach a stage of severe immune suppression over a period of several years. While HIV disease progresses, the attention for symptomatic relief will gradually become more important than curative or causal treatment (see table 2).
The conclusion to stop causal treatment should only be made on the basis of careful investigations for the specific problems, described in these guidelines, or after a period of follow-up whereby severe immuno-deficiency has been confirmed. So two types of criteria are required: The patient has had a long course of progressively worsening illness, i.e. that the patient is in an advanced stage of immuno-deficiency. Everything possible has been done to investigate and manage the specific conditions from which the patient is suffering and that the patient despite adequate management continues to deteriorate.
Each individual patient has particular needs at the final stages of HIV disease. At this terminal stage, care will mainly focus on palliation of symptoms and emotional support.
Patients diagnosed with HIV/AIDS face loss at every level: physical health, independence, career and status, normal family life, predictability and future, motivation and meaning. The diagnosis itself is a traumatic experience. Knowledge and understanding of crisis and the feelings of denial, anger, depression and helplessness are important, as the reality of the patient's life changes within seconds. In addition to any other life-threatening health problems, HIV raises questions about previous and present sexual relationships and partners. These questions are highly emotional and only few health and social workers feel confident to discuss these.
Introduction 8 Table 2: Continuum of Care in the Management of HIV Disease and AIDS
MEDICAL MANAGEMENT
PALLIATIVE CARE D Stages of Early HIV Intermediate HIV Advanced HIV HIV disease disease (stage 3) disease or AIDS disease (stage 2) (stage 4) Clinical Frequent Infections with Combination of problems infections with common and health problems common opportunistic (e.g., chronical E pathogens pathogens diarrhoea, weight loss, fever, anaemia) General Mobile and Mostly mobile with Patients often at condition active. Rapid increasing periods of home or in bed response to illness A treatment
Medical Curative anti- Curative or causal Supportive treatment infectious treatment. treatment (skin treatment Consider prophylaxis lesions, anaemia or maintenance diarrhoea etc.), T treatment. maintain nutrition. Supportive treatment Discontinue (skin lesions, causative treatment anaemia, nutrition, and prophylaxis? vitamins) Palliative Analgesics, Analgesics, Narcotic analgesics care antipyretics antipyretics where needed Pre- and post- Follow-up counselling Continuous (home) test with family members. nursing care H counselling. Address social issues Terminal counselling Involve family Nursing care during and support member(s) or periods of illness other person of confidence
Due to the complexity of HIV related problems it is impossible for individual health or social workers to adequately address these. To support persons and families affected by HIV is emotionally very demanding. It is therefore essential to establish interdisciplinary teams to deal with these problems. The core of the interdisciplinary team is the medical, nursing, counselling and social services. Other services may be available as full-time members or on a consultative basis. Team members share information through discussion.
Introduction 9 Figure 2: The Interdisciplinary Team and its Partners
Community initiatives
Volunteers
Medical
Counselling social worker Nursing health staff spiritual
Private sector, NGOs, etc.
The patient is in the centre of this figure. The skills and interests of team members are complementary and partly overlapping. The team’s close collaboration with Volunteers and Community Based support groups is essential for its success.
The identity of the team as a whole is more important than individual identities. Leadership is assumed by the different team members depending on the task at hand. The team works closely together with volunteers and community based initiatives. Because the team is the vehicle for action, the interactional process is vital for success.
For more information on these issues we refer to the guidelines on counselling and the handbook on community and home based care. In these guidelines we focus further on the clinical aspects of palliative care.
Introduction 10 PART I: MANAGEMENT OF HIV DISEASE IN ADULTS
II.1 DIAGNOSIS OF HIV DISEASE ADULTS
The aim of this chapter is to help the health workers to recognise adult patients with possible symptomatic HIV disease. As explained in the introduction, patients with HIV disease may have only minor health problems or advanced HIV disease when the diagnosis is considered.
Any of the infections or clinical manifestations listed in table 1 may be an indication for HIV testing. Although symptomatic HIV infections may sometimes be recognised clinically (in particular when the presence of opportunistic infections has been confirmed), HIV testing should be done wherever possible to confirm the clinical suspicion. HIV testing is not only important for the management of the patient, but also for referral and counselling of sexual partners.
The laboratory request form includes information on the age, sex as well as the reason for testing and the main HIV related clinical manifestations. This information is compiled and analysed by the Ministry of Health and Social Services at regular intervals and constitutes one of the main instruments for surveillance of the HIV/AIDS epidemic in Namibia. It is therefore important for all clinicians to thoroughly complete each laboratory request form.
At present, most persons have symptomatic or advanced HIV disease at the time of HIV diagnosis. Increasingly, however, HIV disease will be diagnosed at earlier stages due to improved counselling, partner referral and voluntary testing. Early HIV diagnosis has the advantage that it facilitates the timely and appropriate recognition and treatment of symptoms and complications. Moreover, promotion of positive living with HIV, including improved hygiene, a balanced diet and prophylactic treatment may further delay the onset of symptoms. Early diagnosis of HIV infection also contributes to a reduction of HIV transmission to uninfected partners.
Receiving an HIV positive diagnosis has a profound impact of any person's life. This impact is even more important in otherwise healthy persons. Adequate preparation of the person for the diagnosis is important to facilitate acceptance and positive living. Appropriate counselling, ensuring informed consent, confidentiality and non-discrimination are essential components of this process.
Clinicians are often in a privileged position to explain to patients why an HIV test is considered, how the result will be used improve clinical management and that any fear for discrimination by health workers is ungrounded. Some explanations by the clinician on the procedures for testing and follow-up by the team of the health facility will further facilitate the acceptance of counselling and testing.
Because the majority of patients present with symptoms or return for follow-up after treatment of symptomatic disease, the guidelines start with the management
PART 1-ADULTS 11 of specific clinical problems. Guidelines for follow-up of symptomatic and asymptomatic adults with HIV are found at the end of part 1.
PART 1-ADULTS 12 II.2 PERSISTENT DIARRHOEA ADULTS
PERSISTENT DIARRHOEA (A)
History and physical examination
Correct with oral rehydration YES Dehydrated salts (oral or ? naso-gastric (B) tube) or parenteral fluids
NO
1. Maintain hydration (C) Hydration YES 2. Consider supplemental feeding and general as tolerated condition improved?
NO
Continue Refer to Level 1 Level 2
PART 1-ADULTS 13 ANNOTATIONS FOR PERSISTENT DIARRHOEA ADULTS
A: Definition:
Liquid stools 3 or more times a day, continuously or intermittently for more than two weeks, in a patient with HIV infection.
B: Diarrhoea occurs at some point in the clinical course of most HIV infections, and the incidence and duration of diarrhoea increases during the course of HIV disease.
C: The management of acute diarrhoea should follow standard treatment guidelines (see Treatment manual for clinics and national guidelines on the management of diarrhoea). Also for persistent diarrhoea, maintenance of adequate hydration and ensuring the electrolyte balance is the first priority, preferably by means of oral fluids.
Table 3: Assessment of dehydration
Clinical features Moderate Severe
General appearance/ Restless, irritable Usually conscious; cold, condition Apprehensive, Sweaty cyanotic extremities
Pulse Rapid Rapid, feeble, Sometimes impalpable
Respiration Deep, may be rapid Deep and rapid
Skin elasticity Pinch retract slowly Pinch retract very slowly (>2 seconds)
Eyes Sunken Deeply sunken
Mucous membrane Dry Very dry
Urine flow Reduced amount and dark None passed for 6 or more hours; bladder empty
C: Potassium is readily available in fruits like oranges, bananas and local fruits. ORS also contains sufficient potassium to maintain a good electrolyte balance.
PART 1-ADULTS 14 PERSISTENT DIARRHOEA – LEVEL 1 ADULTS
Contin ue from Page 12
Persistent YES diarrhoea with blood? (A)
NO
Treat with Co-trimoxazole 2 Treat with Nalidixic Acid, tabl bd for 5 days (C) 1g qid for 5 days (B) Continue supportive Continue supportive treatment (fluids, diet) treatment (fluids, diet)
YES Diarrhoe a Improve d? NO
Maintain hydration and Treat for anaemia if nutrition needed Refer to level 2 Follow up
PART 1-ADULTS 15 ANNOTATIONS FOR PERSISTENT DIARRHOEA – LEVEL 1 ADULTS
A: If a patient has no other problem than diarrhoea without blood, the majority of patients may improve on fluid replacement only and not need any antibiotics.
B: In patients with persistent bloody diarrhoea Nalidixic Acid 1g qid for 5 days should be given. Other common causes of bloody diarrhoea should also be considered according to the prevalence in the area (e.g. Amoebiasis and Bilharzia). In areas with high prevalence of Amoebiasis for example, Metronidazole 400 mg tds for 10 days should be given as well. Fluid replacement and appropriate nutrition should be continued.
C: For those who were not yet treated with antibiotics, Co-trimoxazole 2 tabl. bd for 5 (TMP-SMX: 80 mg trimethoprim plus 400 mg sulfamethoxazole) may be given at this stage. In case of relapse, prolonged treatment up to 3 weeks may be required. In areas where Giardiasis is common, Metronidazole 400 mg bd for 5 days should be given as well. Fluid replacement and appropriate nutrition should be continued.
D: Patients not responding to the above mentioned therapy should be referred for further examination and treatment of a possible underlying cause. After all required examinations have been done and necessary treatments have been given, constipating agents may be prescribed at level 2. These patients may be referred back to level 1 for continuation of this treatment.
Constipating agents should never be used in: Patients with bloody diarrhoea (because of the risk of inducing toxic megacolon) Elderly patients Children
PART 1-ADULTS 16 PERSISTENT DIARRHOEA – LEVEL 2 ADULTS Referred patient with persistent diarrhoea not responding to treatment prescribed at level 1
Stool examination (X 3) (A) Bacterial: (B) Give antibiotics as indicated
Are laboratory and/or clinical findings consistent Protozoal: (B) with: YES Bacterial infection (fever, Metronidazole 400 blood, or leukocytes in mg bd for 5 days stool) OR OR tds for 10 days Protozoal infection (Amoebiasis, Giardiasis) Helminthes Helminths: (B) (See also Table 2) Albandazole 400 mg/day for 3 days (repeat after 3wks)
NO YES Improved?
NO
Give constipation agents as tolerated (C)
YES Improve d? NO
1. Stop all drugs Follow 2. Maintain hydration up as 3. Maintain nutrition needed (D)
PART 1-ADULTS 17 ANNOTATIONS FOR PERSISTENT DIARRHOEA – LEVEL 2 ADULTS
A: Multiple stool examination (up to 3 samples) increases the diagnostic yield of parasites.
B: Bloody diarrhoea that does not respond to the usual treatment at level 1 (Nalidixic Acid) and is not caused by Amoebiasis may be due to Campylobacter. This infection should be treated with Erythromycin (500 mg po qid for 7 days). Toxic symptoms (fever, low blood pressure, high pulse rate, pallor) in patients with diarrhoea and previous antibiotic treatment should raise suspicion of an intestinal Clostridium difficile infection. Diagnosis is mainly based on clinical grounds, as confirmation by culture or detection of toxines by ELISA is not available in most facilities. Treatment consists of immediate stopping of all antibiotics and administration of oral Metronidazole 400 mg tds for a total of 10 days. Clinical response is usually good if treatment is started early, but relapse may occur.
Protozoal infections should be treated with Metronidazole. Five days 400 mg bd po for Giardiasis and 10 days 400 mg tds po for Amoebiasis. Isospora belli usually requires prolonged treatment with Co-trimoxazole (2 tabl. po bd for 21 days) to reduce the occurrence of relapses.
In patients with HIV and diarrhoea, treatment of possible worm infections should be considered. This should include treatment for Strongyloides stercoralis, an infection that is often not diagnosed by stool examination and requires a high dose of anthelmintic drugs: Albendazole 200 mg 2 tabl. once daily during 3 days, repeated after 3 weeks.
C: If microscopic examination does not identify any pathogen, lactose intolerance should be considered. In this case, diarrhoea will improve with a lactose-free diet. Constipating agents may be tried, for example, Loperamide 2 mg, 2 tabl. after each loose stool (max 10 tabl. per day). Constipating agents should not be used in: Patients with bloody diarrhoea (because of the risk of inducing toxic megacolon) Elderly patients Children.
In about 50% patients with persistent diarrhoea and HIV/AIDS no treatable infectious agents can be identified. Maintenance of hydration and adequate nutrition (including fruits and vegetables for potassium) are the most important form of management. If potassium-rich food is not available, potassium supplement may be needed).
PART 1-ADULTS 18 Table 4: Aetiology and treatment of persistent diarrhoea in patients with HIV 1. Infectious Aetiology Clinical signs Diagnosis Therapy Parasites
Giardia lamblia Diarrhoea Fresh stool Metronidazole 400 mg microsc. tds for 5 days (+aspirate upper E. histolytica Diarrhoea + GIT) Metronidazole 400 mg blood tds for 10 days Fresh stool Strongyloides microscopy Albendazole 400 mg stercoralis. Diarrhoea + once daily for 3 days blood Fresh stool Isospora belli microscopy Co-trimoxazole 2 tabl. bd for 7–21 days Diarrhoea Fresh stool Cryptosporidiu microscopy No curative therapy34 m Diarrhoea Fresh tool (AFB Metronidazole 500mg Microsporidium stain) tds Diarrhoea Albendazole 800mg bd Fresh stool microscopy Bacteria
Salmonella Diarrhoea + Stool microscopy Chloramphenicol 250- species fever + blood + 500 mg qid, for 7-14 d culture+haemocu Shigella Diarrhoea + lture Nalidixic Acid 1g qid for species blood + fever 5 days Stool microscopy Diarrhoea + + culture Erythromycin 500mg qid Campylobacter blood +fever for 7 days Stool microscopy Diarrhoea + + culture Stop other antibiotics Clostridium fever Manage toxic shock difficile Stool microscopy Metronidazole 400 mg + culture p.o tds for 10 days.
Cefuroxime 750 mg tds Diarrhoea + for 7 days E Coli fever Stool microscopy + culture Viruses
CMV Diarrhoea + Biopsy No etiologic therapy blood available
PART 1-ADULTS 19 HIV Diarrhoea No etiologic therapy available 2. Malignancies such as Kaposi Sarcoma or lymphoma
3. Idiopathic (possibly HIV infection)
PART 1-ADULTS 20 II.3 WEIGHT LOSS, MALNUTRITION AND WASTING ADULTS
Serious weight loss is a problem for many people with AIDS. It is caused by HIV infection, other infections and medical treatments. Weight loss is also caused by not eating enough nutritious food. This can be the result of nausea, a sore mouth, no appetite, diarrhoea, vomiting, depression or poverty.
The absorption of nutrients into the blood mainly takes place in the small intestine. With AIDS, the body may lose its ability to absorb nutrients properly. Diarrhoea further reduces absorption, because food does not stay long enough in the system to be absorbed. When the body cannot absorb the nutrients, it must use its stored energy, it’s fat and muscle to keep functioning. The muscles start to break down and there is wasting of the body.
Exercise is important for preventing weight loss and wasting because it stimulates the appetite, reduces nausea, improves the functioning of the digestive system and strengthens muscles.
Foods to stimulate weight gain should have a high protein content and include: Avocados, coconut, full-cream milk powder, yoghurt or sour milk, soya products, cheese, meat, fish, chicken, peanut butter, nuts and seeds, dried fruit, eggs, beans, lentils, potatoes, sweet potatoes, bananas, olives, cassava, millet, sorghum, oats, rice, barley, wheat, maize. Avoid refined sugar and sweets, as these increase the risk of dental and oral problems.
Some tips to facilitate digestion of food: Squeeze fresh lemon juice over fatty foods like meat, chicken and nuts. Add the grated skin of oranges and lemons to fatty foods. To help digest meat, eat papaya (pow-pow) with the meat. Eat many small meals a day and chew food well Drink between meals, not with meals. Eat fermented or sour foods such as sour milk, sour porridge, etc.
Supportive diet for patients with diarrhoea: Diarrhoea disturbs the intestinal flora. Replace this by drinking sour porridge or yoghurt. Carrot soup helps to replace vitamins and minerals. Carrot soup contains pectin. It soothes the bowels and stimulates the appetite. Drink lots of fluids. Drink water, soups and diluted fruit juices. Foods that help reduce diarrhoea are rice, potatoes, watermelon, and steamed fruits. Avoid raw foods, cold foods, fatty foods, high-fibre foods, milk and food containing much fat. Drinking water may be an important source of infection even when others can drink it without problems. Drink boiled water or tea when possible.
N.B. All dietary recommendations should be adapted to local circumstances.
PART 1-ADULTS 21 II.4 ORAL MANIFESTATIONS OF HIV DISEASE - LEVEL 1 ADULTS
ORAL MANIFESTATION IN A PERSON WITH HIV (A)
White plaques YES on oral mucosa, Oral thrush. bleeding when Go to page 22 removed?
NO Analgesics (B) YES Oral hygiene (C) Ulcers or blisters Herpes simplex or Refer in case of Aphthous ulcers severe aphthous ulcers (D)
NO
Peroxide 3% (or Bleeding and YES Acute necrotising Chlorhexidin) painful ulcers of gingivitis PLUS the gingiva Metronidazole 400mg bd p.o. for 5 days (E) NO
YES Red or purple Kaposi sarcoma Refer for further nodular lesions investigation and treatment (F)
NO
Other oral manifestations
Refer for further investigation and treatment (G)
PART 1-ADULTS 22 ANNOTATIONS FOR ORAL MANIFESTATIONS – LEVEL 1 ADULTS
A: Oral manifestations are common in persons with HIV disease. Up to 70% of persons with HIV or AIDS develop oral manifestations during the course of the disease. In many patients oral manifestations are the first manifestation of HIV disease. Oral manifestations often cause serious discomfort and contribute to malnutrition and weight loss. Most oral manifestations respond well to adequate treatment. Appropriate hygiene and eating habits reduce the incidence and recurrence of oral manifestations.
B: Multiple blisters and superficial ulcers on the lips and oro-pharingeal mucosa are mostly caused by Herpes simplex virus. Single painful ulcers of less than 2cm diameter with a yellowish base and red inflamed border are called aphthous ulcers. Both conditions are self-limiting and will usually heal within a period of 2 weeks. Provide symptomatic treatment with Aspirin or Paracetamol 4-6 times daily and oral hygiene.
C: Oral hygiene includes the following measures: Brushing of teeth with a toothbrush and toothpaste or by brushing with a traditional stick. Avoid refined sugar and sweets. Stimulate the saliva with sugar free chewing gum or palm leaves in case of a dry mouth. Consult a dentist in case of toothache. Because teeth may also be damaged in the absence of symptoms, it is advisable to consult a dentist at the time of HIV diagnosis and at least annually thereafter.
D: Severe aphthous ulcers and frequent recurrence of these ulcers cause serious discomfort and deterioration of the general nutritional status. These patients should therefore be referred to level 2 for further treatment.
E: Acute necrotising ulcerative gingivitis (ANUG) is chacterised by a rapid onset, spontaneous bleeding of the gums and severe pain. It is easily recognised by destruction of the interdental gum, which is covered by whitish pseudo-membranes. This destruction causes a characteristic foul smell. ANUG may lead to rapid loss of teeth. Refer patients where possible to a dentist for thorough local removal of bacteria and diseased tissue. Early cleaning of the gingiva with a cotton tip soaked in peroxide 3% in order to remove all dead tissue is the most effective initial treatment. If no peroxide is available, povidone iodine or chlorhexidine 0.2% mouthwash should be used for local cleaning. In addition, give oral Metronidazole 400mg bd for 5 days.
F: Oro-pharyngeal Kaposi sarcoma mostly presents as painless red or purple macules, papules or nodules. Occasionally, lesions have the same colour as normal mucosa or are painful. Patients should be referred to level 2.
