Guinea Ebola Response Plan I: End of Project Report November 17, 2014–August 16, 2015
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Région De Kindia 2018
REPUBLIQUE DE GUINEE Travail - Justice- Solidarité MINISTERE DU PLAN ET DU DEVELOPPEMENT ECONOMIQUE La région de Kindia en chiffres Edition 2020 GEOGRAPHIE ET ORGANISATION ADMINISTRATIVE Géographie 0rganisation administrative en 2018 5 préfectures ; 41 sous-préfectures ; 5 communes urbaines, Superficie = 28 875 km2 627 quartiers/districts ; 2 424 secteurs 40 communes rurales Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) Préfectures Sous-préfectures Bangouyah, Damankanyah, Friguiagbé, Kolente, Lisan, Madina Oula, Mambiya, Molota, Kindia Samayah, Sougueta Coyah Kouriya, Manéah, Wonkifong, Dubréka Badi, Falessade, Khorira, Ouassou, Tanènè, Tondon, Forécariah Alassoya, Benty, Farmoriah, Kaback, Kakossa, Kallia, Maferenya, Moussaya, Sikhourou Bourouwal, Daramagnaky, Gououdje, Koba, Kollet, Kosotamy, Missira, Santou, Sarekaly, Sinta, Télimélé Sogolon, Tarihoye, Thionthian Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) STATISTIQUES DEMOGRAPHIQUES Populations des RGPH 1983 1996 2014 Population région de Kindia 555 937 928 312 1 561 336 Population de la principale préfecture : Kindia 163 032 287 611 439 614 Part de la population nationale en 2014 : 14.8 % Rang régional en 2014 : 4/8 Sources : Institut national de la statistique/RGPH Population au 1er juillet 2015 2016 2017 2018 Population région Kindia 1 620 881 1 667 695 1 715 504 1 764 268 Sources : Institut national de la statistique (Perspectives démographiques de -

Rapport De La Situation Epidémiologique De La Maladie À Virus Ebola Dans La Préfecture De FORECARIAH Situation Au 28 Mai 2015 a 18H I- SOMMAIRE
onfirmé Rapport de la Situation Epidémiologique de la Maladie à Virus Ebola dans la préfecture de FORECARIAH Situation au 28 Mai 2015 A 18H I- SOMMAIRE: Situation des cas : 02 nouveaux cas confirmés ont été enregistrés ce jour dont 1 dans le village de Sinki S/P de Moussayah et 1 dans le village de Bokariah S/P de Kalliah, tous contacts connus et suivis, appartenant à la chaine de transmission de Yaworiah / S/P Moussayah; 15 alertes ont été enregistrées dont : 06 suspects parmi lesquels, il y a 3 contacts connus et suivis ; 09 décès communautaires tous prélevés, enterrés de façon digne et sécurisée ; 08 nouveaux échantillons ont été examinés par le laboratoire de Forecariah dont 2 positifs; 11 malades sont actuellement hospitalisés au CTE de Forecariah dont 3 confirmé et 8 suspects ; 08 cas confirmés ont été notifiés durant les 7 derniers jours dans 4 Sous-préfectures sur 10 à savoir, Moussayah (4 cas), Kalliah (2 cas), Sikhourou (1 cas) et Farmoriah (1cas). Situation des contacts : 1017 contacts sur 1028 ont été vus soit un taux de suivi de 99,92%; 11 contacts n’ont pas été vus ce jour parmi lesquels 2 sont partis à Conakry pour des raisons de commerce, 4 de la S/P Maferinyah (dont 3 qui sont réticents au suivi et 1 des 6 contacts interpelés qui a fuit pour une localité non encore connue par les agents du suivi), 1 de la S/P de Farmoriah (parti à Coyah) et 4 de la sous-préfecture de Moussayah ayant fait des déplacements internes. -

Forecariah Kindia Coyah Conakry
