Challenges Encountered by New Zealand Mines Rescue at the Pike River Mine Disaster
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Key Points Value of Kupe to NZOG
for the quarter ended 30 June 2010 Dear investor It was a busy three month period for NZOG, Production from the Tui area oil fields slightly In May, shareholders of Pike River Coal (PRC) against a backdrop of falling international exceeded the revised target for the financial year agreed to a funding package that included a new sharemarkets and dismay over the BP oil spill in ended 30 June, producing a total of 4.83 million equity issue and around $40m of debt from the Gulf of Mexico. That disaster demonstrated barrels – NZOG’s share 604,000 barrels. NZOG NZOG through convertible bonds. More details the need for health, safety and environmental received NZ$13.1m in revenue from Tui in the about Pike can be found on the back page of performance to always be the number one June quarter. this report. priority in the petroleum industry. In late June, it was identified that repairs were The Kupe gas and oil field was in full production required to the artificial lift system for one of the through the quarter, earning NZOG NZ$18.2m in Tui field’s four producing wells, Pateke 3-H. revenue. A reserves review was completed, The Operator is planning a work-over of the David Salisbury CEO which saw the 2P (proved and probable) well later in 2010. In the meantime the well has 21 July 2010 reserves increased substantially. At current been shut-in, which means some production prices, NZOG’s share of the additional will be deferred. recoverable light oil, LPG and gas has a value of As you know, NZOG is always on the lookout around NZ$100m. -

The Impact of Non-Technical Issues on Decision-Making by Coal Mining Incident Management Teams
The impact of non-technical issues on decision-making by coal mining incident management teams. Ruth Grace Fuller BEng Hons Civil Engineering Grad Dip Psychology BSc Hons Psychology Grad Dip Secondary Education A thesis submitted for the degree of Doctor of Philosophy at The University of Queensland in 2014 Sustainable Minerals Institute Abstract A serious incident in an underground coal mine can claim many lives in an instant. The lives of those who survive the initial moments can be dependent on the decisions made by the incident management team (IMT). The IMT is a team of mine employees assembled immediately upon the discovery of an incident to manage the response. Evaluations of annual emergency exercises conducted at underground coal-mines in Queensland have indicated that IMT decision-making is generally sub-optimal. This finding was echoed by the Royal Commission into the New Zealand Pike River Coal Mine Tragedy that occurred in 2010. In many other high-reliability roles technical and non-technical issues have been found to impact decision-making. The goal of this research is to explore the role of non-technical issues in emergency decision-making following an underground coal mining incident. A review of the Queensland emergency exercise reports, direct observation of emergency simulations, and interviews with twenty-five mining personnel with real-life incident management experience at underground coal mine emergencies has led to the development of a non-technical skills taxonomy for decision-making in mining IMTs. The decision-making process in a mining IMT has been shown to be a broad socio-psycho-technical process within which technical and non-technical issues cannot be separated. -

Tuesday, March 30, 2021
TE NUPEPA O TE TAIRAWHITI TUESDAY, MARCH 30, 2021 HOME-DELIVERED $1.90, RETAIL $2.20 OKITU DEVELOPERS FINED CORN CHANGES: The Cedenco proposal to shut FOR CONSENT BREACHES down its IQF (Individually PAGE 5 Quick Frozen) plant (below) in the industrial subdivision will directly affect the jobs of 13 permanent staff. It will also affect the amount of corn grown in the district and trucked (main picture) to the factory each season. Pictures supplied PIKE RIVER FAMILIES HEARTBROKEN PAGE 6 PAGE 16 TAKING THE KNEE AT FLOYD MURDER TRIAL Proposal to close IQF CEDENCO factory will affect jobs CEDENCO Foods New by Watties. employees can be easily Zealand proposes to close one “We put the proposed changes absorbed in other departments of its four Gisborne processing to staff last week in a plan and field operations. lines in early April when the that includes reutilising our “All staff will be offered current harvest ends, and it IQF facilities for powder and redeployment either to other RESET will directly affect the jobs of 13 frozen squash facilities, which departments in Gisborne or to people. are already at full capacity,” Mr the Cedenco Hastings factory The company proposes to shut Nelson said. which the company is currently down its Individually Quick “The proposed closure of the expanding with construction of a Frozen or IQF facility which has IQF factory will allow Cedenco new apple processing plant due operated on the site since 2001. and its growers to focus on for completion in April.” “If the closure proceeds it will growing sweetcorn for its Mr Nelson said it was hoped reduce employment on the site powder operation. -