G: Patients with other oral manifestations should be referred for further investigation and treatment. PART 1-ADULTS 23 ORAL MANIFESTATRIONS OF HIV DISEASE - LEVEL 2 ADULTS
Table 5: Oral manifestations in HIV disease
Condition Clinical signs Aetiology Treatment Oral thrush White plaques on Candida Gentian violet 1% oral mucosa, or bleeding when Nystatin 500,000 IU removed tabl. qid Oral ulcers or Grouped blisters and Herpes simplex Analgesiscs blisters superficial on lips and oral mucosa Single ulcers with a Recurrent aphthous Analgesics yellow base and red ulcers Triamcinolone 0.1% inflamed border oral cream Painful ulcerative Acute necrotising Peroxide 3% or gingiva. Whitish ulcerative ginigivitis Chlorhexidin 0.2% pseudo-membranes and Metronidazole 400mg bd p.o. for 5 days Hairy White thickening of Epstein-Barr virus Explain benign leukoplakia the mucosa in a nature of the hairy pattern, mostly condition at the border of the Oral hygiene tongue. Parotid Swelling of parotid Unknown origin Investigate further if enlargement glands Infectious inflammation is Lymphoma, present or leukaemia enlargement is unilateral Xerostomia Dry mouth HIV infection of Oral hygiene parotid glands Stimulate saliva Side effect of medication Oral tumors Hard swelling, often Kaposi sarcoma Biopsy and referral dark in colour to oncology for Small, painless oral Lymphoma specific therapy masses Swelling of tongue or Squamous cell mucosa carcinoma
PART 1-ADULTS 24 ANNOTATIONS FOR ORAL MANIFESTATIONS - LEVEL 2 ADULTS
Oral thrush This is the most common HIV associated oral manifestation. It is an indicator of a decline in immunity and CD4 cells. Management of oral thrush is addressed separately (p 20- 24).
Ulcerative lesions Patients with severe or recurrent aphthous lesions will benefit from topical: Triamcinolone 0.1% oral cream bd. An alternative treatment is mouth rinses with a Betamethasone 0.5mg tablet dissolved in water. Ulcers with a diameter of more than 2 cm do not respond to this treatment and should be treated with Beclomethasone oral spray. In case secondary infection is suspected, local antifungal or systemic antibiotic treatment should be given.
ANUG Thorough local elimination of bacteria and affected tissue is essential for successful treatment of ANUG. Delay in treatment leads to a rapid spread of gingival infection to peridontal tissues and supporting bone. Peroxide 3% on a cotton tip is the most effective local treatment to eliminate necrotic tissue. If peroxide is unavailable, Povidone-iodine may be used. This treatment is followed by Chlorhexidine mouth rinses qid and Metronidazole 400mg p.o. bd for 5 days. Patients should be seen daily for follow-up to eliminate additional necrotic tissue. If symptoms persist patients should be referred to a dentist.
Parotid enlargement Parotid enlargement is sometimes observed in patients with HIV. If inflammation is present, an infection should be suspected and treated with Amoxycillin 500mg p.o. tds. Parotid enlargement may also be due to lymphoma or leukaemia, which may be confirmed by biopsy. Most frequently, parotid enlargement is due to unknown causes and does not need specific treatment. If Xerostomia is present, supportive treatment for this condition should be given.
Xerostomia Lack of saliva or dry mouth are common complaints in persons with HIV, even in absence of parotid enlargement. Some drugs, such as atropine may also reduce saliva production. Supportive treatment consist of stimulation of saliva. Stimulate the saliva with sugar free chewing gum or palm leaves in case of a dry mouth.
Kaposi sarcoma Biopsies should be taken from lesions that may possibly be and other lesions caused by Kaposi Sarcoma or any other lesion suspected to be due to malignancy (Lymphomas, oral carcinomas, etc.) PART 1-ADULTS 25 II.5 ORAL THRUSH – LEVEL 1 ADULTS
ORAL THRUSH (A)
Difficulty and/or YES pain in swallowing or retrosternal pain? (B)
NO
Presumed oral thrush Presumed oesophageal only Candidiasis
1. Oral hygience 2. Gentianviolet 1% solution tds for 14 days.
NO Nystatin tablets 500,000 IU Improved? qid for 14 days (C)
YES
YES Improved?
1. Follow up as needed NO 2. Consider maintenance treatment Refer to level 2 (E) (D)
PART 1-ADULTS 26 ANNOTATIONS FOR ORAL THRUSH – LEVEL 1 ADULTS
A: Definition: Presumptive: The presence of the characteristic white plaques on the oral mucosa. These plaques, usually located on the palate or buccal mucosa often bleed when they are removed. In some cases it may present only as red mucosal surface.
Confirmation:The demonstration of Candida spores or pseudohyphae in mouth scrapings
Aetiology: Candida infection
B: In HIV infected patients with oral thrush Candiasis may extend into the oesophagus. This will cause pain on swallowing, reluctance to take food, salivation and weight loss. Untreated oesophageal lesions, even if causing only mild dysphagia or discomfort may alter eating habits and add to poor nutrition.
C: Gentian violet and Nystatin tablets are very effective for oral candidiasis and may give sufficient relief for patients with candidiasis of the oesophagus. Nystatin is not absorbed and has only a local effect. To improve the contact between the drug and the infected areas, it is recommended to use dissolved tablets for gargling and swallowing after each meal and before bedtime. Treatment should be continued for at least 2 weeks to eliminate the spores.
D: Recurrence of oral thrush and oesophageal candidiasis is very common. Predisposing factors, such as the recent use of antibiotics could contribute to recurrence. In this case, prolonged treatment with Gentian violet or Nystatin may still be effective. Consider maintenance treatment with Gentian violet or Nystatin 500,000 IU twice daily if recurrences are too frequent or severe.
E: If response to Nystatin is insufficient, refer to level 2 for treatment with systemic antifungal treatment or further investigation.
PART 1-ADULTS 27 Referred ORAL THRUSHpatient LEVEL 2 ADULTS with oral thrush and malnutritio n or dysphagia
Do microscopic examination of mouth scraping (A)
YES Difficulty and/or YES Candida pain in swallowing spores or retrosternal demonstrate pain? (B) d NO
NO Presumed oesophageal Presumed oral candidiasis thrush only
NO 1. Oral hygiene 2. Nystatin 500.000 IU tabl. gargled qid for 14 days
Miconazole 250 mg po q.i.d. for 14 days YES NO or Improved? Ketoconazole 200 mg bd p.o. for 14 days (C)
YES Resolved?
NO 1. Follow up as needed 1. Continue treatment 2. Consider until resolved (D) maintenance 2. Consider maintenance Re-evaluation treatment (E) treatment (E) (F)
PART 1-ADULTS 28 ANNOTATIONS FOR ORAL THRUSH – LEVEL 2 ADULTS
A: The microscopic identification of pseudohyphae and/or blastospores of Candida albicans confirms the diagnosis of oral thrush.
B: Candidiasis may extend in to the oesophagus in HIV infected patients with oral thrush and causes pain on swallowing, reluctance to take food, salivation and weight loss. Other causes of oesophagitis are infections with Cytomagalovirus and Herpes simplex virus. Ulceration due to oral medication (such as Aspirin or NSAID) or acid reflux may also cause retrosternal pain. Rarely these symptoms are due to malignancy (Kaposi sarcoma, lymphoma, carcinoma) Untreated oesophageal lesions, even if causing only mild dysphagia or discomfort, may alter eating habits and add to poor nutrition of patients.
C: Miconazole is a local anti-fungal agent and Ketoconazole is a systemic oral anti-fungal agent. Miconazole is more effective than Nystatin, but less effective than Ketoconazole. Miconazole has less side effects and costs less than Ketoconazole. Use of Ketoconazole should be avoided in the presence of liver disease and in patients receiving treatment with Rifampicin.
D: Oesophageal lesions heal slowly, although symptomatic response is usually prompt. Prolonged treatment is often required.
E: Oro-pharyngeal and oesophageal candidiasis has a high likelihood of recurrence. Maintenance treatment (Nystatin 500,000 IU tablet gargled or Miconazole 3-4 times daily or Ketoconazole 200mg p.o. once per day or 3 times per week) may therefore be required.
F: Further investigations, such as endoscopy may be indicated after failure of adequate anti-fungal and anti-acid therapy, in order to diagnose and treat possible other conditions (such as Kaposi Sarcoma or severe Herpes simplex).
PART 1-ADULTS 29 II.6 RESPIRATORY CONDITION ADULTS
RESPIRATORY CONDITION (A)
History and physical Examination
Severe dyspnoea and/or a YES respiratory rate of more than 30 per minute (B)
NO
Give supportive Continue Level 1 treatment as available (C) Go to page 28 Refer to level 2
PART 1-ADULTS 30 ANNOTATIONS FOR RESPIRATORY CONDITION ADULTS
A: Definition:
Persistence or worsening of cough and chest pain and/or dyspnoea in a patient with symptomatic HIV infection.
Aetiology:
1. Pulmonary conditions:
Infections: Pyogenic bacteria Mycobacterium tuberculosis and atypical mycobacteria Pneumocystis carinii pneumonia Fungal infections (Candidiasis, Cryptococcus, histoplasmosis, coccidioidomycosis) Other: Cytomegalovirus infection Toxoplasmosis,
Malignancies: Kaposi sarcoma, Lymphoma
2. Other associated conditions:
Pleural effusion/empyema (associated with tuberculosis, bacterial infection or cancer).
Pneumothorax (associated with tuberculosis, Pneumocystis carinii pneumonia or cancer)
Pericardial effusion (often associated with tuberculosis)
B: Dyspnoea is defined as subjective shortness of breath at rest or on minimal exertion.
Respiratory distress is defined as objective evidence of respiratory dysfunction including tachypnoea (>30 per minute), hypoxaemia, tachycardia, and signs of ventilatory effort (intercostal indrawing, use of accessory muscles)
C: Oxygen therapy, where available, is indicated in the presence of dyspnoea and cyanosis. Supportive treatment, i.e. fluid replacement, temperature management, propping up of the patient and provision of enough fresh air should be done. In addition, symptomatic relief should be given, i.e. bronchodilators, if wheezing, etc. A first dose of a parenteral antibiotic should be given before referral, for example penicillin G. The patient should be transported in sitting position.
PART 1-ADULTS 31 RESPIRATORY CONDITION – LEVEL 1 ADULTS
Respirato ry condition Level 1 (Continu ed)
YES Cough with Co-trimoxazole 2 tabs fever bd for 5 days (A)
NO
NO YES Productive Improved? Cough?
YES NO Treat with Co- trimoxazole 2 tabs Amoxycillin 250-500 bd for 5 days mg p.o. tds for 5 days (B) AND Take sputum samples for AFB (D)
YES YES Improved? Improved?
NO NO
Take sputum smear for AFB Refer to level 2 AND for TB treatment Follow Refer to level 2 Supportive treatment or further up as for TB treatment (C) investigation needed or further Follow up as needed investigation (D)
PART 1-ADULTS 32 ANNOTATIONS FOR RESPIRATORY CONDITION – LEVEL1 ADULTS
A: In Namibia, Gram-positive pyogenic bacteria are the most likely cause of cough with fever. Response to Co-trimoxazole or Amoxycillin is likely to be prompt. Because malaria is a common cause of fever in endemic areas during the malaria season, anti-malarials should be added to the treatment if the temperature is > 39°C (see also “Fever in adults").
B: A second antibiotic course may be given if there is no response to Co- trimoxazole to eliminate all treatable pyogenic causes.
C: People with HIV diseases often have symptomatic respiratory conditions not due to a pyogenic infection. These may resolve without antibiotic treatment. Supportive treatment like analgesics, maintaining hydration and nutrition, should be given. Symptomatic relief with antihistamine drugs like Promethazine 10mg p.o. at night may be beneficial for patients with chronic unproductive cough.
D: The exclusion of tuberculosis is a high priority in patients not responding to antibiotics treatment. . Sputum smears should be carried out in all patients with cough > 2 weeks . High index of suspicion for patients who do not respond to a five day course of antibiotics . Refer if there is persistent fever of more than 2 weeks duration, night sweat, weight loss, or a presence of a swollen lymph node (>2cm in diameter) especially in the neck or the area above the clavicle.
PART 1-ADULTS 33 Referred patient RESPIRATORY CONDITIONSwith severe LEVEL 2 ADULTS dyspnoea or cough AND/OR not responding to adequate treatment at level 1 (A)
Oral or IV antibiotics Severe YES AND dyspnoea? Supportive therapy (B)(C)
NO
YES AFB Treat for positive TB ? (C)
NO
Treat with oral antibiotics (if not yet administered) AND/OR according to X-ray findings (B)(C)
YES Follow up as Improved? needed
NO
Consider presumptive treatment for TB (E)
YES Follow up as Improved? needed
NO
Consider presumptive treatment for fungal infection or re-evaluate (F)
PART 1-ADULTS 34 ANNOTATIONS FOR RESPIRATORY CONDITIONS – LEVEL 2 ADULTS
A: For all HIV positive patients, who are referred for severe dyspnoea or who did not respond to the prescribed treatment at level 1, an X-ray examination of the patient and sputum examination (for pyogenic bacteria and AFB) is done routinely. When laboratory facilities are available for analysis of blood gasses, blood is drawn in all patients with severe dyspnoea, when oxygen has been administered. Supportive treatment should always be started immediately. This includes fluid replacement, antipyretics, oxygen, etc.
If the temperature is > 39°C malaria should be excluded and haemocultures should be done.
B: Gram-positive pyogenic bacteria are the most probable cause of pneumonia. Response to oral Amoxycillin 250-500 mg qid for 5 days is likely to be prompt. In pneumonia with severe dyspnoea, IV treatment with Penicillin G 0.6 MIU qid plus IV Gentamycin 5 mg/kg once daily is indicated.
For suspected Staphylococcus lung infection based on X-ray images suggestive for abscess formation Cloxacillin 500mg iv or po qid is indicated. I In case Pneumocystis pneumonia is suspected on the basis of X-ray findings and presence of severe dyspnoea, Co-trimoxazole is given at a dosage of 15mg/kg/day Trimethoprim in 3 divided doses. A patient between 50-60kg will need for example a dosage of 20 ml or 4 tablets tds. Patients with PO2 <70mmHg should receive corticosteroids: prednisone 40mg po bd for 5 days, then 40mg daily for 5 days, then 20mg daily for 5 days 5. Treatment should be continued for 3 weeks and followed by maintenance treatment of 2 tablets of Co-trimoxazole once daily.
C: In case of TB, chest X-rays may be ‘classical’, but often the image is atypical such as in miliary tuberculosis. Treat TB according to National TB Guidelines. Patients with HIV have an increased risk for drug-induced hepatitis, exfoliative dermatitis, neuropathy on INH or other drug reactions. Routine supplement of pyridoxine should be given.
The effectiveness of TB treatment is similar for HIV positive and HIV negative patients. HIV infected persons have, however, a higher risk of dying from other infections.
Mortality and hospitalisations of persons with HIV and active TB can be reduced significantly by adding Co-trimoxazole prophylaxis (1 tabl. daily of trimethoprim 80mg/sulphamethoxazole 160 mg) to the usual TB treatment6.
PART 1-ADULTS 35 D: Pleural effusion should be aspirated for examination: TB is the principal cause of exudate in patients with HIV. Lymphocytes are expected to be found and AFB is usually negative. Pleural effusion will resolve on TB treatment. Persistent exudate is likely to be caused by malignancy, such as Kaposi Sarcoma.
E: A deteriorating clinical picture and worsening chest X-rays in spite of the prescribed treatment are sufficient for starting a trial of TB therapy.
F: All patients on presumptive TB treatment should be re-evaluated after 3 weeks. If there is no improvement, fungal infection or Kaposi sarcoma should be considered.
Pulmonary Kaposi sarcoma should be suspected in any patient with respiratory complaints and typical skin lesions or visceral lesions. Careful examination of the skin and oral cavity is the key to early diagnosis. For those suspected to have pulmonary Kaposi sarcoma referral for confirmation of diagnosis and cytotoxic therapy may be considered.
An empirical treatment for fungus using Ketoconazole 200mg bd for 3 weeks may be justified if no other cause is identified. The same treatment should be given if the respiratory symptoms get worse over time, even if the chest X-ray is not changing.
PART 1-ADULTS 36 II.7 OBSTETRICAL AND GYNAECOLOGICAL PROBLEMS
A: Common gynaecological problems include:
1. Vaginal discharge, due to Gonococcal infection Chlamydia trachomatis Trichomonas vaginalis Bacterial vaginosis Candidiasis
2. Lower abdominal pain and fever (PID), due to Gonococcal infection Chlamydia trachomatis Mixed bacterial infections (including anaerobes) TB
3. Genital sores (ulcers or blisters), due to Syphilis Chancroid Lymphegranuloma venereum (LGV) Herpes simplex (usually blisters, ulcers occur in severe immuno- deficient patients)
4. Genital warts Condylomata acuminata. This should be distinguished from: Condylomata lata (due to secondary syphilis)
5. Malignancies Cervix CA Kaposi sarcoma
6. Amenorrhoea
For management of vaginal discharge, lower abdominal pain, and genital ulcers, follow national STD management guidelines. Ensure treatment of partner(s). Response to treatment of bacterial STDs is usually excellent. Early, appropriate treatment of STDs in male and female patients and their partners is an important strategy to reduce HIV transmission.
In case of lower abdominal pain, exclude acute conditions (such as appendicitis, ectopic pregnancy, etc.). If the patient does not respond to the usual treatment for PID, patients should be referred for a pregnancy test on blood (to exclude ectopic pregnancy with a negative urine pregnancy test) and to exclude pelvic abscess or TB.
PART 1-ADULTS 37 Vaginal candidiasis is common in women with HIV. In most cases, response to treatment with vaginal antifungal therapy (Clotrimazole pessary 500 mg) is good. Recurrence of infection after appropriate treatment may occur. These recurrent infections usually also respond well to treatment. If recurrence is very frequent, regular intermittent treatment may be considered. Candidiasis also frequently occurs during systemic antibiotic treatment. Candidiasis on other body parts, such as skin folds will usually respond well to topical gentian violet. Systemic treatment with Ketoconazole 200mg po daily for 5 days may rarely be indicated in severe cases.
In patients with HIV, genital Herpes infection is common. It tends to be more severe and may spread to other parts of the body (buttocks, abdomen). Give supportive treatment (pain relief and gentian violet). Antibiotics (Co-trimoxazole 2 tabl. bd or Cloxacillin 250 mg qid for 5 days) are indicated in case of secondary infection. Oral Acyclovir 200 mg qid for 5 days reduces the pain and promotes healing when started early and may be indicated for very severe cases.
Genital warts tend to be more common and severe in persons with HIV. Treatment consists of topical application of Podophyllin 20% twice a week by a health worker or removal by means of surgery or electro-cauterisation.
Menstrual disturbances are frequent in women with HIV. These may be linked to general deterioration and weight loss due to HIV disease. However, other causes of menstrual disorders need to be excluded, such as cervicitis, PID and TB.
A missed menses or irregular bleeding in a sexually active women who is not consistently using a very effective method of contraception is an indication for pregnancy testing.
Fertility declines when HIV disease progresses. However, even in advanced HIV disease, pregnancy occurs. All HIV positive women should therefore be counselled on the following issues: HIV can be transmitted from the infected mother to her child during pregnancy and delivery as well as by breastfeeding. About one third of the children born will become infected (see also part 2). Pregnancy does not have an influence on the progression of HIV disease. A woman with HIV has the right to terminate the pregnancy as a medical indication. This decision should, however, be taken early in pregnancy and usually a tubal legation (sterilisation) is done to prevent subsequent pregnancies.