Infrastructures de Santé de la Préfecture de Forecariah au 26 Octobre 2015 Guinea : Sogoroyah GBereire Gombokhori_Centre Wariya Kindia Khambiyah Wanindara Kalmata Alayiyah Kafera Coyah Moribayah Kanfounyah ± Tinekhoure Katafo Kondekhourou Yakhamodiyah Timbirin Khoundinde Moungoutouniyah Bambayah Dambata Yeralande Kolotoyah Lasiria Tandonya Conakry Wondima Kamalabo Nissikhoure Sarayah TABAN CENTRE Sikhourou Campama Madina Kilimou Samayah PS Sikhourou BONFET CENTRE Soriyayah PS Walia Neriboun Farabanna Sansanyi Samayah PS Moribaya Tamouyah Teguefili Yimbonyah Garayah Fansiga Gbomilo Kenende Bofoudiyah Kouliyire Filidonke Kabaya_Khourekhore Komboya PS Dafira Dembayah Salifouyah Fori Tolomaya Garasoriyah SAFEYA CENTRE Kolakhoure Salifouyah Nene Daoudayah Kolongaya Silia Kaposse Kimara Wondima Siliya Saanya Noumoukhoure Khimbely Salifouyah Filide Siafou Seriyah GCS Mafrinyah Salia Wondeta Koronboya Moukhouragbe Maferenya Amaraya Tonokhoure FEINDEMODIA CENTRE Kanda Tanene Moukhourady Salguidia Sabakhoure PS Degui-Degui Terrain Sirakhataya Yoroya Fayimbaya CS Bassia G Khouregueli Fanyeyire PS Koket Mambiyah2 Souleymania Lamana Ps de feindemodiya Fodemomoyah Wonkifon Madina Sambalia Sansanyi Tougande Barekhoure PS Fandie Kondekhoure Sourima Khabousoriya Kondeyire Yalague DAARY CENTRE Bendougou Laminaya Kenende Khalimale PS Kamalayah Tafedy Layah Fokoufokou Koniakhori PS Dandayah PS Soriwoula Kounde Sourikhouli Fossy Sagoyah Soriwoula Carrefour Kolakhoure Dembayah Memalayah Khourekhori Korebounyi Soriya Bembenyi Khouredi Dalaba Gbangba Allassoyah -

Guinea : Reference Map of N’Zérékoré Region (As of 17 Fev 2015)
Guinea : Reference Map of N’Zérékoré Region (as of 17 Fev 2015) Banian SENEGAL Albadariah Mamouroudou MALI Djimissala Kobala Centre GUINEA-BISSAU Mognoumadou Morifindou GUINEA Karala Sangardo Linko Sessè Baladou Hérémakono Tininkoro Sirana De Beyla Manfran Silakoro Samala Soromaya Gbodou Sokowoulendou Kabadou Kankoro Tanantou Kerouane Koffra Bokodou Togobala Centre Gbangbadou Koroukorono Korobikoro Koro Benbèya Centre Gbenkoro SIERRA LEONE Kobikoro Firawa Sassèdou Korokoro Frawanidou Sokourala Vassiadou Waro Samarami Worocia Bakokoro Boukorodou Kamala Fassousso Kissidougou Banankoro Bablaro Bagnala Sananko Sorola Famorodou Fermessadou Pompo Damaro Koumandou Samana Deila Diassodou Mangbala Nerewa LIBERIA Beindou Kalidou Fassianso Vaboudou Binemoridou Faïdou Yaradou Bonin Melikonbo Banama Thièwa DjénédouKivia Feredou Yombiro M'Balia Gonkoroma Kemosso Tombadou Bardou Gberékan Sabouya Tèrèdou Bokoni Bolnin Boninfé Soumanso Beindou Bondodou Sasadou Mama Koussankoro Filadou Gnagbèdou Douala Sincy Faréma Sogboro Kobiramadou Nyadou Tinah Sibiribaro Ouyé Allamadou Fouala Regional Capital Bolodou Béindou Touradala Koïko Daway Fodou 1 Dandou Baïdou 1 Kayla Kama Sagnola Dabadou Blassana Kamian Laye Kondiadou Tignèko Kovila Komende Kassadou Solomana Bengoua Poveni Malla Angola Sokodou Niansoumandou Diani District Capital Kokouma Nongoa Koïko Frandou Sinko Ferela Bolodou Famoîla Mandou Moya Koya Nafadji Domba Koberno Mano Kama Baïzéa Vassala Madina Sèmèkoura Bagbé Yendemillimo Kambadou Mohomè Foomè Sondou Diaboîdou Malondou Dabadou Otol Beindou Koindou -
PRSP II) for Guinea and the Public Disclosure Authorized Joint IDA-IMF Staff Advisory Note (JSAN) on the PRSP II