Royal Commission on the Pike River Coal Mine Tragedy 2012
H.3 Royal Commission on the Pike River Coal Mine Tragedy Te Komihana a te Karauna mo- te Parekura Ana Waro o te Awa o Pike Volume 2 + Part 1: What happened at Pike River + Part 2: Proposals for reform 2012 Author: Royal Commission on the Pike River Coal Mine Tragedy Date of Publication: October 2012 Place of Publication: Wellington, New Zealand ISBN: 978-0-477-10378-7 Cover image: Western Escarpment, Paparoa Range, West Coast, New Zealand Website: www.pikeriver.royalcommission.govt.nz 2 Volume 2 - Part 1: What happened at Pike River Contents List of figures 8 Board 46 Chief executive 46 Glossary 10 Site general manager 47 Explanatory note on the page numbering Underground mine operations 47 of references 16 Coal preparation plant 48 PART 1: What happened at Pike River Engineering 48 Technical services 48 Context 19 Project and planning 48 CHAPTER 1 Safety and training 49 Friday afternoon, 19 November 2010 20 Environment 49 A tragedy unfolds: Friday afternoon, Human resources 49 19 November 2010 20 CHAPTER 5 A planned maintenance shutdown 21 Governance and management 50 Signs that all was not well 22 Introduction 50 An electrician enters the mine 22 Composition of the board 50 Calls to emergency services 23 Executive management 50 Daniel Rockhouse 24 Legal obligations of directors 50 A rescue 25 Governance by the board 51 Two miners walk out of the portal 25 Pike’s governance documents 51 The emergency response 25 Risk assessment 52 CHAPTER 2 The challenges facing the board and executive Accident analysis – some concepts 27 management 52 -
Notes & Map Paparoa Great Walk Brochure
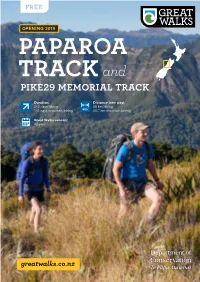
OPENING 2019 PAPAROA T R A C K and PIKE29 MEMORIAL TRACK Duration: Distance (one way): 2–3 days hiking 55 km hiking 1–2 days mountain biking 55.7 km mountain biking Great Walks season: All year PAPAROA ELEVATION PROFILE & TRACK GUIDE 1,400 m Moonlight Tops Hut Ces Clarke Hut 20 bunks 16 bunks TRACK 1,200 m 1,000 m K Experience our newest Great C 800 m Smoke-ho A R car park Pike River Mine T Walk – a purpose-built, shared-use Interpretation L (Croesus Track) IA 600 m Centre R walking and mountain biking track O EM M 400 m 29 within the Paparoa National Park on KE PI the West Coast of the South Island. 200 m This Great Walk crosses the Paparoa 0 m Range, taking you through alpine 6 – 8 hrs / 19.9 km tops, limestone karst landscapes and thriving rainforests. It provides breathtaking views across to the Southern Alps/Kā Tiritiri o te Moana and over the Tasman Sea. From the Paparoa Track, the 10.8 km Pike29 Memorial Track leads to the site of the former Pike River Mine. The track is a memorial to the 29 men who were killed in the 19 November 2010 Pike River Mine disaster. Day 1: Smoke-ho car park to Moonlight Tops Hut The Paparoa Track is open all year and provides walking and cycling access through the remote and spectacular natural wilderness 6–8 hours, 19.9 km of the Paparoa National Park. This track is The Great Walk begins at its southern end at Smoke-ho car park challenging in poor weather conditions. -

July 2013, Vol. 4 No. 7 National Labour News National, Economic
American Income Life Insurance Company 1701 K Street, N.W., Suite 300 Washington, D.C. 20006 (202) 833-2030 JAMES WILLIAMS, General President - International Union of Painters and Allied Trades, Chairman - AIL Labour Advisoury Board VICTOR KAMBER, Vice President - American Income Life Insurance Company, Executive Director - AIL Labour Advisoury Board ROGER SMITH, Chief Executive Officer - American Income Life Insurance Company, President - AIL Labour Advisoury Board DENISE BOWYER, Vice President - American Income Life Insurance Company, Secretary - AIL Labour Advisoury Board DEBBIE ENSTEDT, Vice President International Public Relations - American Income Life Insurance Company STEVE FRIEDLANDER, State General Agent - American Income Life Insurance Company July 2013, Vol. 4 No. 7 National Labour News The Government rejected calls by the Council of Trade Unions, forestry workers' unions and the Labour Party for an inquiry into the deaths of four workers earlier this year. Labour Minister Simon Bridges said the new stand-along workplace health and safety agency that will be created will take a hard look at the forestry industry. The new agency, WorkSafe New Zealand, will be established under legislation that's going through parliament. Bridges said the agency will be operational by December. CTU President Helen Kelly recently charged that Bridges gave "a misleading report" to parliament that the current code of practice in forestry "is working." "This statement from the Minster certainly does not reflect the very concerning discussion we had with the forest workers at the worksite. The workers told us that they believed many workers in the region were working in very dangerous conditions," she said. After 10 months of consultation, the Independent Taskforce on Workplace Health and Safety recently reported that current workplace safety and health systems were not fit, citing "a number of significant weaknesses" that needed addressing. -