In choosing a contraceptive, the woman (and her sexual partner) should be assisted the effect on HIV transmission and the wish to have following issues should be considered: effect on HIV transmission, pregnancy failure rate, acceptability of the method. A combination of a barrier method (condom) and highly reliable method (pill, injection, sterilisation) may be considered, in particular in discordant couples or partners with unknown sero-status.
PART 1-ADULTS 38 Table 6: Contraceptive methods and pregnancy failure rate* Method Pregnancy failure Effect on HIV Comments rate transmission Typical Perfect use use Tubal sterilisation 0.5% 0.5% No effect Permanent Vasectomy (male 0.5% 0.5% No effect Permanent sterilisation) Injection (Depo- <0.5% <0.5% No effect Injection every 3 Provera) months Norplant <0.5% <0.5% No effect Subdermal implant. Lasts 5 years. Rate of irregular bleeding in first year 60% Oral contraceptive 5% <1% No effect Requires daily pill IUCD 0.8% 0.6% No effect Duration 3-5 years Male condom 14% 3% Reduced more Major concern is than 10-fold proper consistent use Female condom 21% 5% Reduced more Woman needs clear (Femidom) than 10-fold instruction on utilisation and support of partner. Consistent use. More expensive than male condom. Rhythm 25% 9% No effect Not recommended for birth control in persons with HIV Withdrawal 19% 4% No effect Not recommended for birth control in persons with HIV *percent who accidentally became pregnant in first year of use
Pregnancy and HIV Pregnant women with CD4 counts <200/mm3 may be at increased risk for pre- term delivery and low birth weight infants. Complications due to HIV disease may occur during pregnancy. Prophylaxis should therefore be continued where indicated (see page ) The usual scheme for follow-up is applicable for HIV positive pregnant women. Emphasise safer sexual practices throughout pregnancy to avoid STD and HIV re-infection Discuss postpartum contraception Avoid procedures such as foetal scalp monitoring and scalp blood sampling Use universal precautions, including eye protection during delivery. Avoid artificial rupture of membranes. Caesarean section should be performed for standard obstetric indications. Avoid episiotomy if possible.
PART 1-ADULTS 39 II.8 FEVER - LEVEL 1 ADULTS
FEVER (A)
History and physical examination
Consider antipyretic management Maintain hydration Test and treat for malaria (B)
YES Improved?
NO
Co-trimoxazole 2 tabl. bd for 5 days (C)
YES Improved?
NO
Refer to Level 2 Follow up as (D) needed
PART 1-ADULTS 40 ANNOTATIONS FOR FEVER - LEVEL 1 ADULTS
A: Definition: Recurrent or persistent fever (temperature > 37.5 °C) with a duration of more than 2 weeks as the ONLY clinical presentation in a patient with HIV infection.
Aetiology: 1. Infections: 1 Protozoal: Malaria
2 Bacterial: Pyogenic infections of the chest, of the CNS or the urinary tract, etc Bacteraemia due to Borreliosis, Salmonella, Streptococcus pneumoniae, Haemophilus influenzae, etc
3 Mycobacterial: Mycobacterium tuberculosis Atypical mycobacteria
4 Viral: Upper respiratory tract infections, e.g. common cold Cytomegalovirus, Epstein-Barr virus HIV infection itself
2. Malignancies (for example Lymphomas)
B: In endemic areas, a febrile patient should be tested for malaria and antimalarial treatment should be given prior to further diagnostic investigation, especially during peak malarial season.
C: Use a broad spectrum antibiotic e.g. Co-trimoxazole 2 tablets bd for 5 days, as an initial therapy for bacteraemia, ENT infections and urinary tract infections.
D: Referral is particularly helpful in identifying other treatable causes of persistent fever, such as tuberculosis.
PART 1-ADULTS 41 FEVER LEVEL 2 Referr ADULTS ed patien t with fever
1. Blood slides for malaria and Borreliosis 2. Examination of urine for deposit of WBC and RBCs 3. Full haemogramme 4. Blood culture (A) 5. Microscopy of sputum (if present) for AFB Treat for malaria or Borrelia according to findings (B)
YES Any findings
NO 1. Chest X-ray 2. CSF microscopy: Treat any infection as Gram stain, cells, etc. indicated (C) acid fast stain, Indian ink culture 3. Repeat blood slide for malaria and Borreliosis 4. Full haemogramme 5. Blood culture (including anaerobes and mycobacteriae) 6. Other investigations (ultrasound?) (D)
YES Other causes Treat as indicated identified
NO
Re-evaluate (E)
PART 1-ADULTS 42 ANNOTATIONS FOR FEVER – LEVEL 2 ADULTS
A: In cases of persistent fever, despite adequate antimalarial treatment, a blood slide for Malaria parasites should always be done. Depending on local prevalence, blood should also be examined for other infections, in particular for Borreliosis. For very sick patients blood for culture should be taken and treatment with intravenous antibiotics should be started immediately (for example Ampicillin 250-500 mg qid plus Gentamycin 5mg/kg once daily plus Metronidazole 500 mg tds). If the patient can produce sputum, Ziehl-Neelsen stain for AFB should be done. In all patients with persistent fever not responding to antibiotics, mycobacterial infection should be suspected. Diagnosis may be confirmed by haemocultures, using specific growth media.
B: Treatment for malaria should be done according to national malaria treatment guidelines. In those patients suspected of complicated malaria, intravenous Quinine should be started immediately.
C: Treatment for bacterial infection should be according to the site of infection (for example respiratory, urinary) or identified micro-organisms.
D: Specialised investigation where available, such as ultra-sound, may be useful to identify other possible causes of fever such as intra-abdominal abscesses or tumour.
E: The possibility of viral infection should be considered, whereby symptomatic treatment is given, including antipyretics, maintenance of hydration and nutrition. If no other causes have been determined and fever continues, a trial with TB treatment may be justified.
PART 1-ADULTS 43 II.9 HIV ASSOCIATED SKIN DISEASE ADULTS AND CHILDREN
HIV-ASSOCIATED SKIN DISEASE (A)
Warm, inflamed, YES Bacterial Go to painful and/or infection page 44 fluctuating?
NO
Discoloured YES Fungal infection Go to skin-patches? or Kaposi page 46 sarcoma
Kaposi sarcoma
Localised Go to eruptions or YES Viral infection Page 48 Localized pimple- like swellings
NO
Prurigo and/or other skin conditions
Go to Page 50
PART 1-ADULTS 44 ANNOTATIONS FOR HIV-ASSOCIATED SKIN DISEASES ADULTS AND CHILDREN
A: The management of skin diseases associated with HIV infections does not differ greatly between adults and children except where systemic therapy is required, in which case the dosage for children should be adjusted according to body weight.
Definition: The presence of a skin disease (dermatosis) in a patient with symptomatic HIV infection.
Aetiology: 1. Viral infections Herpes zoster Herpes simplex Molluscum contagiosum Condylomata acuminata
2. Bacterial infections Furunculosis Impetigo and pyoderma (staphylococci, streptococci) Hidradenitis suppurativa Pyomyositis (often with discharging sinuses Condylomata lata
3. Fungal infections Candidiasis Dermatophytosis
4. Malignancies Kaposi sarcoma
5. Other dermatoses Drug eruptions: erythema multiforme and its severe form, Stevens-Johnson syndrome Chronic prurigo or urticaria (blood parasites or other common aetiologies excluded) Severe seborrhoeic dermatoses Generalised erythroderma Severe psoriasis Scabies
Itching and dry skin, in absence of any other treatable cause are very common in persons with HIV. This problem can severely affect the wellbeing of the patient and deserves the necessary attention and treatment.
PART 1-ADULTS 45 HIV-ASSOCIATEDConti SKIN DISEASES – BACTERIAL INFECTIONS nued from Page 42
1. Surgical Fluctuant YES Skin abscess drainage And tender or 2. Antibiotics for pyomyositis 5 days (B)
Furunculosis 1. Local lesion Skin-sepsis YES or care around hair Folliculitis 2. Antibiotics for follicles 5 days (B)
NO
1. Local lesion Recurrent care and/or multiple sores YES Hydradenitis surgical and boils in suppurativa drainage the armpit or 2. Antibiotics for other wet 5 days (B) areas?
NO
1. Local lesion YES care Multiple Impetigo superficial 2. Antibiotics for skin sores 5 days (C)
NO
1. Re-evaluation 2. Symptomatic relief (D)
PART 1-ADULTS 46 ANNOTATIONS FOR HIV-ASSOCIATED SKIN DISEASES BACTERIAL INFECTION
A: Although surgical drainage is all that is usually required in abscesses or pyomyositis, immuno-suppressed patients are given antibiotics to prevent the possible development of Bacteraemia or septicaemia during the procedure and also to speed up recovery.
B: In the absence of facilities for determining antibiotics sensitivity of the micro-organisms responsible for abscesses, Cloxacillin or Erythromycin 250-500mg capsules qid for 5 days is the treatment of choice. In many cases Amoxycillin 250-500 mg qid is also effective. This drug should therefore be given if none of the above-mentioned drugs are available.
C: Impetigo is a common condition in children. Treatment consists of local lesion care with skin antiseptics. In severe cases antibiotics are indicated. In these situations Cloxacillin or Erythromycin 50 mg/kg/day qid for 5 days should be given.
D: Symptomatic relief for itching may include: Avoid exposure to dry wind. Soothing lotions like calamine or Vaseline. Use of bath oil. Dry skin after bath by patting with a soft towel. Oil skin after bathing with cream, body oil or lanolin. A cucumber cut and rubbed over the itchy areas is a good home remedy for dry itchy skin. Local corticoids may be useful if inflammation is present in absence of any (bacterial, fungal or viral) infection. Antihistamines, like oral Promethazine 10 mg at night, may be useful. Hydroxyzine 25mg at bedtime may be useful for severe itching.
PART 1-ADULTS 47 HIV – ASSOCIATED SKIN DISEASES FUNGAL INFECTIONS OR KAPOSI SARCOMA Conti nued from page 42
Dark patches, painless swelling or Kaposi Refer if nodules that are not YES sarcoma necessary itchy and no ring after biopsy pattern, with or (A) without similar oral lesions?
Hyper– or hypo- YES pigmented patches, Tinea Treat with which are itchy, with (dermatophytosis) anti-fungal or without a ring cream (B) pattern and with scaling
1. Local application of 1% aqueous solution of gentian violet Itchy, wet lesions, YES Skin prominent in IF NO RESPONSE Candidiasis armpits, groins and under breast? 2. Clotrimazole cream twice daily until lesions are cleared (C)
NO
1. Re-evaluate 2. Symptomatic relief (D)
PART 1-ADULTS 48 ANNOTATIONS FOR HIV–ASSOCIATED FUNGAL INFECTIONS AND KAPOSI SARCOMA
A: Cytotoxic treatment for Kaposi sarcoma (KS) is in itself immuno- suppressive. Before considering referral of a patient with KS, the benefits and the disadvantages should be weighed and if necessary, discussed with the patient and the caring family. When a decision of referral is reached, a biopsy should be taken for referral to the oncology department. If the condition of the patient requires immediate referral, the biopsy number (obtained form the Department of Pathology) should be sent with the patient.
B: Topical anti-fungal treatment includes Clotrimazole cream 1% daily for up to 3 weeks. Patients should explained that local treatment may take a long time. Widespread dermatophytosis may necessitate systemic treatment with Griseofulvin 500 mg once daily or Ketoconazole 200mg daily for 3 weeks for skin lesions and up to 6 months for lesions of the nails.
C: If there is no response to therapy, Ketoconazole 200 mg tables bd for 10 days may be required.
D: Symptomatic relief for itching may include the following: Avoid exposure to dry wind. Soothing lotions like calamine or Vaseline. Use of bath oil. Dry skin after bath by patting with a soft towel. Oil skin after bathing with cream, body oil or lanolin. A cucumber cut and rubbed over the itchy areas is a good home remedy for dry itchy skin. Local corticoids may be useful if inflammation is present in absence of any (bacterial, fungal or viral) infection. Antihistamines, like oral Promethazine 10 mg at night, may be useful. Hydroxyzine 25mg at bed time may be useful for severe itching.
PART 1-ADULTS 49 HIV ASSOCIATED SKIN DISEASES VIRAL INFECTIONS Conti nued from Page 42 Local YES On the YES Herpes lesions Painful? mouth or or simplex care ano-genital (A) area?
Local lesions Well YES Herpes care demarcated zoster Pain relief NO along a (B) dermatome
NO
1. Re-evaluate 2. Symptomatic relief (C)
No YES Small papula Molluscum treatment with a contagiosum required central (D) dimple
NO
Finger-like Treatment by with projections on YES Condylomata Podophyllin 20 % surface with acuminata twice weekly cauliflower (genital warts) (E) appearance?
NO
1. Re-evaluation 2. Symptomatic relief (F)
PART 1-ADULTS 50 ANNOTATIONS FOR HIV-ASSOCIATED SKIN DISEASES VIRAL INFECTIONS
A: Herpes simplex in HIV disease runs a chronic ulcerative course. Local lesion care should include cleaning the ulcerated vesicles with salt water and keeping them dry. Gentian violet may be applicated on the lesions. For very severe cases, Acyclovir 400 mg tds for 5 days may give great relief if administered within the first 24 hours.
B: Herpes zoster lesions may be self limiting and may not need more than pain relief (Aspirin or Paracetamol 500 mg qid) and local lesion care (with gentian violet or antiseptics). Local application of Lignocaine gel 2% may help to improve pain relief in some patients. Stronger analgesics are sometimes needed such as Paracetamol 1g plus Codeine 60mg every 4 hours. Acyclovir (800 mg qid for 7 days) is indicated in patients with ophthalmic lesions. Treatment should start within 1-2 days of onset of symptoms.
Post-herpetic neuralgia, if present, should be treated with pain modifying agents. Phenytoin 100 mg slowly increasing to 250 – 300 mg daily or Carbamazepine 100 mg daily increasing to 400 mg daily in 10 days.
C: Symptomatic relief includes analgesics and local care.
D: These lesions are usually painless and do not necessitate treatment.
E: Podophyllin 20% can be corrosive to the surrounding unaffected skin. It should only be applied to the tips of the warts and washed away not later than 6 hours after application. For warts on the genital mucosa and mouth a lower concentration of Podophyllin (10%) may be applied. Alternative treatments include electro-cauterisation and surgical removal.
PART 1-ADULTS 51 HIV ASSOCIATED SKIN DISEASES OTHER SKIN CONDITIONS Conti nued from page 42
1. Withdraw drug Generalized skin 2. Local lesion eruption and/or YES Drug care inflamed mucous eruption 3. Oral anti- membranes histamines (A)
NO
Topical calamine Itchy generalzed YES lotion maculo-papular skin HIV associated skin rash Or rash Antihistamines Erythroderma (B)
NO 1. Topical steroids (1% hydro- YES Generalized greasy Seborrhoeic cortisone) scaling with dermatitis 2. Coal tar excessive dandruff 3. Soothing cream on the scalp, face (C) and chest
NO
1. Re-evaluate 2. Give symptomatic treatment (D)
PART 1-ADULTS 52 ANNOTATIONS OTHER SKIN CONDITIONS
A: Co-trimoxazole and anti-TB drugs are often associated with drug eruptions. Systemic corticosteroids are immune depressing and should only be given in life-threatening situations.
B: A generalised pruritic maculo-papular skin rash due to eosinophilic folliculitis is a typical of HIV. No specific opportunistic infection has identified to cause it. Treatment is mainly symptomatic. Antihistamines e.g. tabs Chlorpheniramine 4 mg 8 hourly or Promethazine 10mg bd. Ultraviolet light and topical application of steroids and calamine lotion over the involved areas are useful.
C: Seborrhoeic dermatitis usually responds well to topical steroids, coal tar and soothing cream. Recurrence is frequent, maintenance therapy may therefore be necessary. If response to therapy is poor, suspect secondary infection, which requires local antiseptics (such as povidone iodine or chlorhexidine) and may need systemic antibiotics (Cloxacillin or Ampicillin 250-500mg tds). Seborrhoeic dermatitis may also be complicated by cutaneous fungal infection. In this case combine topical steroids with Clotrimazole cream 1%. In severe cases, oral Ketoconazole 200mg daily may be indicated.
D: Not all HIV associated skin diseases can be easily fitted in this algorithm. Many times a decision has to be made to give only symptomatic relief. In general the following approach can be useful: Avoid exposure to dry wind. Dry scaly lesions need a soothing lotion, such as Calamine lotion, Emulsifying ointment or Vaseline. Use of bath oil. Dry skin after bath by patting with a soft towel. Oil skin after bathing with cream, body oil or lanolin. A cucumber cut and rubbed over the itchy areas is a good home remedy for dry itchy skin. Local corticoids (hydrocortisone cream 1%) may be useful if inflammation is present in absence of any (bacterial, fungal or viral) infection. Oral antihistamines, such as Chlorpheniramine 4 mg tabs 8 hourly and/or Promethazine 10 mg at bedtime, may be useful. Hydroxyzine 25mg at bed time may be useful for severe itching.
PART 1-ADULTS 53 II.10 LYMPHADENOPATHY – LEVEL 1 ADULTS
LYMPHADENOPATHY (A)
Any local or regional YES Treat as indicated infection which might (such as skin explain infections, genital lymphadenopathy? ulcers, etc.)
NO
1. Carry out RPR test or treat for presumptive Non-itchy skin Syphilis (Benzathine rash and/or YES Penicillin 2.4 million evidence of IU im weekly for 3 recent genital weeks) (B) ulcer? 2. Follow up
NO
Any of the following present? fever YES Presumptive weight loss TB (C) unilateral nodes increase in size matted nodes fluctuant nodes Minimal tenderness
NO Refer to level 2 for further Persistent Generalised investigation Lymphadenopathy and treatment (D) (D)
PART 1-ADULTS 54 ANNOTATIONS FOR LYMPHADENOPATHY - LEVEL 1 ADULTS
A: Definitions: Lymphadenopathy may be localised or generalised. It is important to identify the possible underlying causes of localised lymphadenopathy, in order to give appropriate treatment. Usually, local lymphadenopathy, affecting only 1 or 2 regions is caused by a local infection. Sometimes it may be due to TB or a malignancy such as lymphoma.
Persistent Generalised Lymphadenopathy (PGL) is defined as follows: 1. More than 3 separate lymph node groups affected 2. At least 2 nodes more than 1.5 cm in diameter at each site 3. Duration of more than 1 month 4. No local infection that might explain the lymphadenopathy
Aetiology:
1. Infections Bacterial infection: Staphylo- or Streptococcal (in particular in association with dermatological conditions) Mycobacterial (TB or atypical mycobacteria) Syphilis Fungal (histoplasmosis) Viral (Cytomegalovirus, infectious mononucleosis)
2. Malignancies Kaposi sarcoma (not necessarily associated with cutaneous KS) Lymphoma
3. HIV infections itself
B: In presence of genital ulcer, manage according to STD guidelines (Benzathine Penicillin im 2.4 MIU stat plus Ceftriaxone 250mg im stat). Secondary syphilis may be diagnosed on the basis of skin rash and Condylomata lata, etc. When possible, the diagnosis should be confirmed with a syphilis test (RPR). Treat patients and their partners with Benzathine Penicillin im 2.4 MIU once weekly for 3 weeks. Alternative treatments for syphilis are: Doxycycline 100 mg bd for 2 weeks if a patient is allergic to penicillin. Erythromycin 500 mg qid for 2 weeks in case of pregnancy
C: Extrapulmonary TB is common in HIV infected patients. In this case, peripheral lymph nodes are frequently involved and show one or more of the features listed in the algorithm.