OFFICIAL USE ONLY IDA/SecM2007-0684 December 12, 2007 Public Disclosure Authorized For meeting of Board: Tuesday, January 8, 2008 FROM: Vice President and Corporate Secretary Guinea: Second Poverty Reduction Strategy Paper and Joint IDA-IMF Staff Advisory Note 1. Attached is the Second Poverty Reduction Strategy Paper (PRSP II) for Guinea and the Public Disclosure Authorized Joint IDA-IMF Staff Advisory Note (JSAN) on the PRSP II. The IMF is currently scheduled to discuss this document on December 21, 2007. 2. The PRSP II was prepared by the Government of Guinea. The paper acknowledges the disappointing outcome of the first PRSP, which covered the period 2002-2006. The political, social and economic environment in which the implementation of PRSP I took place was characterized by poor governance, political instability, and low growth which led to an increase in poverty from 49 percent in 2002 to an estimated 54 percent in 2005. Overall, public service delivery deteriorated in terms of both quality and access and the living conditions for most Guineans worsened. Public Disclosure Authorized 3. PRSP II aims at recapturing lost ground over the past five years. The overall strategy is based on three pillars: (i) improving governance; (ii) accelerating growth and increasing employment opportunities; and (iii) improving access to basic services. It focuses on restoring macroeconomic stability, institutional and structural reforms, and mechanisms to strengthen the democratic process implementation capacity. 4. As approved by the Board on August 6, 2007, the pilot Board Technical Questions and Answer Database (http://boardqa.worldbank.org or from the EDs' portal) is now open for questions. -

IOM Guinea Ebola Response Situation Report, 8-31 March 2016
GUINEA EBOLA RESPONSE INTERNATIONAL ORGANIZATION FOR MIGRATION RAPPORT DE SITUATION From 8 to 31, March 2016 News Launching of the “soft ring containment” of Koropara sub-prefecture. © IOM Guinea 2016 On February 29 and March 17, three On March 9, 2016, IOM organized a From March 9 to 11, 2016, a joint IOM-RTI- people died in the sub-prefecture of ceremony during which, it officially handed- DPS mission went to different sub- Koropara following an unknown disease over the health post of Kamakouloun to sub- prefectures of Boffa for a maiden contact characterized by fever, deep emaciation, prefectural authorities of Kamsar, prefecture with local authorities. The aim was to explain diarrhea including vomiting of blood. A few of Boke. The health facility was rehabilitated the criteria used in the selection of CHA days later, two other people developed the and fully equipped by the organization. (Community Health Assistants), validating the same symptoms. The tests, carried out on list of CHA provided by the DPS in their March 17, were positive to the Ebola Virus localities and selecting 30 participants for the Disease, indicating the resurgence of the participatory mapping exercise (10 wise men, disease in Guinea, nearly three months after 10 youths and 10 women). it was officially declared over by WHO. Situation of the Ebola virus disease after its resurgence in Guinea In the sub-prefecture of Koropara, located at 97km from the city of NZerekore, an approximately 50-year-old farmer along with his two wives died between February 29 and March 17, 2016 following an unknown disease characterized by fever, deep emaciation, diarrhea and vomiting of blood. -