´Group Work Speeches
´Group Work Speeches Shashi Tharoor’s address to the Oxford Union, Oxford, 2015 Video: https://www.youtube.com/watch?v=f7CW7S0zxv4 (0:00-6:48) (remember to stop the video at 6:48!) Transcript: http://www.news18.com/news/india/read-shashi-tharoors-full-speech-asking-uk-to-pay-india-for-20 0-years-of-its-colonial-rule-1024821.html Your task: Watch the speech together (go somewhere where you will not disturb anyone! – write on the blackboard where you will be sitting, so I can find you at any given time). In the speech, you must look at the following aspects: ✓ Background: o Who is the speaker? (occupation etc.) o What is the occasion/reason for the speech? ✓ What method(s) of delivery did the speaker use? -and why do you think this is the case? ✓ How is the speaker’s … o voice? (pronunciation, articulation, rhythm, volume, rate, accent/dialect) o choice of words? (accurate, clear, redundant) o body language? (gestures, movement, eye contact) ✓ Which pillars of persuasion did the speaker use to emphasize his/her point? Provide examples All of the above must be presented to the rest of the class with the use of PowerPoint. Remember to use the tools about oral communication in your own presentation as well. Presentations will be followed by feedback / Q&A. While listening to presentations, each group must note at least one thing for feedback OR come up with a question to ask the group once the presentation is done. Transcript: Madam President and gentlemen, ladies of the house I standing here with eight minutes in my hands in this venerable and rather magnificent institution, I was going to assure you that I belong to the Henry VIII School of public speaking - that as Henry VIII said to his wives 'I shall not keep you long'. -

The Institute of Quarrying New Zealand Inc
The Institute of Quarrying New Zealand Inc IoQ QUARTERLY NEWSLETTER Issue No. 26 March 2011 President’s Notes: Executive Committee Welcome Members 2010/11: Hi everybody and welcome to the New Year. President: I hope you all had a safe and happy New Mr Warwick Leach Years. I can’t believe its April already! It still Vice President: seems to be summer in the North Island with Mr Gavin Hartley our farming community a lot happier this year with the odd drop of rain, Immediate Past President: relieving the bad drought that they have had to endure for the last three Mr George Kelcher years. The Dairy companies are looking at some good pay outs for the milk Mr Murray Discombe fat this season which must a have a ‘trickle down’ affect on quarries with maintenance metal and lime rock going out the quarry gate for farm tracks Mr Chris Gray and cow races before the wet seasons arrives. Mr Gordon Laing Mr Andrew Mahon At this stage, I would just like to make comment on the Christchurch Mr Peter Morgan earthquake and pass on our deepest condolences to our Christchurch people, we always think this sort of thing just doesn’t happen in NZ. To be Mr Les Ward hit with two major earthquakes within months is unbelievable and watching National Secretary/Treasurer: the scale of the damage unfold, it was like a war zone and it made every Mrs Christine Dodds New Zealander wonder how can we help. I was talking to George Kelcher the other day and he was saying that Christchurch has 5 million tonnes of Invited Board Member: Mr Kevin Walker, waste that needs to be removed from the city and one problems they are CEO Exito facing is where can they put that amount of waste? The availability of roading work around our area sponsors with a commitment again from our hasn’t improved with work being tough and margins Platinum, Gold, Silver & Bronze sponsors. -
A Systems Failure: How the Cherries Lined up the Pike River Mine Disaster
A systems failure: how the cherries lined up THE PIKE RIVER MINE DISASTER HFESA Ron Cummings Memorial Lecture 2018 Jim Knowles November 2018 1 Background Friday, 19 November 2010 At 3:45pm, the Pike River Underground Coal Mine, near Greymouth on the west coast of the South Island, New Zealand, exploded 29 men underground died immediately or later, from the blast or from the toxic atmosphere Over the next nine days the mine exploded three more times before it was sealed. November 2018 2 The survivors Two men in the stone drift, some distance from the mine workings escaped with minor injuries. Daniel Rockhouse and Russell Smith November 2018 3 Background November 2018 Pike River Mine is still an unexplored crime scene. There has been no forensic examination of the drift or mine. No-one has been able to explain categorically what happened that day. November 2018 4 Greymouth November 2018 5 The Terrain November 2018 6 The Mine The portal (entrance) Ventilation shaft Mine workings The stone drift – 2.4km Pit bottom in stone November 2018 7 Fire at the ventilation shaft November 2018 8 Smoke from the ventilation shaft November 2018 9 The poker machine analogy “the cherries” November 2018 10 How the cherries lined up Fire Suppression Unit Accident Cherries Legislation changes Loss of specialist knowledge and skills Costs and production pressures Poor mine design and maintenance Management structure and culture Operational issues Human resources November 2018 11 The path to tragedy Changes in legislation Mines came under Health Safety and -