D: PGL in HIV-infected patients is mostly due to the normal immune reaction to HIV infection. If no other problems are identified, no additional investigation or treatment is required. Lymph nodes usually disappear as the immuno- suppression advances and opportunistic infections appear.
PART 1-ADULTS 55 LYMPHADENOPATHYReferred – LEVEL 2 ADULTS patient with lymphad enopathy (A)
Any of the following present? Chest X-ray and/or fever YES lymph-node biopsy weight loss for AFB stain and unilateral nodes histology matted nodes fluctuant nodes minimal tenderness
YES Any treatable Treat as findings indicated established? (B) NO
Lymphadenopathy of uncertain origin
Follow up as needed
PART 1-ADULTS 56 ANNOTATIONS FOR LYMPHADENOPATHY – LEVEL 2 ADULTS
A: In case no syphilis test or treatment was given at level 1, perform the RPR test at level 2 to exclude possible syphilis. Treat RPR positive patients and their partners with Benzathine penicillin 2.4 MIU im weekly for 3 weeks.
B: Persistent generalised lymphadenopathy is common in HIV-infected patients. The presence of enlarged painless lymph nodes is usually due to the immune reaction to HIV and disappears when the disease progresses.
The presence of the following signs suggest that there may be another underlying cause: Marked asymmetry or a unilateral enlarged lymph node. Rapidly enlarging lymph nodes. The presence of general symptoms (such as weight loss and fever)
Biopsy is the most reliable method to establish the diagnosis, such as: TB, Lymphoma, lymphadenopathic Kaposi sarcoma and infiltrative fungal infection.
If no underlying problem is identified, no additional investigation or treatment is required.
PART 1-ADULTS 57 II.11 PAIN IN HIV DISEASE ADULTS
A: Definition:
Persistent or recurrent pain, localised in a part of in parts of the body, lasting more than 48 hours and not disappearing on simple comfort measures in a patient with symptomatic HIV infection. It can be just flashes of pain, burning or tingling.
For most patients, physical pain is only one of several symptoms. Relief of pain should therefore be seen as part of a comprehensive pattern of care. Physical aspects of pain cannot be treated in isolation from other aspects, nor can patients’ anxieties be effectively addressed when patients are suffering physically. The various components must be addressed simultaneously.
The first principle of managing pain in HIV disease is an adequate and full assessment of the cause of the pain, bearing in mind that most patients have more than one pain and different pains have different causes. While the cause of pain is often susceptible to specific treatment, symptomatic treatment should not be delayed.
Types of pain:
1. Headache: Cryptococcal meningitis TB meningitis viral meningitis (HIV, CMV) Malaria muscle tension headache neurosyphilis side effect of some medications Toxoplasmosis dehydration lymphoma of the brain Herpes zoster
2. Peripheral neuropathy: HIV Cytomegalovirus Due to medication Diabetes Avitaminosis post-herpetic neuralgia
PART 1-ADULTS 58 3. Abdominal pain: peptic ulceration gastro-enteritis retroperitoneal adenopathy abdominal tumours (lymphomas and Kaposi sarcoma) pelvic inflammatory disease abdominal abscesses worm infestations acute abdomen
4. Oro-pharyngeal and oesophageal pain: Reflux oesophagitis Candidiasis Herpes simplex Kaposi sarcoma Tonsillitis/pharyngitis Aphthous ulcers
5. Skin pain: Herpes zoster: either acute initial pain or post-herpetic neuralgia skin sepsis
6. Chest pain: lung infections mediastinal lesions (e.g. retrosternal adenopathy, Kaposi sarcoma) oesophageal candidiasis
7. Generalised pain: Fever bed ridden status rheumatism non-specific aetiology
PART 1-ADULTS 59 PAIN IN HIV DISEASE – LEVEL 1 ADULTS
1. Treat for PAIN IN HIV HEADACHE malaria (B) DISEASE Fever? 2. Refer to Neurologicalsi level 2 gns? (A)
Any findings For management YES CHESTPAIN suggestive see chapter on Cough? of a “Respiratory Dyspnoea? treatable Condition” cause of pain
Pharyngeal OR For retrosternal management pain? see chapter Any oral or on “oral pharyngeal thrush” thrush? NO (C)
Treat with anti-acids 2 ABOMINAL tabs tid PAIN Dyspepsia/PU See chapter symptoms? on Diarrhoea? (D) Diarrhoea
Give local SKIN PAIN lesion care Ulceration? and see Local sepsis? chapter on Herpes Skin diseases zoster/scars? Give symptomatic treatment, for example Paracetamol or Aspirin as required. (E)
YES Pain resolved? NO Follow up as Refer to level 2 (F) needed
PART 1-ADULTS 60 ANNOTATIONS FOR PAIN IN HIV DISEASE – LEVEL 1 ADULTS
A: These include: 1. Change in mental state (may be subtle) including loss of concentration, personality change (mild to psychotic), confusion, dementia 2. Weakness of limbs, movement disorders, drunken gait, inability to speak 3. Seizures 4. Evidence of neck stiffness, vomiting, confusion, high blood pressure and slow pulse in presence of fever
Wherever possible, further evaluation of headache, particularly in a patient with symptomatic HIV infection showing neurological signs, should be pursued to identify treatable conditions.
B: Cerebral malaria may lead to mental changes and in endemic areas malaria treatment should be started if fever is present. Immediate referral is needed if there is no improvement, while care is taken to maintain hydration.
C: Oesophageal thrush may represent as pain or difficulty in swallowing. There may be no obvious signs of associated oral thrush. Often an examination of the mouth and throat may reveal pharyngeal thrush.
D: Hyperacidity and oesophageal reflux may often present as pain in the lower chest and in the upper abdomen. This pain will usually respond to therapy with anti-acids.
E: As in patients without HIV infection: commence with simple analgesic such as acetylsalicylic acid or Paracetamol and increase to analgesics containing narcotics of varying strength as needed. In palliative treatment, optimal pain relief is essential.
F: Many treatable conditions may present with localised pain alone. Referral for further evaluation may be indicated. If causal treatment is not possible, adequate palliative treatment of pain should be established at level 2. Thereafter, patients should be referred back with clear instructions on pain medication to level 1 for further maintenance therapy and follow-up.
PART 1-ADULTS 61 PAIN IN HIVReferred DISEASE – LEVEL 2 ADULTS patient with persistent pain
1. Neurological evaluation (A) 2. Blood smear for malaria and other parasites, if fever YES 3. CSF examination for: Headach Cells, protein, glucosis e? Gram, Indian ink, AFB stain RPR (B) NO
Any positive Other localised Treat laboratory YES persistent pain accordingly findings (C)
NO
Treat for Evaluate Any focal YES toxoplasmosis signs? (D)
NO
Any other Treat cause accordingly identified?
NO
Headache or other NO pain of uncertain Improve origin d?
YES
Follow up SYMPTOMATIC TREATMENT (E) as 1. Paracetamol 1 g every 4 hours. needed IF NO RESPONSE, ADD 2. Codeine 30-60 mg qid for 5 days IF NO RESPONSE, CHANGE TO 3. Morphine 20 mg po or im every 4 hours 4. Give specific analgesics for neurologic pain
PART 1-ADULTS 62 ANNOTATIONS FOR PAIN IN HIV DISEASE – LEVEL 2 ADULTS
A: These include: Change in mental state (may be subtle) including loss of concentration, personality change (mild to psychotic), confusion, cognitive impairment, dementia Focal neurological deficits including paresis, cranial nerve palsies, movement disorders, ataxia, aphasia Seizures Evidence of meningeal irritation or raised intracranial pressure (neck stiffness, high blood pressure and slow pulse in the presence of fever)
B: Examination of cerebrospinal fluids (CSF) is essential for establishing the diagnosis of major causes of treatable headache, for example bacterial meningitis, tuberculosis and Cryptococcal meningitis. Suspect TB meningitis if proteins are present in CSF, even if AFB stain is negative. CSF disturbances are often mild in case of cryptococcal meningitis. Indian ink stain has a sensitivity of about 85%. CSF cryptococcal antigen test has a higher sensitivity (about 92%)7. If the RPR test on CSF is positive, treat with IV Penicillin or Procaine Penicillin for 10 days. Benzathine Penicillin is ineffective as it does not reach the CSF.
C: Early diagnosis of Cryptococcal meningitis is important to improve prognosis and reduce duration and cost of hospitalisation. Treatment of Cryptococcal meningitis for patients with a normal mental status consists of oral Fluconazole 400 mg once daily for 6 weeks. All other patients should initially receive IV Amphotericin B, in dose ranging from 0.7 mg/kg daily by intravenous infusion over 4-6 hours for 10 days. It is advised to start with a low dose and increase, as tolerated. After initial treatment, life-long maintenance treatment is necessary with Fluconazole 200 mg daily po or Amphotericin B 0.7-1mg/kg IV once per week, as relapses are common.
D: Toxoplasmosis is the most probable cause of focal signs in patients with HIV. It usually responds promptly and well to treatment and this response can be used to support the diagnosis. Treatment consists of: 3 tablets of Sulphadoxine 500 mg plus Pyrimethamine 25 mg (Fansidar) on days 1 and 4 followed by Co-trimoxazole 2 tablets bd form day 8 to 28. If there is no response to this therapy within 2 weeks, a diagnosis of cerebral Toxoplasmosis is unlikely. If the response is good, the course of 4 weeks should be completed. OR A combination of Pyrimethamine, 50-100 mg orally every 4 days and Sulfadiazine, 8 gr. per day for 6 weeks. Maintenance therapy of Co-trimoxazole 2 tablets twice daily should be given after successful initial treatment, because the risk of recurrence is high.
E: Sufficient medication should be given to ensure adequate pain relief in patients with HIV disease. The choice of analgesic depends on the severity of the pain, not on the stage of the disease. Drugs should be administered at regular intervals in a stepwise fashion (see page 64). PART 1-ADULTS 63 Table 7: CNS Conditions Co C C Other Diagnostic Tests nd l S Cr F N Crypt antigen ypt e o CSF: nearly 100% oc v r Serum: 95% oc e m Definitive dx: CSF antigen cal r a and/or positive culture Tome F, Nl Toxoplasmosis serology (lgG) xo e o false neg. in 5-10% pla v r Response to empiric therapy: sm e m >85% respond by day 7. osi r a CT Scan/MRI s , l Tu Fr N: Chest x-ray - active TB in 50% ber e o PPD positive: 20-30% cul v r Definitive dx: positive culture osi e m CSF s Ar Pa Serum VDRL and FTA-ABS s r are clue in >90%; false neg y o serum VDRL in 5-10% with Ne m t tabes dorsalis or general uro p e paresis sy t i Definitive diagnosis: positive phi o n CSF VDRL (found in 60-70%) lis m : Note: Most common forms in a HIV-infected persons are t 4 ocular, meningeal, and i 5 meningovascular. HI Ac N- Neuropsychological tests show V- f o subcortical dementia as e r Minimental exam is insensitive so b m - use timed tests, eg, HIV cia r a Dementia Scale (JAIDS ted i l 1995;8:273) Pde Al N: Definitive dx: stereotactic ML f o biopsy - antibody stain to e r SV40. Characteristic inclusions (Pr b m in oligodendrocytes; bizarre ogr r a astrocytes Pries Ai Nl Suspect with neg. toxo. IgG or ma f o failure to respond to empiric ry e r toxo. treatment (MRI and CN b m clinical evaluation at 2 wks) S r a Additional diagnostics: EBV Ly i l DNA in CSF Cmp Fl C: Definitive dx: brain biopsy with M e S hisTOPath and/or positive V v F culture (cy e Hyponatremia (reflects CMV to r m adrenalitis) me ± a Retinal exam for CMV retinitis
PART 1-ADULTS 64 Table 8: Differential Diagnosis of Lower Extremity Symptoms in HIV Infection Syndrome Symptoms Clinical Features Treatment Pain and numbness in Reduced pinprick/vibratory Symptomatic treatment: toes and feet; ankles, sensation. Avoid tight footware, walk short Poly sensory calves, and fingers Reduced or absent ankle jerks distances, soak feet in ice. neuropathy involved in more Contact allodynia Analgesics where indicated (PSN) advanced cases CD4 (hypersensitivity) present in some (paracetamol, ibuprofen, <200 but can occur at cases. Amitriptyline) higher CD4 level Discontinuation of presumed Same as PSN (above) but neurotoxic medication. Toxic symptoms occur after Same as PSN (above). Symptoms may worsen for a few neuropathy initiation of ddI, ddC, d4T. weeks ("coasting") before improving. Any CD4 count. Symptomatic treatment. Reduced sensation over soles of Pain and numbness Infiltration of local anesthetic in tarsal Tarsal tunnel feet predominantly in anterior tunnel may provide symptomatic syndrome Positive Tinel's sign at tarsal portion of soles of feet. relief. tunnel. Pain and aching in Mild/moderate muscle Creatine phosphokinase (CPK) muscles, usually in thighs tenderness. HIV- usually elevated. and shoulders. Weakness Weakness predominantly in associated If patient is on AZT, discontinue AZT with difficulty arising from proximal muscles (ie, deltoids, myopathy/AZT and follow every two weeks. a chair or reaching above hip flexors). myopathy Symptoms/signs/CPK should shoulders. Normal sensory exam/normal improve within one month. Any CD4 count. reflexes. Rapidly evolving weakness and numbness Diffuse weakness in legs. Spinal fluid helpful in determining in legs (both proximally Diffuse sensory abnormalities in Poly aetiology (cytomegalovirus or herpes and distally), with legs and buttocks radiculitis simplex virus infections – bowel/bladder Reduced/absent reflexes at lymphomatous infiltration). incontinence knees and ankles. CD4 >500 or <50 Weakness and spasticity mainly Stiffness and weakness in in hip flexors, knee flexors, ankle Spinal fluid may show elevated legs with leg numbness. dorsiflexors. protein, mild (5-10 cells/mm3) or no Vacuolar Bowel/bladder Brisk knee jerks, upgoing toes pleocytosis. myelopathy incontinence in advanced ("Babinski's sign"). If sensory No specific therapy. cases. neuropathy coexists, then distal Physical therapy often helpful. CD4 <200 sensory loss and reduced/absent jerks will also be seen. Diffuse weakness including facial Inflammatory Predominantly weakness musculature, asymmetric in early Spinal fluid shows a very high demyelinating in arms and legs, with cases, with diffuse absent protein with mild to moderate polyneuro minor sensory symptoms. reflexes. lymphocytic pleocytosis, but all pathies CD4 >500 or <50 Minor sensory signs. cultures are negative.
PART 1-ADULTS 65 II.12 STEPWISE TREATMENT OF PAIN ADULTS
First line analgesics, include Acetylsalicylic Acid (600 mg every 4 hours) or Paracetamol (1 g every 6 hours). Second line treatment: weak opined drugs in combination with first line treatment such as and Codeine phosphate 60 mg every 4 hours. Compound analgesics (such as Betacod) contain sub-therapeutic doses of codeine and should not be used for this purpose. For severe pain, oral or injectable Morphine is given. Treatment is mostly started with 5-20mg every 4 hours. The dosage of Morphine should be based on the response and often needs to be increased while the disease progresses. For very severe pain there is no maximum dose.
Never combine morphine with a weak opioid (such as codeine or Tramadol).
Some pains do not respond well to morphine. These include bone, neuropathic and visceral pain. These pains often respond to adjuvant drugs or specific therapy (for example cytotoxic drugs in case of severe pain due to tumours, such as Kaposi sarcoma).
Adjuvant drugs may be added at any stage according to the type of pain: Anticonvulsants such as Carbamazepine 200 mg tds are given for pains of a nervous origin such pain after Herpes zoster. Antidepressants, such as Amitriptyline 10-25 mg at bed time are given for the tingling sensation and burning pains of peripheral HIV neuropathy and nerve compression. Non-steroid anti-inflammatory drugs (NSAID) are used in case of pain of bone pain, pain of inflammatory origin, such as in rheumatic conditions and hepatomegaly. Haloperidol (1.5 mg at bed time or twice daily) reduces some of the side effects of Morphine (such as nausea and agitation).
PART 1-ADULTS 66 Avoid peaking of pain by maintaining an appropriate level of analgesic therapy. Most patients with AIDS in a final stage will have severe pain and will benefit from adequate analgesic therapy. At this stage oral morphine, often in combination with adjuvant drugs, will be indicated.
Some secondary effects of Codeine and Morphine are beneficial for persons with HIV disease, such as constipation, depression of cough reflex and mood alteration. In the presence of pain, respiratory depression is never a problem. Nausea occurs in most patients only during the initial 2 weeks of treatment with Morphine and may be reduced by adjuvant drugs such as Haloperidol, Chlorpromazine or Hydroxyzine.
Table 9: ANALGESIC DRUGS RECOMMENDED FOR PAIN IN HIV DISEASE
Drug Dosage
Mild pain
Aspirin 600 mg every 4 hours Paracetamol 1 g every 4 hours
Moderate pain
Codeine 60 mg every 4 hours
Severe pain
Oral or injectable opioid drugs, Minimum 5mg every 4 hours. In such as Morphine severe pain there is no maximum dosage (sometimes even more than 500mg every 4 hours is needed) Adjuvant drugs
Anticonvulsants Carbamazepine 200 mg tds Antidepressants Amitriptyline 10-25 mg at bed time Non-steroid anti-inflammatory Ibuprofen 200-400mg tds drugs (NSAID) Indomethacin 25mg tds Axiolitics, hypnotics Lorazepam 1mg at bed time Hydroxyzine (Atarax) 25mg tds Antihistamins Promethazine 10mg at bed time Haloperidol 1.5 mg at bed time or Neuroleptics twice daily
PART 1-ADULTS 67 II.13 ANAEMIA IN HIV DISEASE ADULTS
CLINICAL SUSPICION OF ANAEMIA
History, physical examination and Hb test (where possible) (A)
Bleeding (e.g. epistaxis, haemoptystis, bloody YES diarrhoea, vaginal bleeding?) Jaundice Fever Hb<10
NO
Supportive treatment Follow-up
Refer to level 2 for further investigat NO Improved? ion and manage ment (B) YES
Follow-up as needed
PART 1-ADULTS 68 ANNOTATIONS FOR THE MANAGENMENT OF ANAEMIA IN HIV DISEASE ADULTS
A. Definition: Moderate anaemia: Hb values of 5-10 g/dl. Severe anaemia: Hb values of less than 5 g/dl.
Anaemia is a frequent clinical and laboratory finding in HIV positive patients. Anaemia may also be the first clinical manifestation of HIV infection. Clinical signs, such as paleness of the conjunctiva, tachycardia and general weakness should raise suspicion about the presence of anaemia. Clinical signs and symptoms are not sufficiently accurate to diagnose anaemia or to assess its severity. Where possible, a laboratory test to assess the Hb level should be performed.
B. Supportive treatment for anaemia: Iron supplement: ferrous fumarate 200mg plus folic acid 10mcg bd
C. Severe anaemia in persons with HIV should be investigated as usual and appropriate treatment should be given. Investigations for anaemia in HIV positive patients should always include: FBC LFT Urea, electrolyte status Stool analysis (microscopy, occult blood) Chest X-ray
Iron, Vitamin B12 and Folic Acid concentrations should be determined as indicated, depending on results of the above mentioned investigations and appropriate treatment should be given.
Severe anaemia, not responding to this therapy, should be further investigated by bone marrow aspirates or biopsy to identify possible bone marrow infiltration due to tuberculosis, metastatic carcinoma or fungal infections, for which specific management may be envisaged. Blood transfusion does not affect the result of bone marrow examination. In severely anaemic patients blood transfusion should therefore not be delayed for this purpose.