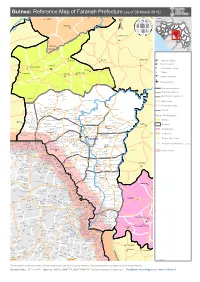
Guinea: Reference Map of Faranah Prefecture (As of 05 March 2015)
Guinea: Reference Map of Faranah Prefecture (as of 05 March 2015) Kalinko SENEGAL MALI GUINEA Sélouma BISSAU GUINEA Komola Koura COTE D'IVOIRE SIERRA LEONE Dialakoro Kankama LIBERIA Sisséla Sanguiana Bissikirima Regional Capital District Capital Dabola Arfamoussayah Sub District Capital Banko Kounendou Village Dogomet N'demba Unpaved runway Paved runway Region boundaries Koulambo District boundaries Morigbeya Dar Es Salam Daro Gada Walan Sub District boundaries Kindoyé DIGUILA CENTRE Fabouya TOUMANIA CENTRE Boubouya Main roads Yombo Nialen Moria Dansoya Secondary roads NIENOUYA CENTRE Teliayaga Doukou Passaya Souriya Mansira Moribaya KONDEBOU KASSA BOUNA CENTRE Tambaya Rivers Foya Gadha Mongoli Babakadia Hafia Gomboya BELEYA CENTRE SABERE KALIA Keema SOUNGBANYA CENTRE Balandou Beindougou SANSANKO CENTRE Sidakoro Gueagbely Gueafari Sokora District (Préfectures) Harounaya Miniandala Badhi Gnentin Oussouya Banire Wolofouga Lamiya Gueagbely Mameyire SANSAMBOU CENTRE BIRISSA CENTRE NGUENEYA CENTRE NIAKO CENTRE Koumandi Koura Dabola Wassakaria Kobalen Bingal Dansoya Tomata Konkofaya Heredou Marela karimbou Sansamba Bouran SOLOYA CENTRE Kolmatamba KOUMANDI KORO Sanamoussaya MILIDALA CENTRE Banfele Labatara Gninantamba BONTALA Koura Sambouya DIANA CENTRE Sansando Faranah Wossekalia FRIGUIA CENTRE MAGNA Halossagoya KALIA CENTRE I KOMBONYA Ballayany Herewa Alia Filly Fore Sakoromaya SOLONYEREYA Khamaya Bindou Dansaya Koutamodiya Salia Kamako Kissidougou Goulouya Fantoumaniya Nerekoro SEREKORO CENTRE Guidonya Kombonyady Wassambala Balankhamba Kabaya -

Guinea : Reference Map of Kankan Region (As of 3 March 2015)
Guinea : Reference Map of Kankan Region (as of 3 March 2015) Bankolen Mambifagalena Niagassola Kry Tourelen Berlen Sokoromansa Magadiano Faraboloni Linkekoro KIGNEKOUROU CENTRE Bouyido Malsadou Seourou Konfara 2 Gnembou Tanssa Magnaka KOTE CENTRE Balenda SOUMBARAYA CENTRE Kourelen TALABE CENTRE Dialawassa II Kondoko Djanwely Itipony Dougounta Dora Kourakoda DIBIA CENTRE Djinko Ilimalo Naboun Kanimbakalako Kodougoulen KAKAMA CENTRE Tondo Komagron Kayaga Kignedi Sininko Kadabili Kignero Gnere Sininkoro Badamako Kounsounkoro Yirikelèma Kanikoumbaya SOKORO CENTRE DIATEA CENTRE Dita Salla Tondji1 Koda Kebesabaya Siguirini Sakounou Malea Bembéta Megnèkoma Silabado Diakan Toukönö BOULAN CENTRE Gbèdela MANKADIAN CENTRE Gbörökola Doko Tombani Maragbè Kana Sékela Mansadji Sidao Tonso Banankölö Tomba Doula Amina Amina Kinièba Franwalia Tinko Diatifere Fountou Soumbalakölen Iroda Kounkoun Koda Mainou SARAYA CENTRE Tomboni Sinimbaya KOBEDRA CENTRE MIGNADA CENTRE Bökökö Farani Banora Simbona Bida Tomba Boufe Bandioula FOULATA CENTRE Kintinian Yorola Tougnou Sanouna SEELA CENTRE Bankon MALI Tinkoba Kobada Beretela Sando Noumandiana Kandani Fodela Bèrèko Tabakoro BAMBALA Tabako Madila Moyafara Kourouni Banantamou Siguiri FALAMA BANFARA CENTRE Saint Alexis Dialakoro Nedekoroko Banantou Lansanaya Sakolado Manakoro Farabada Dounin Farabelen Bida Bantambaye Woléwoléya Koda Koda Kogne Tambabougou Gbongoroma Kigne Kokoudouninda Dinguiraye Gbilin Balandougouba KONKOYE CENTRE Waran-Fougou Kiniebakoura DIARRADOU CENTRE Sansani Faradjian Tassiliman Centre Kewoulé -