Murder at Pike River Mine?
1 MURDER AT PIKE RIVER MINE? The incestuous collusion between corrupt, fascist, international corporations, banks, global mining companies & compliant politicians ² And how the inexorable love of money by those who run them supersedes everything else. What was the real truth behind the Pike River coal mine disaster in New Zealand killing 29 men? ² Was the tragedy simply an ´accidentµ or was it premeditated murder? ² Involving people at the highest level of the New Zealand Government and international business and banking community? Does this case have implications for the world? by Dr Jacob Cohen This book is copyright ©. However, as it is written in the public interest, it may be freely reproduced or used by whoever may wish to use it without contacting the original author or publisher. First published in New Zealand December 24, 2010. All underlining or emphasis is the author¶s unless otherwise stated. 2 CONTENTS INTRODUCTION .............................................................................................. 3 CHAPTER ONE PIKE RIVER COALMINE HISTORY ...................................................................... 8 CHAPTER TWO PIKE RIVER COALMINE EXPLOSION & SAFETY NEGLIGENCE .......................... 10 CHAPTER THREE NAMES OF KEY PEOPLE WHO SHOULD BE CHARGED .................................... 13 CHAPTER FOUR UPPER BIG BRANCH MINE DISASTER ʹ PIKE RIVER MINE DISASTER SIMILARITIES ................................................................................................. 16 CHAPTER FIVE PIKE RIVER MINE DISASTER -

The Impact of Disasters on Independent Contractors: Victims of Circumstances
The Impact of Disasters on Independent Contractors: Victims of Circumstances Felicity Lamm Nadine McDonnell Ryan Lamare Auckland University of Technology Introduction The year 2010-2011 will be known in New Zealand as annus horribilis. Within a period of five months New Zealand had not only experienced a major mining disaster but also two major earthquakes. All three disasters were located in the South Island of New Zealand. While remarkably in the first earthquake no one was killed, the second 6.3 magnitude earthquake centred in Canterbury s largest city Christchurch killed 185 people in February 2011. Three months earlier on the 19th November 2010 a series of methane explosions at the Pike River Coal Mine (PRCM), situated outside the small regional West Coast town of Greymouth, killed 29 workers. Thirteen of the dead were contracted workers. At the time of the Pike River Coal Mine explosion, out of a workforce of 200, over 80 independent contractors were employed at the mine. Most of the independent contractors operated local, small businesses, employing on average 10 people. Pike River Coal Mine Ltd not only subcontracted manual labour (skilled and unskilled) but the company also outsourced aspects of the mine design, financial and environmental risk assessments, and a great deal of the management of occupational health and safety (OHS), such as mine ventilation. Shortly after the explosions at PRCM, the mine was closed and the company went into receivership. As most of the independent contractors were unsecured small creditors, neither they nor their workers nor their families received any money owed to them by Pike River Coal Mine Ltd (in receivership). -

RAW DATA: the Pike River Report Volume II Part Two (PDF)
CHAPTER 10 12. The five sensors circled in blue were all located within the intake roadways, in areas expected to be ventilated by fresh air. These sensors were located at or near electrical equipment in an area Pike designated as the ‘non-restricted zone’. Regulations require the non-restricted zone to contain no more than 0.25% flammable gas. The sensors in this area at Pike River were set to trip power at 0.25% methane. Sensors in the return 13. The three sensors circled in red were in the return of the ventilation system, and were intended to measure the concentration of methane in the contaminated air removed from the mine workings.23 14. The sensor at L11 stopped working on 4 September 2010,24 and the sensor at L20 stopped working on 13 October 2010,25 leaving Pike with no gas sensors reporting to the surface from further into the return than the ventilation shaft. This did not give the mine adequate information about the location, source and quantities of flammable gas within the mine. Surface controller Barry McIntosh said the controllers had raised the issue of the location of gas sensors, and in his view the gas sensors ‘weren’t up far enough’ in the mine.26 15. By way of comparison, consultant David Reece provided on request a plan showing where Pike would have typically required gas sensors under Queensland legislation. His plan was not absolute and was subject to a number of technical qualifications including the proximity of other detectors, but on the basis of the plan, Pike would probably have required seven fixed sensors (marked in red) reporting to the surface from inbye of the ventilation shaft.