PART 1-ADULTS 69 Table 10: Anaemia in HIV disease
Types of Anaemia: Cause Hypochromic microcytic Epistaxis cause due to thrombocytopenia anaemia Hemoptysis due to TB, necrotising pneumonia (Klebsiella, Staphylococcus aureus), Kaposi sarcoma GIT bleeding due to peptic ulceration, bloody diarrhoea, Kaposi sarcoma Tumors (GIT lymphoma, Kaposi sarcoma) Nutritional Malabsorption syndrome Macrocytic anaemias Vitamin B12 and folate deficiency due to Malabsorption Existing liver disease Haemolysis with reticulcytosis due to auto-immune reactions Thrombocytopenic purpura Disseminated Intravascular Coagulation (DIC) Haemolytic Uraemic syndrome Drugs such as Sulfamides, Zidovudine Cytopaenias Due to reduced production or accelerated destruction of formed elements: Septicaemia, Anti-Erythrocyte antibodies, Anti-platelet antibodies Anti-neutrophyl antibodies HIV induced Normocytic normochromic Chronic infections e.g. TB, fungal anaemias infection Chronic renal failure Drugs e.g. Zidovudine (AZT), Lamivudine (3TC) HIV induced bone marrow suppression
Leukopenia is also common in persons with HIV. There is much variation in the individual level of white blood cells. A level of 3,500 WBC/ml requires further investigation to determine eventual treatable causes.
PART 1-ADULTS 70 II.14 GUIDELINES FOR FOLLOW-UP ADULTS
HIV infection leads to a chronic disease, which may last for several years before one dies from it. During this prolonged course, one starts off by having no symptoms for an unknown period before he/she develops them.
Asymptomatic HIV infection
One may become aware of the sero-status through an HIV test. This may have been performed voluntarily, or as a requirement for medical examination for various reasons, such as securing a scholarship or for insurance purposes. The HIV test may also have been carried out in an asymptomatic person, who is a sexual contact of a known patient with HIV.
The objective of follow up of an asymptomatic HIV infected person include:
Promote positive living. To offer support through counselling, etc. so that the person can cope with the knowledge of being HIV infected. To educate and inform the person with HIV about various aspects of HIV infection in order to promote positive living with HIV and delay the onset of disease (such as exercise, hygiene, nutrition, regular lifestyle, safe sex, contraception, social contacts, etc.). To facilitate referral to the range of existing organisations and facilities which may provide assistance for various problems which may arise (psychological, medical, social, financial, spiritual, legal, etc). To detect early any HIV related disease and to institute prompt management.
It is suggested that asymptomatic HIV infected persons should be reviewed once every 3-6 months at level 1. A detailed history of possible HIV related symptoms should be taken and a physical examination carried out. Patients should be advised that they should seek medical attention whenever they develop suspicious symptoms.
The following basic care of early HIV disease should be considered:
Monitoring A detailed history of possible HIV related symptoms should be taken and a physical examination at each visit Baseline complete blood count (may be repeated annually)
Diagnosis and/or treatment of occult infections RPR-test for active syphilis PPD (or Tine test) testing for previous contact with TB Stool examination or epidemiological treatment for intestinal parasites may be considered depending on the prevalence of these infections in the community.
PART 1-ADULTS 71 Maintenance of optimal health Dental care: it is advisable to consult a dentist at the time of HIV diagnosis and at least annually thereafter Health promotion on nutrition, hygiene, safer sex, contraception, etc. Assessment for ongoing counselling needs and referral for significant problems to relevant services (health workers, social workers, legal assistance, unions, religious leaders, etc.)
Symptomatic HIV disease
The objective of follow-up of symptomatic patients is to established and treat promptly any HIV related problems which may be found after a detailed history and physical examination. This is likely to slow down the rate of immuno- suppression because it is known that the longer it takes to treat an opportunistic infection, the worse the immune status becomes.
It is suggested that the frequency of visits should depend on the condition of the patient at the time of presentation. The very sick should be seen within 1-2 weeks and those who are moderately sick can be reviewed every month, while those with minimal symptoms and signs can be seen once every 3-6 months.
Supportive treatment
In the different sections of the guidelines, supportive treatment is highlighted for symptomatic patients. A balanced nutritious diet is the most important supply of energy, vitamins and minerals. Most traditional diets provide a balanced diet at low cost. This may, however not always be available due to drought, poverty and migration to an urban environment.
Nutritional supplements: 200 mg Fe fumarate plus folic acid 10 microgram once daily 200,000 IU (1 capsule) of vitamin A once weekly Multivitamins once daily may be added if the supply of vitamins through nutrition may be insufficient.
Prophylactic treatment
Pneumocystis carinii and Toxoplasmosis
Co-trimoxazole at a dosage of 1-2 tablets once daily is effective in preventing pneumonia due to Pneumocystis carinii (PCP) and meningitis due to Toxoplasma gondii (The higher dose of 2 tablets is recommended for the prevention of T. gondii). It is also effective to suppress Isospora belli infection and may reduce the incidence of pulmonary and skin infections by gram positive organisms (streptococci, staphylococci).
PART 1-ADULTS 72 Indications: History of Pneumocystis pneumonia CD4 count of less than 200 cells/cubic mm Lymphocyte count of less than 1000 cells/cubic mm Oral thrush TB treatment
Tuberculosis
HIV positive persons who are PPD positive have a 5-8% annual risk and a 30% or more lifetime risk of developing active tuberculosis. In addition, these people may then transmit the disease to their close contacts8. In addition, these people may then transmit the disease to their close contacts.
The rationale behind preventive therapy is to eradicate latent infection in PPD positive people before it develops Prophylactic treatment with INH 300mg p.o. per day for 6 months reduces the incidence of tuberculosis in persons with HIV and a positive tuberculin skin test by about 50% during the period of prophylaxis. Because the risk of peripheral neuropathy is already high in HIV positive patients, pyridoxine 25mg p.o. should be given together with INH. There is no justification to prescribe TB prophylaxis to PPD negative persons with HIV, as prophylaxis does not reduce the incidence of TB in these patients.
Active TB should be excluded before prophylaxis is considered. In the presence of any symptom, which may be due to TB (cough, fever, lymph node swelling, etc.) prophylaxis should be postponed and if symptoms persist, further investigations should be carried out.
Persons with HIV immuno-suppression are at high risk for re-infection after completion of the prophylactic treatment. Clinicians should therefore also in these patients consider TB as a possible cause of respiratory symptoms.
Careful selection of patients is essential for prophylaxis to be successful. Prophylaxis may be initiated at any stage of HIV disease (including asymptomatic persons). Good compliance is essential as INH resistant strains may be selected by intermittent treatment. Selection criteria include: A positive tuberculin skin test Patients should be highly motivated or live under conditions where supervised prophylaxis is ensured (such as workplace-based distribution, HIV infected health workers, prison services, etc.).
In non-compliant patients, prophylaxis should be discontinued. No further efforts should be done to restart prophylaxis.
PART 1-ADULTS 73 Prophylactic treatment in pregnancy
Pneumocystis carinii and Toxoplasmosis
Co-trimoxazole at a dosage of 1-2 tablets once daily is effective in preventing pneumonia due to Pneumocystis carinii (PCP) and meningitis due to Toxoplasma gondii. There are theoretical concerns about the use of Co-trimoxazole in the first and third trimester, although no relationship with either teratogenic effects or neonatal kernicterus has been confirmed.
Tuberculosis
Prophylactic treatment with INH 300mg p.o. per day for 6 months plus pyridoxine 25mg p.o. should be considered in PPD positive pregnant women that did not yet receive this treatment. INH is not associated with maternal or foetal adverse effects.
Active TB should be excluded before prophylaxis is considered. In presence of any symptom, which may be due to TB (cough, fever, lymph node swelling, etc.) prophylaxis should be postponed and if symptoms persist, further investigations should be carried out.
Maintenance treatment
Some opportunistic infections are not cured after initial treatment and therefore require life-long maintenance treatment.
Cryptococcal meningitis Amphotericin B 0.6-1mg/kg once or twice per week Toxoplasma encephalitis Pyrimethamine 25-50mg/d plus folinic acid 10mg/day plus Sulfadiazine qid Oral thrush (Candida) Nystatin 500,000 IU qid OR Ketoconazole 200mg/d po.
PART 1-ADULTS 74 II.15 MEDICAL MANAGEMENT OF ADVANCED HIV DISEASE ADULTS
A patient with terminal illness is often uncomfortable due to one or more of the conditions below. Good palliative and supportive care should address these conditions.
1. Psychological support In the terminal stages of HIV disease, one of the most important components of care is psychological support. This support is usually give by family, friends, relatives, members of the community and spiritual leaders, with the support of professional health staff, social workers and trained community counsellors.
2. Pain control In terminal stages, pain should be minimised by effective management. Strong analgesics in high dosage, such as oral or im Morphine, might be indicated at this stage (see chapter on pain).
3. Anxiety and insomnia Good counselling and family support are essential to handle these conditions. Long acting anxiolytics (such as Diazepam) may further increase weakness. Short acting drugs, such as Lorazepam are more appropriate for insomnia. Hydroxyzine can be used to treat anxiety and insomnia and does not increase weakness. This drug is also useful in combination with Morphine.
4. Dementia Dementia is a progressively worsening condition of physical and mental incapacitation. It is usually caused by HIV infection itself and has no satisfactory medical treatment so it has to be handled palliatively. Again counselling and family and psychosocial support are the best forms of management. Medicinal management will depend on the state. Sometimes there is excitement almost approximating to psychosis. If this occurs, Haloperidol 2.5 mg tabl. bd or tds may be indicated.
5. Anorexia, nausea and vomiting There is no easy solution to loss of appetite in terminal illness. The family should be encouraged to continue providing frequent small amounts of food. Fluid meals may be tried, in particular if the patient has problems to swallow food. Oral rehydration may be necessary. Vitamin supplement should be given. Metoclopropamide 10mg tds may be beneficial in particular when nausea is present.
PART 1-ADULTS 75 6. Hiccup Hiccup is common in severe HIV disease and usually difficult to manage. Treatment with Metoclopropamide po 10mg tds, Haloperidol 2.5 mg po bd or tds. Alternatively, Chlorpromazine, 100 mg bd or tds may be beneficial. However these drugs are usually sedative and should be taken with caution.
7. Pressure sores The family should be taught to turn the patient at least once every two hours. If the pressure sores develop, they should be kept clean and dry.
8. Care for the mouth Maintenance of oral hygiene and reducing symptoms of dry mouth by stimulating saliva (by sugar-free chewing gum or chewing palm leaves). The family should be taught to clean the mouth using a piece of wet cloth and salt water after every feed.
9. Terminal respiratory distress Many terminally ill patients develop dyspnoea as they near their death. This may be due to pneumonia or due to an untreatable chest condition like Kaposi sarcoma. Good ventilation and putting the patient in a comfortable sitting position should be done. Oxygen may give relief when available. This condition is very stressing for patients and families, which may require treatment with oral Morphine as needed every 4h plus Hydroxyzine 25 mg tds.
10. Caring for the carers People who look after terminally ill infected patients, for example family members, relatives and health workers, need psychosocial support themselves. This can be provided in the form of counselling directed towards them by interdisciplinary team members and by mutual support by community members.
PART 1-ADULTS 76 II.16 ANTIRETROVIRAL TREATMENT ADULTS
During recent years, the medical management of HIV disease in high-income countries has changed drastically as a result of the availability of antiretroviral drugs. Antiretroviral drugs act directly on the replication of HIV. Antiretroviral treatment aims to reduce the viral load to a minimum level for a prolonged period by combining Antiretroviral drugs.
At present three classes types of antiretroviral drugs are available in Namibia: Nucleoside Reverse Transcriptase Inhibitors (NRTIs): these drugs inhibit the transcription of viral RNA into DNA, which is necessary for reproduction of the virus. It includes Zidovudine (ZDV or AZT), Lamivude (3TC), Didanosine (DDI), Zalcitabine (ddC), Stavudine (D4T) and Abacavir (ABC). Non-Nucleoside Transcriptase Inhibitors (NNRTIs): these are of a chemically different class than NRTIs and also inhibit transcription of viral RNA into DNA: Nevirapine (NVP), Efavirenz (EFV) and Delavirdine (DVL). Protease inhibitors (PIs): act on the viral enzyme that cuts long chains of amino-acids into smaller proteins. It in includes Indinavir (IDV), Nelfinavir (NFV), Sequinavir (SQV), Ritonavir (RTV) and Amprenavir (APV).
Antiretroviral drugs can be used to prevent new HIV infections, for example to reduce HIV transmission for example after needle stick injuries of health workers or rape. This is called Post Exposure Prophylaxis (PEP). Antiretroviral drugs can also be used to reduce mother-to-child transmission of HIV. The use of antiretroviral drugs for this purpose is not discussed in the context of these guidelines, which focus on clinical management of HIV disease.
Principles of Antiretroviral Therapy
In patients with an established HIV infection, about 100 to 1,000 million virus particles are produced and cleared each day. The concentration of virions in the blood (also called the viral load) reflects the amount of virus production in the body and is the best predictor of the progress of the disease9: persons with a low viral load survive longer than persons with a high viral load.
In all patients with HIV, the virus replicates rapidly and viral strains with resistance towards antiretroviral drugs emerge fast if these drugs are used as monotherapy. A combination of 2 transcriptase inhibitors is also insufficient to reduce viral load sufficiently to achieve a durable effect the course of HIV disease10. Several randomised controlled trials have shown that sustained suppression of the viral load can be achieved by various combinations of 3 drugs. This treatment approach is known as Highly Active Anti-Retroviral Treatment (or HAART) and has become the standard antiretroviral treatment of symptomatic HIV infection.
PART 1-ADULTS 77 Effects of HAART The introduction of HAART on the course of HIV disease in high-income countries has resulted in a drastic decline in AIDS related morbidity and mortality 11,12. Sustained and progressive immunological reconstitution has been observed. When optimal response to treatment is achieved, the median CD4 cell rise is 100- 200 cells within the first year. Maintenance or prophylactic treatment for several opportunistic infections may be discontinued in these patients.
Limitations of HAART Although HAART has become the cornerstone of HIV disease management in situations where it is available, there are various limitations: HAART does not eliminate the virus. Treatment fails to control viraemia in clinical trials in about one third of patients.13. Viraemia rapidly increases after stopping therapy (or even after stopping one of the three drugs). Patients should therefore continue treatment for the rest of their life. Emergence of resistant HIV strains frequently occurs in particular if patients have low compliance. Failure is more likely in advanced disease.14 Adherence to therapy for a long period is difficult. A decline of compliance to antiretroviral therapy over time has been documented in all studies15. Sexual transmission of HIV may continue to occur, even if viral load is at an undetectable level in serum and sexual transmission of strains resistant to the 3 drug regimen of HAART has already been documented16 17. Short-term side effects of treatment are common (anaemia, neutropenia, nausea, headache, abnormal fat distribution). Long term side effects are unknown. Drug interactions are frequent. At present, there are few alternative treatment options for patients, which do not respond to the recommended ARV drugs, discontinue treatment due to side effects or developed resistant viral strains.
Table 11: Advantages and Limitations of HAART Advantages of HAART Limitations of HAART Morbidity and Mortality declines No cure, treatment should be taken life-long Effective in most, but not all patients Long-term prognosis unknown Sustained suppression for several years can Strict compliance of treatment required be achieved in a considerable proportion of Close monitoring needed to adapt treatment patients when resistance develops Resistant strains can be transmitted by unprotected sex Patients receiving HAART remain productive Side effects of some drug regimes may reduce quality of life Immune system recovers reducing the need Opportunistic infections may still occur, for prophylaxis of opportunistic infections especially if treatment is started at low initial CD4 levels Reduced HIV transmission from mother to MTCT may still occur child Reduced cost of hospitalisation and orphan Recurrent costs for drugs and monitoring of maintenance treatment Availability of HAART encourages persons Accessible high-quality services required to with HIV to seek diagnosis and to voluntarily ensure counselling and medical follow-up. disclose their HIV status
PART 1-ADULTS 78 Availability and Cost of HAART in Namibia Most antiretroviral drugs are available in Namibia through private pharmacies. The monthly drug cost at wholesaler prices for different HAART regimes varies between N$ 2,300 and N$ 3,700. With additional mark-ups of individual pharmacies or dispencing docters, patients or their medical aid schemes are charged an additional 10-30%. To facilitate the access to HAART, initiatives have been taken by international agencies and action groups to reduce the prices of antiretroviral drugs by negotiating with major drug companies or by promoting the access to alternative manufacturers of antiretroviral drugs (in India, Thailand, Brazil, etc.). These initiatives may reduce the cost of drugs to less than N$ 1,000 per month.
Table 12: Antiretroviral drug regimes for HAART
(One from Column A and Column B) Column A Column B Efavirenz (preferred) AZT+ddI Indinavir (preferred) ddI+3TC Nevirapine (alternative) d4T+ddI Ritonavir (alternative) AZT+ddC Saquinavir (SQV) AZT+3TC +Ritonavir Nelfinavir d4T+3TC
Required conditions for the implementation of HAART The following conditions are essential for appropriate provision of HAART: Easy access to voluntary counselling and HIV testing (VCT) for early diagnosis of HIV infection. Identification of sufficient resources to pay for HAART on a long-term basis. Counselling for the patient and his/her environment to ensure full understanding of HAART, the importance of treatment compliance, timing of drug intake in relation to meals and possible side effects of HAART. Follow-up counselling of the patient and his/her environment to ensure continued psychosocial support and to enhance adherence to treatment. Capacity to recognise and appropriately manage common HIV related illnesses and opportunistic infections. Reliable laboratory monitoring services including routine haematological and biochemical tests for the detection of drug toxicity CD4 counts and viral load. Assurance of an adequate supply of quality drugs, including drugs for treatment of opportunistic infections and other HIV related illnesses. Availability of interdisciplinary health teams, including doctors, nurses, counsellors, social workers. These teams should where possible assist in the establishment of support groups of persons with HIV and their care givers. Availability of a system for training, continuous education, monitoring and feedback on safe and effective management of HIV disease and HAART. Availability of a reliable regulatory mechanism against misuse of antiretroviral drugs.
PART 1-ADULTS 79 Indications for HAART HAART is indicated for all persons with progressing HIV disease who have a CD4 count of less than 200 cells per ml and can afford the sustained cost of diagnostic tests, purchase of drugs and comprehensive medical follow-up. Possible drug interactions should be considered before initiating HAART and any treatment of other conditions in persons receiving HAART.
Laboratory monitoring For initiating treatment and for follow-up of HIV disease the following diagnostic tests are required to assess the baseline parameters and to monitor the effect of treatment.
Table 13: Diagnostic tests for HAART
Diagnostic test Frequency HIV test First visit Full blood count Every visit Renal function tests Every visit Complete Urine analysis Every visit Liver enzymes Every visit Hepatitis B serology At initiation RPR test At initiation CD4+ cell count Every 3 months Viral load with sensitive test Every 3-6 months
When not to give HAART Asymptomatic patients with CD4 of more than 500 and low viral load (less than 10,000 copies/ml). Initiating HAART in terminal patients with very low CD4 levels is unlikely to result in significant restoration of the immune system. The gain in duration and quality of life, if any, is therefore likely to e limited. .
Timing for initiation of HAART There are still discussions on the timing of antiretroviral therapy. Results of HAART are better when the immune system still has sufficient capacities to recover (at a CD4 level of more than 200 cells/ml). HAART should also be considered in case of symptomatic HIV disease, regardless of CD4 levels. Some experts argue that starting earlier will have the advantage of maintaining the immune system at an even more effective level, for example when the patient is asymptomatic and CD4 counts are 350/ml or more, or when viral loads are high (above 30,000 copies/ml).
Other experts argue that delaying treatment allows patients to continue longer to lead a normal life, to be more compliant when treatment is needed and to save drug expenditures18. Recent studies seem to confirm there are no therapeutic advantages of starting HAART in asymptomatic patients at CD4 levels higher than 200 cells/ml even if the baseline viral load is high.