Plan De Gestion Environnementale Et Sociale (Pges)
MINISTERE DE L’AGRICULTURE REPUBLIQUE DE GUINEE ***************** TRAVAIL - JUSTICE – SOLIDARITE DIRECTION NATIONALE DU GENIE RURAL ***************** SECRETARIAT EXECUTIF DE L’ABN Public Disclosure Authorized PROJET DE DEVELOPPEMENT DES RESSOURCES EN EAU ET DE GESTION DURABLE DES ECOSYSTEMES DANS LE BASSIN DU NIGER (PDREGDE) ETUDE D’IMPACT ENVIRONNEMENTAL ET SOCIAL, EVALUATION SOCIALE ET EVENTUELS PLANS D’ACTION DE REINSTALLATION DANS LE CADRE DE L’APPUI AUX TRAVAUX D’AMENAGEMENTS HYDRO AGRICOLES, A LA RESTAURATION ET LE DEVELOPPEMENT DES ACTIVITES AGROFORESTERIES ET DE PROTECTION DES VERSANTS DANS LA REGION DE FARANAH, REPUBLIQUE DE LA GUINEE Public Disclosure Authorized Public Disclosure Authorized FINANCEMENT IDA ETUDE D’IMPACT ENVIRONNEMENTAL ET SOCIAL VERSION PROVISOIRE CORRIGEE Public Disclosure Authorized Novembre 2013 SOCIETE D’ETUDES POLYTECHNIQUES Société à responsabilité limitée au capital de 1.500.000 F CFA BP: 3069 Bamako – N° Fiscal: 086 100086 V - Tél. : (+223) 20 20 69 29) SOMMAIRE ABREVIATIONS ET ACRONYMES.......................................................................................................... 5 LISTE DES TABLEAUX ET FIGURES ...................................................................................................... 6 RESUME ....................................................................................................................................................... 8 INTRODUCTION ...................................................................................................................................... -

Sous-Préfecture De Douako
G!! (!G!! Morsira (! Sirman GUIFNadoÉugoEu - Région Kankan / Préfecture de Kouroussa - Sous-Préfecture de Douako - Carte de Base Pampam Niamana Kondé SOUS-PREFECTURE SOUS-PREFECTURE DE KINIÉRO DE BANFÉLÉ Niona Centre Djindo Yankafissa !! Kouva Famawolia ± R É G I O N D E R É G I O N D E Kinieko Nongoa 61km K A N K A N F A R A N A H Kiniekonin Poste de santé Gbossoko Arfela Centre Kanséréya !! Sanakoya (!G! Kansereya Sedakoro Kendou Fodeya Ténenkofé 24km 55km 51km!! Kolomangbeya Kidiboun Saranwaliya Kouyaléha 48km Banankoro 23km Gnarako 22km Mansouare Kolomanfiya Leybadyangna 45km Kossidiya 21km PREFECTURE DE FARANAH Irla u Sanankoro o 17km f 16km PREFECTURE a Boussoura M Poste de 19km Sansambaya 23km Danka Sangbagna santé Tindo Boumbouran DE KOU17RkmOUFSranSmAoriyasouaré 35km Centre Marenady 36km 40km !! ! Mamoudouya Fouria (!!GTindo Worondo Faceligbeya Ba Faroro 32km Tindikan lé 14km Bransan Gbelenkoro Sobalia 12km Momora Toumania Faramoriya Simbo Makarakofe Gbossokoroya 12km Serekoro Djirmalo 29km Centre Kondemoriya Condé 15km !! 11km 12km Bagnaya Kindesandofe Manicelia Maniceliya Fesse !! Selen Centre 21km Kouya-Woela SOUS-PREFECTURE !! !! Kignero (!G Kouya-Sidia 24km CentreG! Yalawa DE DOUAKO Poste de (! Finikiriya santé Dankala 15kmG Marabérétéya Kouya-Sidia Fantogna (! 9km Kolowa Kouman Poste de Centre Aryambali Kambiya !! Wonomoriya santé Mara ! 6km Worobe Bereteya Yaraya Poste de Sirakoro Talikoro 6km santé Centre Centre Silamana !! !! Tienkofé Centre Serdou Centre 15km!G! Silamana !! de sante (! Sirikoroma PREFECTURE Douako 0km -