PART 1-ADULTS 80 Experience with HAART in developing countries suggests that the majority of patients start treatment at CD4 levels well below 200 cells/ml. In this situation, the theoretical discussion regarding early initiation of HAART is irrelevant. In the Namibian context, efforts should be focused on diagnosing HIV early and monitoring of CD4 levels to ensure that HAART is started in time to ensure maximum benefit.
Indications to change treatment
Change therapy due to drug toxicity: substitute one or more alternative drug of the same potency and from the same class of agents as the agent suspected to cause the toxicity.
Change therapy due to drug failure: Specific criteria should prompt for changing therapy to a totally new regimen: Individuals who have been receiving incompletely suppressive Antiretroviral Therapy, such as single or double nucleoside therapy Individuals who are receiving HAART and viraemia has never been suppressed below detectable limits after 4-6 months Patients receiving HAART with initially suppressed viraemia to undetectable levels that have developed detectable viraemia. The degree of plasma viraemia increase should be assessed and might be due to infection, vaccination, test methodology or lack of adherence. Further observation should be considered if viral levels remain less than 5000 copies/ml. Persistently declining CD4 T cell count numbers, as measured on at least two separate occasions. The effect of HAART should be assessed in case of clinical deterioration and therapy should be changed or discontinued if necessary.
PART 1-ADULTS 81 PART 1-ADULTS 82 PART II: MANAGEMENT OF HIV DISEASE IN CHILDREN
II.17 GENERAL CONSIDERATIONS REGARDING HIV INFECTION IN CHILDREN
The management of childhood HIV/AIDS is a task of health workers at each level of care. All health workers in clinics, health centres and OPD departments of hospitals need to be able to diagnose HIV infection, to provide routine follow-up, to manage the common medical complications and to refer patients to the next level.
The vast majority of HIV positive children are infected vertically, i.e. the virus is transmitted through Mother-to-child-transmission (MCTC). HIV cannot be transmitted by direct contact, such as hugging or kissing a child, changing nappies, bathing or playing. A small percentage of infections in children is attributed to sexual transmission due to sexual abuse.
Antibodies to HIV of infected mothers pass through the placenta during pregnancy. All children born to HIV positive mothers therefore have a positive HIV test. However, only about one third of these infants will be infected by the HIV virus of the mother. Infection may occur during pregnancy, during delivery or postnatally (through breastfeeding).
Transmission is affected by: The maternal stage of disease (high transmission due to sero-conversion of the mother during pregnancy or breast-feeding and advanced HIV disease) Viral characteristics (some subtypes replicate rapidly and are transmitted more easily). Factors related to the delivery (transmission is higher if the duration of rupture of membranes is longer than 4 hours and for a second delivered twin child) Presence of other genital tract infections (STD). Duration of breastfeeding The viral load Administration of ARV treatment to the pregnant woman and/or the child
Mother to child transmission of HIV
Published estimates of mother-to-child transmission rates of HIV-1 in various countries in Africa range from 21 to 43%19. Most infections seem to occur during labour and delivery20. The transmission rate due to breastfeeding is estimated at 3% to 6% per year21. Transmission rates may therefore vary between countries and even within a country according to the particular circumstances. Table 4 presents a simplified representation of the rates And timing of HIV transmission from mother to child.
PART 2-CHILDREN 83 Figure 3: Estimated rates and timing of mother-to-child transmission of HIV
Infection through breastfeeding 11%
Transmission during delivery 11%
Transmission during pregnancy 11% Not infected 67%
HIV is a family disease. Diagnosing the infection in a child invariably means that the mother and often her sexual partner are infected. Ideally, the family should therefore be treated as a unit and support by family and community members should be encouraged as early as possible.
The natural course of HIV disease in children
HIV RNA levels in perinatally infected infants are generally low at birth (i.e., <10,000 copies/ml), increase to high values by age 2 months and then decrease slowly after the first year over the next few years of life. This pattern probably reflects the lower efficiency of an immature but developing immune system in containing viral replication and possibly a greater number of HIV-susceptible cells.
CD4+ T-lymphocyte count and percentage values in healthy infants who are not infected with HIV are considerably higher than those observed in uninfected adults and slowly decline to adult values by age 6 years. A paediatric clinical and immunologic staging system for HIV infection has been developed that includes age-related definitions of immune suppression Although the CD4+ absolute number that identifies a specific level of immune suppression changes with age, the CD4+ percentage that defines each immunologic category does not. Thus, a change in CD4+ percentage, not number, may be a better marker of identifying disease progression in children
CD4+ cell values can be associated with considerable variation due to minor infections and are therefore best measured when patients are clinically stable.
PART 2-CHILDREN 84 Table 14:
A small proportion of the children who are infected early in pregnancy, however, progress more rapidly to advanced HIV disease than those who are infected during labour or through breastfeeding. This early infection leads to a disruption of the thymus, the organ where CD4 and CD8 cells are produced. These children therefore have both low CD4 cell and CD8 cell counts. The immune system of these children therefore cannot respond to HIV infection22. Infants that are aged less than six month when they present with symptoms of HIV disease therefore usually have a shorter survival period than older children.
Figure 4: CD4 counts and Viral Load in Perinatally HIV infected Children
2000 200,000
Normal CD4 cell count 1800 180,000 CD4 Slow progression 1600 CD4 Rapid progression 160,000 Viral load
1400 140,000 l m / t s n e u 1200 120,000 i o p c o l c l e 1000 100,000 A C N
4 R
D V I C 800 80,000 H
600 60,000
400 40,000
200 20,000
0 0 0 2 months 1 yr 2 yrs 3 yrs 4 yrs 5 yrs 6 yrs 7 yrs 8 yrs Age
PART 2-CHILDREN 85 II.18 DIAGNOSIS OF HIV DISEASE CHILDREN
A: At present, the majority of children are diagnosed on the basis of symptomatic HIV disease and a positive HIV test of the mother or the child.
Passively transferred maternal HIV antibody may persist for up to 18 months. To establish a definitive serological diagnosis of HIV infection in a child the test should therefore be repeated at the age of 18 months.
Additional techniques exist for the detection of virus in children under 18 months. HIV infection can be definitively diagnosed in most infected infants by age 1 month and in virtually all infected infants by age 6 months by using viral diagnostic assays (PCR: DNA or RNA polymerase chain reaction). Due to their complexity and cost, these tests are currently not available in Namibia for routine management of HIV disease.
The pattern of HIV disease and their management is often different for children of various age groups. Some HIV related conditions are less frequent in children, such as TB and Kaposi sarcoma). Other conditions, such as Lymphocytic Interstitial Pneumonitis (LIP) are usually only found in children.
Dosages of drugs need to be adapted to the weight of the child. The management of HIV disease in children is therefore addressed in this separate section of the guidelines. For some clinical problems, such as oral and skin manifestations management is similar for children and adults. For the management of these conditions we therefore refer to part 1.
PART 2-CHILDREN 86 A classification of HIV infection is done on the basis of the following symptoms and signs.
Table 15:
PART 2-CHILDREN 87 II.19 PERSISTENT DIARRHOEA CHILDREN
PERSISTENT DIARRHOEA (A)
History and physical examination (B)
Rehydration with YES Dehydrated ORS (sachets or (C) home made), or parenteral fluids
NO
YES Hydration 1. Maintain hydration and general 2. Maintain nutrition condition improved?
NO
Refer to level 2 Continue at level 1
PART 2-CHILDREN 88 ANNOTATIONS FOR PERSISTENT DIARRHOEA CHILDREN
N.B. For the management of acute diarrhoea the general guidelines are used for HIV infected children as for children without HIV infection.
A: Definition: Persistent liquid stools for more than 14 days in a child with symptomatic HIV infection.
Aetiology: A pathogen will only be identified in between 15-50% of the cases. The following list shows the diversity of pathogens involved, the relative frequency differs geographically.
Protozoa: Giardia lamblia Entamoeba histolytica Cryptosporidium Isospora belli Bacteria: Salmonella (non-typhoid) Shigella Campylobacter jejuni Enterotoxogenic E. coli (ETEC) Mycobacterium (atypical, TB) Yersinia enterocolitica Viral: Rotavirus Cytomegalovirus HIV (AIDS enteropathy) Helminthic: Strongyloides stercoralis Fungus: Candida albicans
B: Especially when the child has fever as well, look for other cause of the diarrhoea, such as malaria, pneumonia, otitis and treat as indicated
Table 16: Assessment of dehydration MILD MODERATE SEVERE 1. Look at: Condition Well alert Restless, irritable *Lethargic or unconscious; floppy Eyes Normal Sunken Very sunken
Tears Present Absent Absent
Mouth and Moist Dry Very dry tongue Drinks normally Thirsty, drinks Thirst No thirst eagerly 2. Feel skin Goes back * Goes back slowly *Goes back very pinch Quickly slowly 3. Decide NO SIGNS of Presence of at least 2 Presence of 2 or more dehydration signs, including a * sign: signs, including at least 1 * MODERATE sign: SEVERE DEHYDRATION DEHYDRATION
PART 2-CHILDREN 89 PERSISTENT DIARRHOEA- LEVEL 1 CHILDREN Continu ed from Page 76
malnourished 1. Nutritional advise 2. Refer to level 2 (A)
Fever and or YES bloody stool? 1. Nalidixic Acid for 5 OR days Malnourishe fever and 2. If febrile, do tepid d? bloody stool sponging 3. Maintain nutrition and hydration (B) NO
1. Maintain hydration 2. Maintain nutrition 3. Observe for 10 days YES (E) Improved after 5 days? (C)
NO
Stop antimicrobial treatment Maintain hydration Maintain nutrition Refer to level 2 (D)
YES Improved? (C)
NO
Refer to level 2 Follow up as needed
PART 2-CHILDREN 90 ANNOTATIONS FOR PERSISTENT DIARRHOEA – LEVEL 1 CHILDREN
A: Maintenance of nutrition: advise the mother not to stop breast-feeding and to continue feeding the child. The overall health of the child will be better if the caloric intake can be maintained. It is not so important what the child is eating, but that it eats.
B: Children with symptomatic HIV infection often have persistent diarrhoea without underlying intestinal infection, but one course of antimicrobial treatment is given to treat possible causative agents. In case of diarrhoea with blood and fever, treat with Nalidixic Acid (50 mg/kg per day divided in 4 doses). If the child has received a course of antimicrobial treatment for persistent diarrhoea within the previous 3 months, do not repeat treatment with Nalidixic Acid and consider referral.
C: For the purpose of this guideline, improvement is defined as follows: 1. The child is in a clearly better state of health, with no signs of dehydration 2. Fewer stools than before, and 3. No fever and less blood in stool if fever and blood were present.
D: If no improvement is noticed after 5 days stop all antimicrobial treatment. It is very unlikely that the child will have again an infection sensitive for these drugs. In areas where Strongyloides is prevalent, treatment with Albendazole should be considered (200 mg for 3 days, to be repeated after 3 weeks). If the child is not improving, referral to level 2 should be considered, while maintaining hydration and nutrition.
E: Persistent diarrhoea is a common presentation in HIV infected children. If the child is not severely ill (no bloody stool or fever, not dehydrated or malnourished) observe the child for 10 days, while hydration and nutrition are maintained.
The basic principle of management of persistent diarrhoea in children with symptomatic HIV infection involves two components:
1. Maintenance of hydration, by giving ORS, also in cases the child is not dehydrated. If a child is well hydrated then the appetite may improve and the child feels better in general
2. Maintenance of nutrition, by advising the mother not to stop breast- feeding and to continue feeding the child. The overall health of the child will be better if the caloric intake is maintained. It is not so important that the child eats, but that he eats. Mothers often ask for medicine that will increase the appetite of the child. Multivitamins may be given to ensure sufficient vitamin intake and to respond to the demand of mothers.
PART 2-CHILDREN 91 PERSISTENT DIARRHOEA – LEVEL 2 CHILDREN
Referred patient with persisten t diarrhoea
bacterial infection and/or Stool examination bloody stool Treat as (B) indicated [D]
Are findings consistent Metronidazole with (C): YES 10 mg/kg tid Bacterial infection or for 5-10days bloody stool with or Protozoal (E) without fever? Protozoal infection Helminthic infection
helminths Albendazole NO 200 mg (F)
YES Manage as Malnourishe indicated d?
NO
Maintain nutrition Maintain hydration Return after 10 days
YES Follow up Improved? as needed (G)
NO
Re-evaluate (H)
PART 2-CHILDREN 92 ANNOTATION FOR PERSISTENT DIARRHOEA – LEVEL 2 CHILDREN
A: For all patients with diarrhoea supportive treatment is continued (or started when not given previously) upon arrival: 1. Adequate (oral or IV) hydration as indicated 2. Continued nutrition, including breastfeeding 3. No anti-emetic or antispasmodic drugs
B: For all patients, not responding to treatment at level 1, a fresh stool culture should be done. It is important to examine the stool as fresh as possible. Multiple stool examinations increase the diagnostic yield. In many cases (up to 50%) however, no aetiologic agents may be identified.
C: Look for faecal blood and neutrophils on faecal smear. These findings may support the diagnosis of bacterial infections (Shigella, Salmonella, and Campylobacter). E. Histolytica, ulcerative colitis and Clostridium difficile must also be considered.
D: Fever and/or bloody stools are more indicative of bacterial infection. Malnutrition puts the HIV infected child at an increased risk of dying from persistent diarrhoea. Other possible causes of fever, such as pneumonia, otitis etc, need to be excluded and, if present to be treated appropriately. Children with fever, living in endemic areas should always be treated for malaria during the malaria season.
E: For Entamoeba histolytica infection Metronidazole (10 mg/kg tds for 10 days) is prescribed and for Giardia lamblia Metronidazole 10m m/kg bd for 5 days. Isospora belli should be treated with Co-trimoxazole for 3 weeks: (children 1-5 years: 5ml of syrup of 200mg sulfamethoxazol+40mg trimetroprim/5ml bd; children 6-12 years: 1 tablet 400mg sulfamethoxazol+80mg trimethoprim bd). There is no proven effective treatment for Cryptosporidium infection. This infection should therefore be managed only with supportive treatment.
F: For most helminth infections, treatment consists of a single of Albendazole 200mg for children under 2 years of age and Albendazole 400mg for children of 2 years and older. In areas where Strongyloides is prevalent, treatment with the same dosage of Albendazole per day for 3 days, should be considered. Treatment should be repeated after 3 weeks.
G: For the purpose of these guidelines, improvement is defined as follows: 1. The child is in clearly better state of health, with no signs of dehydration 2. Fewer stools than before, and 3. No fever and less blood in stool, if fever and blood were present
H: Further evaluation should include investigations to exclude lactose intolerance, tuberculosis, typhoid, urinary tract infection, etc.
PART 2-CHILDREN 93 II.20 ORAL THRUSH – LEVEL 1 CHILDREN
ORAL THRUSH (A)
Poor feeding or YES dysphagia and/or crying while swallowing or vomiting (B)
NO
Presumed oral thrush Presumed oesophageal only Candidiasis
Oral hygiene Gentian violet 1% solution tds for 5 days.
1. Nystatin suspension NO 500,000 IU qid for 5 days Improved? 2. Nystatin tablets 500,000 IU tds for 5 days (C)
YES
YES Improved?(D)
Follow up as needed NO Consider Refer to maintenance level 2 treatment (D)
PART 2-CHILDREN 94 ANNOTATIONS FOR ORAL THRUSH – LEVEL 1 CHILDREN
A: Definition: Presumptive: The presence of the characteristic white plaques on the oral mucosa. These plaques, usually located on the palate often bleed when they are removed. In some cases it may present only as red mucosal surface.
Definitive: The demonstration of Candida albicans spores or pseudohyphae in mouth scrapings or biopsy
Aetiology: Candida albicans
B: In HIV infected patients with oral thrush Candidiasis may extend into the oesophagus. This will cause pain on swallowing, reluctance to take food, salivation, crying during feeding and weight loss. Untreated oesophageal lesions, even if causing only mild pain or discomfort may alter eating habits and add to poor nutrition of the child.
C: Severe oral thrush, manifested by plaques on tongue, soft an hard palates, and extending to the pharynx indicates a high likelihood of oesophageal Candidiasis, even in the absence of pain on swallowing. Nystatin oral suspension or tablets should therefore be given.
D: Although symptoms improve, prolonged treatment may be needed to clear fungal infection. If there is no improvement, refer for oral treatment with Ketoconazole or for further investigation if there is no improvement.
E: Recurrence of oral thrush and oesophageal Candidiasis is very common. Recent use of antibiotics is an important predisposing factor for developing oral thrush. Nystatin once or twice daily may be used for maintenance treatment.
For other oral manifestations of HIV disease, please consult Part 1 -Adults
PART 2-CHILDREN 95 Referred ORAL THRUSHpatient with LEVEL 2 CHILDREN oral thrush and malnutritio n or dysphagia
Do microscopic examination of mouth scraping (A)
Dysphagia or YES crying while YES Candida swallowing OR spores vomiting demonstrate OR severe oral d thrush (B) NO
NO Presumed oesophageal Other oral Presumed oral Candidiasis lesions? thrush only (C)
NO Oral hygiene Nystatin suspension 500,000 IU tid for 5 days (D)
NO Ketoconazole Improved 3-6 mg /kg daily for 5 days (E)
YES Resolved?
NO
Follow up as Continue treatment needed until resolved Consider Consider Re-evaluation prophylactic maintenance treatment (F) treatment (G)
PART 2-CHILDREN 96 ANNOTATIONS FOR ORAL THRUSH – LEVEL 2 CHILDREN
A: The microscopic identification of pseudohyphae and/or blastospores of Candida albicans confirms the diagnosis.
B: Candidiasis may extend in to the oesophagus in HIV infected patients with oral thrush and causes pain on swallowing, reluctance to take food, salivation, crying during feeding and weight loss.
C: Severe oral thrush, manifested by plaques on tongue, soft and hard palates an extending to the pharynx indicates a high likelihood of oesophageal Candidiasis, even in the absence of pain. Untreated oesophageal lesions even if causing only mild pain or discomfort may alter eating habits and add to poor nutrition of patients.
D: In case of severe oral thrush in breast feeding children, the nipples of the mother are often infected. Application of Gentian violet on the nipples before breast feeding is advisable. Candidiasis of the perineal area of the child should also be excluded. Alternative topical antifungal therapy may be available: Clotrimazole 1% or Nystatin tablets if oral suspension is not available.
E: Ketoconazole is an oral systematic anti-fungal agent. Use should be avoided in the presence of active liver diseases and in-patients receiving treatment with Rifampicin.
F: Oesophageal candidiasis has high likelihood of recurrence, therefore secondary prophylaxis (Nystatin once or twice daily) is recommended.
G: Oesophageal lesions heal slowly, although symptomatic response is usually prompt. Prolonged treatment is often required.
PART 2-CHILDREN 97 II.21 RESPIRATORY CONDITIONS LEVEL 1 CHILDREN
RESPIRATORY CONDITIONS (A)
NO Severe YES respiratory distress? (B)
1. Treat with Mild YES respiratory antibiotics and distress? 2. Advise mother to (B) give home care (C)
NO Improved YES after 3 days?
NO YES Cough longer than 15 days 1. Complete treatment 2. Follow up as NO needed
Consider empiral treatment with Amoxicillin 50 mg/kg per day for 5 days (E)
NO Improved?
Refer to YES level 2 (D) Follow up as needed
PART 2-CHILDREN 98 ANNOTATIONS FOR RESPIRATORY CONDITIONS – LEVEL 1 CHILDREN
A: Definition: Child with symptomatic HIV infection and respiratory symptoms of difficult breathing or persistence or worsening of cough
Aetiology
1. Infections Bacteria Viral Parasite Pneumocystis carinii Pneumonia (PCP) Mycobacteria: M. tuberculosis Atypical mycobacteria Fungi Candidiasis
2. Malignancies Kaposi Sarcoma Lymphoma
3. Other Lymphocytic Interstitial Pneumonitis (LIP)
The relative frequency of the different pathogens may differ geographically and according to age.
B: The severity of respiratory distress can be assessed on age and clinical grounds (see page 91)
C: Treat with antibiotics: Amoxycillin 50 mg/kg/day in 4 doses. Advise the mother to give home care: Continue breastfeeding the child, Give extra fluids prevent the child from chilling return immediately when the condition of the child worsens. Reassess the child after 3 days If the child is severely undernourished, refer for admission and treat as severe pneumonia In infants below 2 months of age pneumonia is always a severe condition and requires referral for admission and further management.
D: Refer the child to hospital for admission. Give supportive care: sufficient fluids, clear airway, oxygen, etc.
In children with severe dyspnoea, oxygen therapy is crucial. Start treatment with antibiotics immediately if transport may be delayed: Ampicillin 50 mg/kg iv STAT
E: If a child with symptomatic HIV infections has chronic cough or pneumonia, which does not respond quickly to treatment, the child should be referred for further evaluation.
PART 2-CHILDREN 99 RESPIRATORY CONDITIONS LEVEL 2 CHILDREN Referred patient with respirato ry condition
Start Respiratory YES supportive distress? treatment (A) (B)
NO
Do chest X-rays (C) Severe dyspnoea 1. Admit Severe malnutrition 2. Antibiotic Age <2 months treatment (E)
Start treatment on Mild dyspnoea the basis of a No malnutrition 1. Home care presumptive Age > 2 months diagnosis (D) 2. Antibiotic treatment (F) Sputum or , gastric aspirate ZN positive X-ray result Start treatment for PTB (D)
YES Improved Follow up as after 7 days? needed
NO
Cough YES longer than Re-evaluate 30 days Consider TB treatment trial NO (H)
Supportive treatment Follow up as needed (I) PART 2-CHILDREN 100 ANNOTATIONS FOR RESPIRATORY CONDITIONS – LEVEL 2 CHILDREN
A: See page 91
B: Supportive treatment should be started upon admission. Supportive treatment includes: oxygen, sufficient fluids, clear airway, etc.
C: A chest X-rays should be performed, but may not always distinguish disease aetiology. If possible the following additional investigations should be done: - sputum: microscopy, culture, AFB stain - ESR, white blood cell count - Blood culture if fever is present
D: The presumptive diagnosis, based on chest X-rays should be substantiated through clinical signs and additional investigations where possible: ZN stain of gastric aspirate, microscopy of pleural effusion etc.
Pneumocystis carinii pneumonia (PCP) is one of the common severe opportunistic infections occurring in children with HIV. It occurs frequently in children under 1 year of age and is associated with a very poor prognosis. PCP is characterised by sudden onset of fever, tachypnoea, hypoxaemia and a diffuse interstitial infiltrate on X-ray. Usual treatment is co-trimoxazole (20mg/kg per day of the trimethoprim component in 4 divided doses for 14-21 days).
Lymphocytic Interstitial Pneumonitis (LIP) is a slowly progressive interstitial lung disease of unknown aetiology, which commonly occurs in HIV infected children above the age of 1 year, characterised by mild tachypnoea, clubbing. And bilateral reticular nodular infiltrates and mediastinal lymphadenopathy on chest X-ray. LIP usually has a good prognosis. X-ray findings can be confused with miliary TB or PCP. No specific therapy is available for LIP, but steroids (prednisone 2mg/kg/day for 10-14 days) may be beneficial.
E: Admit the child to the hospital and give supportive care. Treat with antibiotics according to age: 0-3 months: Ampicillin 50-100 mg/kg/day IV in 4 doses PLUS Gentamycin 4 mg/kg/day IV as a single dose 4 mo-5 yrs Ampicillin 50-100 mg/kg/day IV in 4 doses OR Cefuroxime 50 mg/kg day IV in 3 doses >5 yrs Penicillin 50,000-100,000 IU/kg/day IV in 4 doses OR Cloxacillin 50-100 mg/kg/day IV in 4 doses if X-ray suggestive of Staphylococcus infection. If bacteria are isolated, treatment should be adapted according to sensitivity testing.
PART 2-CHILDREN 101 F: In infants below 2 months of age or severely malnourished, pneumonia is always a severe condition. The child should be admitted and managed as severe pneumonia (see E). If not severely malnourished, the child can be managed as an outpatient. Advise the mother on home care and treat with antibiotics: Amoxycillin 50 mg/kg per day for 5 days. Reassess after 3 days and follow up as needed.
G: Re-evaluation will include repetition of earlier performed investigations, as repeated examinations increase the diagnostic yield (stool examination, otitis media, postnasal drip). If further investigations do not result in a final diagnosis, a therapeutic trial of TB treatment may be considered. Tine test (grade II) or Mantoux (>5mm) is considered positive in HIV infected children.
H: Many HIV infected children have recurrent respiratory problems without identifiable underlying cause. Supportive treatment (adequate feeding, sufficient fluid supply and management of nasal secretions) is indicated. The child should be followed up as needed.
PART 2-CHILDREN 102 Table 17: Clinical assessment of respiratory distress
CLINICAL ASSESSMENT OF RESPIRATORY DISTRESS
The severity of respiratory distress is assessed on the basis of age and clinical examination:
All children of under 2 months of age: Should be referred if there is clinical suspicion: respiratory rate of >60 or chest indrawing (with or without cyanosis).
For children older than >2 months of age:
CLINICAL SIGNS CLASSIFY AS
No chest indrawing and upper respiratory tract No fast breathing infection or bronchitis (no pneumonia)
Fast breathing but no chest indrawing: Respiratory rate <1 year: 50 or more pneumonia Respiratory rate 1-2 years: 40 or more pneumonia
Fast breathing and Chest indrawing with or without severe pneumonia central cyanosis
PART 2-CHILDREN 103 II.22 PERSISTENT OR RECURRENT FEVER – LEVEL 1 CHILDREN
PERSISTENT OR RECURRENT FEVER (A)
Treat with antimalarials (in endemic areas) Start treatment Patient acutely YES with broad or seriously ill spectrum (B) antibiotics Refer to level 2 (C) NO
Sources of fever YES identified or highly Specific suspected (D) treatment Endemic area for malaria?
NO
Empirical treatment with Ampicillin 50mg/kg qid for 5 days (E)
YES Free of fever?
NO
Patient Presumed HIV Follow up clinically stable associated fever as needed (F) (G)
NO Refer to level 2
PART 2-CHILDREN 104 ANNOTATIONS FOR PERSISTENT OR RECURRENT FEVER – LEVEL 1 CHILDREN
A: Definition: Fever as the only obvious clinical presentation in an HIV infected child.
Persistent fever: is defined as a body temperature of > 37.5 °C for more than one episode during a period of 5 days. Recurrent fever: is defined as a body temperature of >37.5 °C for more than one episode during a period of 5 days.
Fever is common among HIV infected paediatric patients. Children may have fever as a consequence of common childhood illnesses, endemic diseases, serious bacterial or opportunistic infections, carcinomas and/or HIV itself. Under many of these circumstances the fever will be associated with specific localised signs and symptoms (i.e. respiratory, CNS etc). These situations are covered in other sections of this document. The HIV infected child with Fever of Unknown Origin (FUO) should be investigated in the same fashion as the child without HIV infection and FUO.
B: A very sick child with a temperature of 39 °C or higher.
C: 1. Treatment for malaria in endemic areas according to national guidelines. Do not give Chloroquine by injection if the child can take it by mouth. 2. Start treatment with antibiotics for possible septicaemia: Ampicillin 50 mg/kg iv STAT. 3. Refer the patient immediately to the nearest health facility with more diagnostic possibilities.
D: Each child with fever should be thoroughly examined to identify possible localised infections, in particular skin infections, abscesses, etc.
E: For many HIV infected children with fever and no localising findings, HIV itself may be the cause. The empirical treatment is intended to treat occult infections, such as urinary tract infections, otitis media, etc. If there is a suspicion of serious infection, requiring prolonged course of antibiotics (i.e. osteomyelitis or endocarditis), the patient should be referred to level 2.
F: The child has still fever but the clinical situation is stable, the child is attentive, eats and drinks.
G: Consider treatment with antipyretics. Maintain hydration and nutrition
PART 2-CHILDREN 105 Referred patient PERSISTENT OF RECURRENTwith FEVER – LEVEL 2 CHILDREN acute or persisten t fever
1. Admit 2. Investigate for possible cause 3. Treat with broad Patient acutely YES spectrum antibiotics or seriously ill? 4. Treat with (A) antimalarials (B) NO
Investigate to identify the possible cause of the fever (C) Source of fever identified
YES
Sources of YES Specific fever identified treatment or highly suspected? (C)
NO Empirical treatment with Amoxicillin 50 mg/kg qid for 5 days (D)
YES Free of fever
NO
Patient YES Presumed HIV clinically associated fever stable? (E)
NO Follow up as needed Re-evaluate (G) (F)
PART 2-CHILDREN 106 ANNOTATIONS FOR PERSISTENT OR RECURRENT FEVER –LEVEL 2 CHILDREN
A: A very sick child with temperature of 39 C or higher.
B: Investigation which should be carried out: Blood slides for malaria parasites, examination of CSF. Blood culture to diagnose meningitis and sepsis. Malarial treatment should also be given if the blood slides is negative. Treatment for malaria: Chloroquine, 10 mg/kg stat, followed by 10 mg/kg on the second day and 5 mg/kg on the third day (total dose 25 mg/kg). Do not give Chloroquine by injection if the child can take it by mouth.
Treatment with broad-spectrum antibiotics to treat presumed sepsis or meningitis: Ampicillin 200 mg/kg/day 6 hourly for 10 days PLUS Chloramphenicol 100 mg/kg/day 6 hourly
C: Examination, which is useful to identify possible causes of the fever: Malaria slide white blood cell count stool microscopy Blood culture urinalysis Widal Chest X-ray CSF ultrasound
For many HIV infected children with fever and no local findings, HIV itself is the presumed cause. However, other conditions need also to be considered including: - Occult bacterial infections i.e. chronic sinusitis, otitis media, urinary tract infection osteomyelitis, abscess, salmonellosis, syphilis, liver abscesses, endocarditis. - Mycobacterial infection – M. tuberculosis, M. avium - Fungal infections – Candida - Chronic viral infections – MCV, EBV - Parasitic infections – malaria, Toxoplasma - Neoplasms: lymphoma, Kaposi sarcoma, smooth muscle tumors The HIV infected child with true Fever of Unknown Origin (FUO) should be investigated in the same fashions the child without HIV infection.
D: The empirical treatment is intended to treat occult bacterial infections, such as urinary tract infections etc. If there is a suspicion of serious infections, requiring prolonged courses of antibiotics (i.e. osteomyelitis, endocarditis), the patient should referred to specialised facilities.
E: The child still has fever but the clinical situation is stable, the child is attentive, eats and drinks
F: Considered treatment with antipyretics and maintain hydration
G: It may be necessary to repeat some of the earlier investigations: Blood slides for malaria parasites and Borreliosis, blood cultures, stool examination. Repeat investigations may increase the diagnostic yield. If fever persists, the most likely cause is HIV associated fever. PART 2-CHILDREN 107 II.23 FAILURE TO THRIVE – LEVEL 1 CHILDREN
FAILURE TO THRIVE (A)
Home dietary trial: Feeding advice, Feeding YES increased calorie error intake through a (B) balanced diet (C)
Improved NO (D) NO
Refer to level 2
Identifiable 1. Appropriate contributing causes: treatment of cause YES vomiting, diarrhoea, 2. Home dietary trial oral thrush, (B) pneumonia, mouth ulcers or neurological diseases?
NO
Home dietary trial: Feeding advice, increased caloric intake YES Improved
1. Continue NO treatment Refer to until level 2 resolved. 2. Follow up as needed
PART 2-CHILDREN 108 ANNOTATIONS FOR FAILURE TO THRIVE –LEVEL1 CHILDREN
A: Definition: Failure to thrive should be suspected when a child deviated from it’s own apparent path of growth or when it deviates from the normal growth pattern for its age.
B: It is particularly important to take a detailed feeding and social history to assess the caloric intake and the social conditions, especially whether the mother is the caretaker of the child. The child should be weighed, the weight charted and a physical examination should be carried out to assess the degree of failure to thrive and any other obvious illness.
If prior weights are available, define points on a growth curve to assess severity.
If prior weights are not available, failure to thrive is defined as follows: - mild to moderate: weight 60% to 80% of normal weight for age - severe: weight lower than 60% of the expected weight for age OR weight 60% to 80% of the expected weight for age if oedema is present
To assess, as precisely as possible, the caloric intake, eating habits and schedules, breast feeding etc. should be described by the mother in details. The mother should tell exactly what the child is taking, how much and how often per day.
C: Give exact advice to the mother on the schedules and content of the diet: breast feeding, weaning foods and other foods. A balanced diet should contain sufficient proteins, fats, carbohydrates, vitamins and minerals. Make use of dietary advice of the nutrition unit for the use of local foods. If possible let the mother record exactly what the child takes and any problems she may come across. The dietary trial should be evaluated after 7 days. If possible a home visit should be made to assess the availability of resources at home and in the community.
D: Improvement is defined as weight gain with an increased alertness of the child, or loss of oedema (which may result in initial weight loss before weight gain).
E: The child will only benefit from referral when superior diagnostics and treatment facilities are available. Any referral should take into consideration: duration of illness clinical state of the patient prior investigations and treatment availability of resources at referral clinic
PART 2-CHILDREN 109 FAILURE TO THRIVE – LEVEL 2 CHILDREN Referred child with failure to thrive
YES 1. Home dietary trial: Feeding 2. Feeding advice Improve error? (A) 3. increased calorie intake. (B) d YES NO
If available do: 1. Treat 1. Chest X-ray appropriately Any specific YES 2. WBC, electrolytes, 2. Dietary trial. diagnosis? urea, creatinine (may include made? 3. Urine analysis and naso-gastric microscopy feeding) (B) (E) 4. Stool microscopy NO and culture 5. Blood culture 6. LFTs Home dietary trial: 1. Feeding advice, 2. Increased calorie intake. (B)
YES Improved? (C)
NO 1. Continue treatment until resolved Re-evaluate (F) 2. Follow up as needed
1. Treat YES Specific appropriately diagnosis? 2. Home dietary trial 3. Follow up as needed NO Probably HIV related failure to thrive (G)
PART 2-CHILDREN 110 ANNOTATIONS FOR FAILURE TO THRIVE – LEVEL 2 CHILDREN
A: To assess, as precisely as possible, the caloric intake habits and schedules, breast-feeding etc. should be described by the mother in detail. The mother should tell exactly what the child is taking and how much and how often per day.
B: Give exact advise to the mother on the schedule and content of the diet: breast-feeding weaning foods and other foods. If possible let the mother record exactly what the child takes an any problems she may come across. The dietary trial should be evaluated after 7 days. If possible a home visit should be carried out to assess the availability of resources at home.
C: Improvement is defined as weight gain with an increased alertness of the child, or loss of oedema (which may result in initial weight loss before weight gain!).
D: These investigations may help identify causes of failure to thrive that should be treated immediately.
E: If no specific diagnosis has been made, it may be possible to admit the child for a trial of naso-gastic feeding, especially when a previous home dietary trial did not result in improvement of the child.
F: If the child is not improving and in first instances no underlying cause has been established, admission for further evaluation may be necessary: investigations for endocrine disorders, renal failures, CNS disease and chronic infections need to be considered.
G: Many HIV infected children show failure to thrive without identifiable cause or feeding error and despite adequate caloric intake. This is thought to be due to HIV itself.
PART 2-CHILDREN 111 II.24 LYMPHADENOPATHY – LEVEL 1 CHILDREN
LYMPHADENOPATHY (A)
Any local or regional YES infection which might Treat explain as indicated lymphadenopathy?
NO
Any of the following present fever weight loss YES unilateral nodes increasing in size matted nodes fluctuant nodes Minimal tenderness (B)
NO
HIV related Persistent Generalised Lymphadenopathy (C)
Refer to level 2 Follow-up as indicated
PART 2-CHILDREN 112 ANNOTATIONS FOR GENERALISED LYMPHADENOPATHY CHILDREN
A: Definition Lymphadenopathy may be localised or generalised. It is important to identify the possible underlying causes of localised lymphadenopathy, in order to give appropriate treatment. Usually, local lymphadenopathy, affecting only 1 or 2 regions and is caused by a local infection. Sometimes it may be due to TB or lymphoma.
Persistent Generalised lymphadenopathy (PGL) is a non-specific finding which is very common in children with HIV infection. PGL in HIV infected children is defined as:
1. Lymph nodes measuring at least 0.5 cm 2. Present in 2 or more sites, with bilateral lymph nodes counting as 1 site. 3. Duration of more than 1 month 4. No local infection that might explain the lymphadenopathy
This
Aetiology Possible causes of lymphadenopathy in HIV infected children:
1. HIV infection itself
2. Infections : Bacterial Tuberculosis Fungal Cryptococcosis Histoplasmosis Protozoal Toxoplasmosis
3. HIV associated cancers Lymphomas
4. Dermatological conditions Seborrhoeic dermatitis Chronic pyoderma
B: Further evaluation is required in case: 1. Unilateral nodes are increasing in size 2. The nodes are matted 3. The nodes are becoming fluctuant 4. The nodes show signs of inflammation, e.g. are hot and tender
In these cases lymph node biopsy is indicated and treatment depends on the findings. In case of tuberculosis, TB treatment should be started.
C: PGL in HIV-infected children is mostly due to the normal immune reaction to HIV infection. If no other problems are identified, no additional investigation or treatment is required. Lymph nodes usually disappear as the immuno- suppression advances and opportunistic infections appear.
PART 2-CHILDREN 113 II.25 HIV INFECTIONS AND BREASTFEEDING
Transmission of HIV from infected mother to their infants may occur before, during or shortly after birth. About one third of the children born from HIV infected mothers will be HIV infected (see page 88).
Breast milk of infected mothers may contain HIV and breast milk can be a source of HIV infection. The transmission rate due to breastfeeding is estimated at 3% to 6% per year2324. Transmission rates are therefore higher if the breastfeeding period is longer. HIV transmission is also higher if the mother has mastitis. If the mother is infected before birth or in the postpartum period, the HIV transmission rate through breastfeeding is also higher.
Children who receive mixed feeding seem to have a higher risk of HIV infection during the first months of life than children who receive exclusive breastfeeding or exclusive artificial feeding.
Shortening the period of breastfeeding may therefore reduce the risk of HIV transmission and mixed feeding should be discouraged. The alternative of giving exclusively artificial feeding has also considerable risks. Studies in other African countries indicate that children without HIV infection receiving artificial feeding have 2.5 to 5 times more risk of dying from any cause before the age of 12 months than breast fed infants.
In addition, the immunological, nutritional, psychosocial and child-spacing benefits of breast-feeding are well recognised. Breast milk is also important to preventing infections, which could accelerate progression of HIV-related diseases in already infected infants.
Taking all these factors into account, exclusive breast-feeding for the first 6 months in life is continued to be generally promoted and supported, as for the majority of mothers the sero-status is unknown and for most children the benefits of exclusive breastfeeding outweigh the risks, regardless of the HIV status.
The final choice about the method of feeding, however, is made by the mother. Whatever this choice may be, health staff should provide support to ensure optimal nutrition of mother and child.
PART 2-CHILDREN 114 II.26 HIV INFECTION AND IMMUNIZATION
Data from several studies have shown that the benefits of immunisation outweigh the low risk of adverse effects of these vaccines, even in the presence of symptomatic HIV infection.