La Région De N'zérékoré
REPUBLIQUE DE GUINEE Travail-Justice-Solidarité MINISTERE DU PLAN ET DU DEVELOPPEMENT ECONOMIQUE La région de N’Zérékoré en chiffres Edition 2020 GERAPHIE ET ORGANISATION ADMINISTRATIVE Géographie 0rganisation administrative en 2018 6 préfectures ; 60 sous-préfectures ; 6 communes urbaines, Superficie : 37 658 km2 782 districts/quartiers ; 2 541 secteurs 60 communes rurales Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) Préfectures Sous-préfectures N’Zérékoré Bounouma, Gouécké, Kobéla, Koropara, Koulé, Palé, Samoé, Soulouma, Womey ; Yalenzou, Boola, Diarraguerela, Diassadou, Fouala, Gbackedou, Gbessoba, Karala, Koumadou, Beyla Moussadou, Niossomoridou, Samana, Sinko, Sokourala Bolodou, Fangamadou, Guendembou, Kassadou, Koundou, Nongoa, Ouende-Kénéma, Tékoulo, Guéckédou Terméssadoudjibo Lola Bossou, Foubadou, Gama-Berema, Guéassou, Kokota, Laine, N’Zoo, Tounkarata, Balizia, Binikala, Bofossou, Daro, Fassankoni, Kouankan, Koyama, N’Zébela, Oremai, Panziazou, Macenta Sangbedou, Sérédou, Vaseredou, Watanka Yomou Baniré, Bheta, Bignamou, Bowé, Diecké, Péla, Yomou-Centre Source : BSD Ministère de l’administration du territoire et de la décentralisation (Annuaire statistique 2018) STATISTIQUES DEMOGRAPHIQUES Populations des RGPH 1983 1996 2014 Population région de N’Zérékoré 740 128 1 348 787 11 578 068 Population de la principale préfecture : N’Zérékoré 194 600 283 413 396 949 Part de la population nationale en 2014 : 15,0% Rang régional en 2014 3/8 Sources : Institut national -
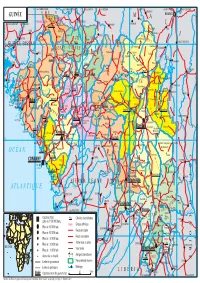
GUINÉE Gam L BAMAKO PARC NAT
14° vers TAMBACOUNDA vers TAMBACOUNDA 12° vers SARAYA vers KÉNÉBIA 10° vers KITA vers KITA 8° vers KOULIKORO vers SÉGOU S É N É G A L F SIRAKORO bie a GUINÉE Gam l BAMAKO PARC NAT. é M m A DU KONIAGUI é GALÉ FOULAKOUNDA BADIAR KÉDOUGOU g L n i B vers ZIGUINCHOR vers KOLDA F f SAGABARI a Youkounkoun ARABA a k Koundara o B y ba ï G Niagassola SIBI ê Sarébo do a G GABU Guingan m o T i b B Balandou I o i al K m T e F LÉ é R iba ouba A A M ok l i Kifaya Tamgué D A o vers BISSAO o L ro F Á K n 1538 m I BA AT Foulamôri é Balaki I Sou baraya N K A É OUÉLÉSSÉBOUGOU 12° GUINÉE-BISSAO Mali L Boukaria 12° B S m a O a Naboun Kouré alé n l y N E - G U I N É o o KANGABA k Y E N E N k a é XIME O a r M m Madina l Ya béring F a ÉL K andanda Maléa B u B I m n Koumbia Sala bandé Doko o Kounsitél É i a e Siguirini Barrage B bi g è è R al m in Diatif r E de Sélingué vers BISSAO ub Gaoual a f Rio Cor G a IG KANGARÉ BUBA oumb B Banora N é K a Koubia Nafadji n Kintinian é i i Dabalaré F m Malanta ô F o K llé ifa BOUGOUNI Wéndou Mbôrou T Ganiakali Siguiri n Fouta Labé T H Dialakoro o Lélouma ougué A g Tin vers SIKASSO o 1245 U kisso K Hamdallaï Kâkoni F L T E Kiniébakoura K O U A Dinguiraye - G Balandougouba CATIÓ LÉ o U I SANSA g Sélouma N É E o ê Dabiss H rico a Kalinko Koundianakoro n Missira Kankalabé Sangarédi m F YANFOLILA i Chutes arakoba Niandankoro r o e k de Kinkon ka s n Sansalé L A Santou a Pita s i ou i m Sansando c U K B k Ko ola Koura Niantanina a u F O Tén n ié M Niani BADOGO L C ing ilin m é i n GARA O T ta Konsota i T a O io Dobali Djalon B m