The only vaccine with a certain risk of complication is BCG, if given to children who have symptomatic HIV infection. As BCG is normally given immediately or shortly after birth, when children are usually not yet symptomatic, this does not have any practical consequences.
Table 18 Immunisation in HIV infected children and adults
Vaccine Asymptomatic Symptomatic HIV infection HIV infection
Infants BCG yes no
DPT yes yes
Polio yes yes
Measles yes yes
Adults Tetanus toxoid yes yes
PART 2-CHILDREN 115 II.27 PALLIATIVE CARE CHILDREN
Palliative care may be needed from infancy and for many years for some children, while others may not need it until they are older and only for a short time. Also the transition between aggressive treatments to cure or prolong good quality life and palliative care may not be clear—both approaches may be needed in conjunction, each becoming dominant at different times.
Child development An intrinsic aspect of childhood is children's continuing physical, emotional, and cognitive development. This influences all aspects of their care, from pharmacodynamics and pharmacokinetics of drugs to their communication skills and their understanding of their disease and death.
Care at home Most children with a life limiting disease are cared for at home. Parents are both part of the team caring for the sick child and part of the family and needing care themselves. As their child's primary carers, they must be included fully in the care team— provided with information, able to negotiate treatment plans, taught appropriate skills, and assured that advice and support is accessible 24 hours a day.
Assessing symptoms Assessing symptoms is an essential step in developing a plan of management. Often a picture must be built up through discussion with the child, if possible, combined with careful observations by parents and staff. It is also important to consider the contribution of psychological and social factors for a child and family and to inquire about their coping strategies, relevant past experiences, and their levels of anxiety and emotional distress.
Managing symptoms Many of the symptoms that children suffer and the approaches to relieving them have not been studied formally. Until definitive information becomes available, treatment is often based on clinical experience and adapted from general paediatric practice and palliative care of adults.
Children often find it difficult to take large amounts of drugs, and complex regimens may not be possible. Doses should be calculated according to a child's weight. Oral drugs should be used if possible, and children should be offered the choice between tablets, whole or crushed, and liquids. Long acting preparations are helpful, reducing the number of tablets needed and simplifying care at home. If an alternative route is needed some children find rectal drugs acceptable; they can be particularly useful in the last few days of life. Otherwise, a subcutaneous infusion can be established
Pain The myths perpetuating the under treatment of pain in children have now been rejected. However, most doctors lack experience in using strong opioids in children, which often results in excess caution. The three-step ladder of analgesia, as described for adults, is equally relevant for children, with Paracetamol, Dihydrocodeine, and morphine sulphate forming the standard steps.
Opioids—Children with HIV rarely need antiemetics and laxatives. Itching with opioids in the first few days is quite common and responds to antihistamines if PART 2-CHILDREN 116 necessary. Many children are sleepy initially, and parents should be warned of this lest they fear that their child's disease has suddenly progressed. Respiratory depression with strong morphine is not a problem in children over 1 year old if treatment is started in standard doses and thereafter increased or reduced according to needs. In younger children starting doses should be reduced.
Table 19Doses of Analgesic Drugs in Children
Paracetamol Oral dose 15 mg/kg every 4-6 hours Rectal dose 20 mg/kg every 6 hours Maximum dose 90 mg/kg/24 hours, 60 mg/kg/24 hours in neonates Dihydrocodeine Ages <4 years 500 µg/kg orally every 4-6 hours Ages 4-12 years 500-1000 µg/kg orally every 4-6 hours Morphine Standard starting doses Ages <1 year 150 µg/kg orally every 4 hours Ages 1-12 years 200-400 µg/kg orally every 4 hours Ages >12 years 10-15 mg orally every 4 hours Titrate according to analgesic effect
Adjuvant analgesics—Non-steroidal anti-inflammatory drugs (Aspirin, Ibuprofen) may be helpful for musculoskeletal pains but caution is needed in children with HIV because infiltration of the bone marrow may lead to increased risk of bleeding. Neuropathic pain may be helped by antiepileptic and antidepressant drugs. Pain from muscle spasms can be a major problem for children with neurodegenerative diseases and may be helped by benzodiazepines. Headaches from raised intracranial pressure associated with brain tumours are best managed with gradually increasing analgesics. Corticosteroids should be avoided due to the considerable side effects in children.
Feeding Being unable to nourish their child causes parents great distress and often makes them feel that they are failing as parents. Sucking and eating are part of children's development and provide comfort, pleasure, and stimulation. These aspects should be considered alongside a child's medical and practical problems with eating.
Nausea and vomiting These are common problems. Antiemetics (Metoclopropamide, Haloperidol) can be used to relief symptoms.
PART 2-CHILDREN 117 Support for the family Families need support from the time of diagnosis and throughout treatment as well as when the disease is far advanced. Professionals must be flexible in their efforts to help. Each family and individual within a family is unique, with different strengths and coping skills. The needs of sibling and grandparents should be included.
Figure 5: Faces scale used to measure pain effect in children
PART 2-CHILDREN 118 II.28 FOLLOW - UP CHILDREN
The Road-to-Health chart is the most valuable tool for monitoring of the wellbeing of the exposed or infected infant. Failure to maintain growth is suggestive of progressive HIV infection or superimposed infection such as TB.
CD4 percentages are a valuable tool to monitor the wellbeing of infected children and guide decisions regarding PCP prophylaxis and Antiretroviral treatment. A CD4 count of <15% should be considered equivalent to the adult CD4 count of <200/ml
Asymptomatic HIV infection
All exposed infants should be seen at the age of 4-6 weeks of age.
Asymptomatic exposed children should maintain their normal schedules of immunisations. They should be seen as least every 3 months until the age of 2 years and every 6 months after this age, to monitor their condition, and as indicated if symptoms intervene. History and physical examination should be done at all levels and are essential for classifying the patient as asymptomatic, and for detecting the onset of disease.
1. History – assess presence of HIV symptoms including: Fever Poor feeding / failure to thrive Diarrhoea Thrush Recurrent infections Cough, dyspnoea, tachypnoea Sweating Swollen lymph nodes or parotitis Developmental abnormalities and other neurological symptoms
2. Physical examination General: temperature, weight Skin: herpes zoster, herpes simplex, folliculitis, prurigo, Candida diaper dermatitis, seborrhoeic dermatitis, condyloma, molluscum Eye: retinitis, perivasculitis Ears: nose throat: otitis, rhinitis, thrush, gingivitis, sinusitis, parotitis Heart: pulse, rhythm Chest: respiratory tract infection Abdomen: distension, hepatomegaly splenomegaly Neurologic: developmental milestones, intellectual ability, head circumference, motor abnormalities, tone Extremities: clubbing
PART 2-CHILDREN 119 Symptomatic HIV disease
Symptomatic HIV infected children need to be seen more frequently, depending on their clinical condition. In general it can be recommended to see these children monthly to evaluate the present clinical state and to determine whether new complaints have developed. It is important to evaluate the nutritional state of the children during these follow up visits. If the child has serious problems weekly or 2 weekly follow up may be needed. In any case the child should be reviewed at the end of any course of treatment this may be, to evaluate the effect of the treatment.
Supportive and prophylactic treatment
Supportive and prophylactic treatment is given to all immuno-compromised children to reduce the risk of opportunistic infections and improve quality of life. These treatments should be continued as long as they are tolerated.
1. Vitamins
Vitamin A deficiency is common and predisposes children to infections. Supplementation with Vitamin A has been shown to result in significant short- term improvement in immune function and reduced morbidity, particularly in relation to diarrhoeal disease.
A single dose of Vitamin A supplement is recommended on a six monthly basis:
Table 20: Recommended doses of Vitamin A Age Vitamin A dosage
Under 6 months 50,000 IU
6 to 12 months 100,000 IU
1 year and older 200,000 IU
In addition, a daily dosage of a multivitamin preparation should be prescribed.
PART 2-CHILDREN 120 2. PCP prophylaxis
PCP prophylaxis is recommended for all exposed children in the first year of life, from the age of 6 weeks. From the age 1 year prophylaxis can be discontinued if the HIV test of the child is negative. From the age of 18 months, when a definite serological diagnosis of HIV infection is made, prophylaxis is reserved for symptomatic children and asymptomatic children with CD4<15% should receive.
Recommended doses are as follows:
Table 22:Recommended doses of co-trimoxazole for PCP prophylaxis Age Co-trimoxazole dosage Six weeks to five months 2.5 ml once daily on Mondays, Wednesdays and Fridays Six months to six years 5 ml once daily on Mondays, Wednesdays and Fridays Six years and older 10 ml or 1 tablet once daily on Mondays, Wednesdays and Fridays
3. Anaemia
If dietary iron and folic acid intake may be insufficient, give 1 mg/kg elementary iron per day (for example Fe gluconate) Folate 2.5 mg weekly
4. Helminth infections
Albendazole should be given from the age of 6 months at the following dosis: if weight <10kg 200mg stat (10ml of suspension of 20 mg/ml) if weight >10kg 400mg stat (2 tablets of 200mg)
5. Tuberculosis
In all children who have had contact with sputum positive TB patients (especially those under 2 years), and those who are tuberculin reactors (Mantoux >5mm or Tine test Grade 2) supervised TB prophylaxis with INH should be considered, once active disease has been excluded. The regimen depends on the weight of the child:
Table 22: TB prophylaxis in HIV infected children Weight Dosage of INH 5-10 kg 50 mg 11-20 kg 100 mg 21-30 kg 200 mg
Pyridoxine 25 mg per day should be added to the prophylaxis due to the high frequency of HIV associated peripheral neuropathy.
PART 2-CHILDREN 121 II.29 ANTIRETROVIRAL TREATMENT CHILDREN
General Considerations Although the pathogenesis of HIV infection and the general virologic and immunologic principles underlying the use of antiretroviral therapy are similar for all HIV-infected persons, there are unique considerations needed for HIV-infected infants, children, and adolescents.
Perinatal HIV infection occurs during the development of the infant's immune system; thus, both the clinical manifestations of HIV infection and the course of immunologic and virologic markers of infection differ from those for adults. Drug pharmacokinetics change during the transition from the newborn period to adulthood, requiring specific evaluation of drug dosing and toxicity in infants and children. Finally, optimizing adherence to therapy in children and adolescents requires specific considerations.
Antiretroviral therapy has provided substantial clinical benefit to HIV-infected children with immunologic or clinical symptoms of HIV infection. Trials of symptomatic children have demonstrated that highly effective antiretroviral treatment (HAART) with three drugs is virologically and immunologically superior and delays development of resistance.
The following concepts were considered in the formulation of these guidelines: Identification of HIV-infected women before or during pregnancy is critical to providing optimal therapy for both infected women and their children and to preventing perinatal transmission. Therefore, voluntary prenatal HIV counseling and testing should be made widely available and access to these services should be promoted. Enrollment of pregnant HIV-infected women; their HIV-exposed newborns; and infected infants, children, and adolescents into clinical studies offers the best means of determining safe and effective therapies. All antiretroviral drugs approved for treatment of HIV infection may be used for children when indicated -- irrespective of labeling notations. Effective management of the complex and diverse needs of HIV-infected infants, children, adolescents, and their families requires a multidisciplinary team approach that includes experienced physicians, nurses, counsellors, social workers, outreach workers, and pharmacists. Determination of HIV RNA copy number and CD4+ T-lymphocyte levels is essential for monitoring and modifying antiretroviral treatment in infected children and adolescents as well as adults. The following factors influencing adherence to therapy should be considered: a) availability and taste of pediatric formulations; b) impact of the medication schedule on quality of life, c) ability of the child's caregiver or the adolescent to administer complex drug regimens and d) potential for drug interactions. Monitoring growth and development is essential for the care of HIV-infected children. Growth failure and developmental deterioration may be specific manifestations of HIV infection in children. Nutritional-support therapy is an intervention that affects immune function, quality of life, and bioactivity of antiretroviral drugs.
PART 2-CHILDREN 122 When to Initiate Therapy
Antiretroviral therapy is recommended for HIV-infected children with clinical symptoms of HIV infection (i.e., those in clinical categories A, B, or C) or Evidence of immune suppression (i.e., those in immune categories 2 or 3) regardless of the age of the child or viral load Ideally, antiretroviral therapy should be initiated in all HIV-infected infants aged <12 months as soon as a confirmed diagnosis is established (by PCR RNA testing)-- regardless of clinical or immunologic status or viral load.
Treatment in asymptomatic children aged >1 year with normal immune status may be deferred. Factors to be considered in deciding when to initiate therapy include: a) high or increasing HIV RNA levels, b) rapidly declining CD4+ T-lymphocyte number or percentage or c) development of clinical symptoms.
Choice of Initial Antiretroviral Therapy Combination therapy is recommended for all infants, children, and adolescents who are treated with antiretroviral agents. The preferred regimen is combination therapy with two NRTIs and one protease inhibitor or a non-nucleoside nuclease inhibitor (such as efavirenz). New antiretroviral drugs and combinations are being studied in infected adults and children.
When to Change Antiretroviral Therapy The following three reasons warrant a change in antiretroviral therapy: a) failure of the current regimen with evidence of disease progression based on virologic, immunologic, or clinical parameters; b) toxicity or intolerance to the current regimen; and c) new data demonstrating that a drug or regimen is superior to the current regimen. Intensive family education, training in the administration of prescribed medications, and discussion of the importance of adherence to the drug regimen should be completed before initiation of new treatment.
Cost of Antiretroviral treatment The monthly drug cost of HAART regimes at Namibian wholesaler prices for treatment of a child of 10 kg with syrup varies between N$ 989 (for NVP+AZT+ddI) 1,063 (for NVP+d4T+3TC). The monthly drug costs for treatment of a child of 20 kg with tablets varies between 1,088 (for EFV+ddI+AZT) and N$ 1,322 (for NVP+d4T+3TC). Drug costs may be reduced considerably by negotiating preferrential pricing with major drug companies or by purchasing Antiretroviral drugs from alternative sources. According to information forwarded by an alternative supplier, drug costs for treatment of a child of 20 kg with NEV+3TC+d4T would be around N$ 700 per month.
PART 2-CHILDREN 123 BIBLIOGRAPHY
ABC of AIDS, Edited by Michael Adler, Published by the British Medical Association, London, UK, 1997, ISBN 0-7279-1137-6
ABC of palliative care, Edited by Marie Fallon and Bill O'Neil, Published by the British Medical Association, London, UK, 1997, ISBN 0-7279-0793
Medical Management of HIV infection by John G. Berlett. The John Hopkins University Division of Infectious Diseases, 1998
The Medical Management of AIDS, Edited by M.A. Sande and P.A. Volberding, W.B. Sauners company Second Edition 1990. ISBN 0-7216-3505-9
Primary AIDS care, Edited by Dr. Clive Evian , Jacana Education Hougton South Africa. ISBN 1-874955-21-2
National Tuberculosis control programme (NCTB), Policy document, Ministry of Health and Social Services, Republic of Namibia.
National AIDS Control programme. Guideline for the syndromic management of sexually transmitted diseases.
PART 2-CHILDREN 124 USEFUL WEBSITES http://hopkins-aids.edu/publications/ This sites contains the full updated version of the reference book: Medical Management of HIV infection by John G. Bartlett This book serves as the standard of care for the Johns Hopkins AIDS Service and has been accepted as the standard of care for quality assurance by Maryland Medicaid. http://www.hivatis.org/ The HIV/AIDS Treatment Information Service (ATIS) is the central resource for US federally-approved treatment guidelines for HIV and AIDS.
Guidelines for
To complete: Dose of Fluconazole for Cryptococcus Meningitis p 61/66
PART 2-CHILDREN 125 REFERENCES
PART 2-CHILDREN 126 1 Bartlett JG, Moore RD. Improving HIV therapy, Scientific American 1998; 798: 2 Feinberg MB, Changing the natural history of HIV disease. Lancet 1996: 348: 239-46. 3 Paromycin treatment for crytosporidia. Am J Med 1996;100:370 4 Doumbo O, Rossignol JF, Pichard E, Traore HA et al, Nitazoxanide in the treatment of cryptosporidial diarrhea and other parasitic infections associated with acquired immunodeficiency syndrome in tropical Africa. Am J Trop Med Hyg. 1997;56(6):637-9 5 JAIDS 1995;8:345 6 Wiktor SZ, Sassan-Morokro M, et al. Efficacy of trimethoprim-sulphametoxazole prophylaxis to decrease morbidity and mortality in HIV-1 infected patients with tuberculosis in Abidjan, Cote d'Ivoire: a randomised controlled trial. Lancet 1999;353: 1469-75 7 Heydermann RS, Gangaidzo IT, Haikom JG, Mielke J et al, Cryptococcal meningitis in human immunodeficiency virus infected patients in Harare, Clin. Infect. Dis. 1998;26: 284-9. 8 De Cock KM, Grant A, Porter DH, Preventive therapy for tuberculosis in HIV infected persons: international recommendations, research and practice. Lancet 1995;345: 833-836. 9 Mellors JW, Rinaldo C, Gupta CR, White RM, et al. Prognosis in HIV-1 infection predicted by the quantity of virus in plasma. Science 1996; 272: 1167-70 10 Rhone SA, Hogg RS, Yip B, et al. Do dual nucleoside regimes have a role in the era of vial load driven antiretroviral therapy? J Infect. Dis 1998;178: 662-68. 11 Palella FJ, Delaney KM, Moorman AC, Loveless MO,et al. Declining morbidity and mortality among patients with advanced Human Immunodeficiency Virus infection. N Eng J Med1998; 338:853-860 12 Egger M, Hirschel B, Francoli P, Sudre P. Impact of new antiretroviral combination therapies in HIV infected patients in Switzerland: prospective multicentre study. BMJ 1997;315: 1194-1199. 13 Hirchel B, Francioli P, Progress and problems in the fight against AIDS. Editirial N Eng J Med 1998; 338: 906-908. 14 Montaner JSG, Hogg R, Raboud J, Harrigan R, et al. Antiretroviral treatment in 1998. Lancet 1998; 352: 1919-22 15 Eldred LJ, Wu AW, Chaisson RE, Moore RD. Adherence to antiretroviral therapy and pneumocystis prophylaxis in HIV disease. J Acquir Immune Defic Syndr Hum Retrovirol 1998; 18(2): 117-125 16 Montaner J, Mellors M. Progress in HIV-1 therapy continues on an upward track. Lancet 1999: 353; 565. 17 Zhang H, Dornadula G, Beumont M, Livornese L, et al. Human Immunodeficiency Virus type 1 in the semen of men receiving highly active antiretroviral therapy. N Eng J Med 1998; 339; 1803-1809 18 De Cock KM, Guidelines for managing HIV infection, Editorials BMJ 1997;315: 1-2 19 The Working Group on Mother-To-Child Transmission of HIV. Rates of Mother-to-Child Transmission of HIV-1 in Africa, America and Europe: Results from 13 Perinatal Studies. Journal of Acquired Immune Deficiency Syndromes and Human Retrovirology; 8:506-510. 20 Dabis F, Msellati P, Newell ML, Halsey N. Methodology of intervention trials to reduce mother to child transmission of HIV with special reference to developing countries. AIDS, 1995; 9: S67-S74. 21 Leroy V, Newell ML, Dabis F, Peckham C, et al. International multicentre pooled analysis of late postnatal mother-to-child transmission of HIV-1 infection. Lancet; 1998; 352:597-600. 22 Burns DN, Mofenson LM, Paediatric HIV-1 infection. Lancet 1999; 354(suppl II): 1-6 23 Leroy V, Newell ML, Dabis F, Peckham C, et al. International multicentre pooled analysis of late postnatal mother-to-child transmission of HIV-1 infection. Lancet; 1998; 352:597-600. 24 JAMA 1999;282:744