World Bank Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
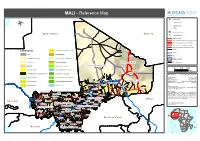
MALI - Reference Map
MALI - Reference Map !^ Capital of State !. Capital of region ® !( Capital of cercle ! Village o International airport M a u r ii t a n ii a A ll g e r ii a p Secondary airport Asphalted road Modern ground road, permanent practicability Vehicle track, permanent practicability Vehicle track, seasonal practicability Improved track, permanent practicability Tracks Landcover Open grassland with sparse shrubs Railway Cities Closed grassland Tesalit River (! Sandy desert and dunes Deciduous shrubland with sparse trees Region boundary Stony desert Deciduous woodland Region of Kidal State Boundary ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Bare rock ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Mosaic Forest / Savanna ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! Region of Tombouctou ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! ! 0 100 200 Croplands (>50%) Swamp bushland and grassland !. Kidal Km Croplands with open woody vegetation Mosaic Forest / Croplands Map Doc Name: OCHA_RefMap_Draft_v9_111012 Irrigated croplands Submontane forest (900 -1500 m) Creation Date: 12 October 2011 Updated: -

Annuaire Statistique 2015 Du Secteur Développement Rural
MINISTERE DE L’AGRICULTURE REPUBLIQUE DU MALI ----------------- Un Peuple - Un But – Une Foi SECRETARIAT GENERAL ----------------- ----------------- CELLULE DE PLANIFICATION ET DE STATISTIQUE / SECTEUR DEVELOPPEMENT RURAL Annuaire Statistique 2015 du Secteur Développement Rural Juin 2016 1 LISTE DES TABLEAUX Tableau 1 : Répartition de la population par région selon le genre en 2015 ............................................................ 10 Tableau 2 : Population agricole par région selon le genre en 2015 ........................................................................ 10 Tableau 3 : Répartition de la Population agricole selon la situation de résidence par région en 2015 .............. 10 Tableau 4 : Répartition de la population agricole par tranche d'âge et par sexe en 2015 ................................. 11 Tableau 5 : Répartition de la population agricole par tranche d'âge et par Région en 2015 ...................................... 11 Tableau 6 : Population agricole par tranche d'âge et selon la situation de résidence en 2015 ............. 12 Tableau 7 : Pluviométrie décadaire enregistrée par station et par mois en 2015 ..................................................... 15 Tableau 8 : Pluviométrie décadaire enregistrée par station et par mois en 2015 (suite) ................................... 16 Tableau 9 : Pluviométrie enregistrée par mois 2015 ........................................................................................ 17 Tableau 10 : Pluviométrie enregistrée par station en 2015 et sa comparaison à -

Par : M. Wonthy DOUCOURE Pour Obtenir Le Grade De Docteur En Pharmacie (DIPLOME D’ÉTAT)
Pratique de la contraception dans la Commune rurale de Diafounou Tambacara dans la région de Kayes au Mali MINISTERE DE L’EDUCATION NATIONALE, REPUBLIQUE DU MALI DE L’ENSEIGNEMENT SUPERIEUR ET DE Un Peuple – Un But – Une Foi LA RECHERCHE SCIENTIFIQUE UNIVERSITE DES SCIENCES, DES TECHNIQUES ET DES TECHNOLOGIES DE BAMAKO FACULTE DE PHARMACIE ANNEE UNIVERSITAIRE 2019-2020 N° /.......….. / THESE Pratique de la contraception dans la commune rurale de diafounou Tambacara dans la région de kayes au mali Présentée et soutenue publiquement le 24/09/2020 devant la Faculté de Pharmacie Par : M. Wonthy DOUCOURE Pour obtenir le grade de Docteur en Pharmacie (DIPLOME D’ÉTAT) Jury Président : Pr Boubacar TRAORE Membres : Pr Abdoulaye DJIMDE : Dr SANGO Fanta SANGHO Codirecteur : Dr Dominique P. ARAMA Directeur : Pr Ibrahima TEGUETE Thèse de Pharmacie 2019-2020 Wonthy DOUCOURE Page I Pratique de la contraception dans la Commune rurale de Diafounou Tambacara dans la région de Kayes au Mali Thèse de Pharmacie 2019-2020 Wonthy DOUCOURE Page II Pratique de la contraception dans la Commune rurale de Diafounou Tambacara dans la région de Kayes au Mali Dédicaces Au nom de DIEU Clément et Miséricordieux Louange à ALLAH SWT ! Le souverain du monde que nous adorons et dont nous implorons la très haute bénédiction. Louange à ALLAH SWT et à son prophète MOHAMED (P. S. L) ! Qui a fait que je sois de ce monde et qui m’a apporté un soutien sans faille et le courage nécessaire pour me permettre de mener à bien mes quotidiens. Permettez-moi chers parents, amis, encadreurs, en cette circonstance solennelle de vous adressée cette dédicace pour vous témoigner ma reconnaissance indéfectible à la suite de votre remarquable concours grâce auquel j’ai pu mener à ce travail. -

World Bank Document
Document of The World Bank Public Disclosure Authorized FOR OFFICIAL USE ONLY Report No: 39308 - ML PROJECT APPRAISAL DOCUMENT ON A Public Disclosure Authorized PROPOSED CREDIT IN THE AMOUNT OF SDR59.5 MILLION (US$90.0 MILLIONEQUIVALENT) TO THE REPUBLIC OF MALI FOR A Public Disclosure Authorized SECOND TRANSPORT SECTOR PROJECT April 30,2007 This document has a restricted distribution and may be used by recipients only in the Public Disclosure Authorized performance oftheir official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective March 3 1,2007) Currency Unit = Franc CFA CFAF 495 = US$1 US$1.51326 = SDR 1 US$1= SDR 0.660825 FISCAL YEAR January 1-December 3 1 *. 11 - ABBREVIATIONS AND ACRONYMS ACDP Agricultural Competitiveness and Diversification Project AFD Agence Franqaise de Dheloppement (French Agency for Development) AfDB African Development Bank AGEROUTE Agence d’extcution d’Entretien des Travaux Routiers (Road Works Execution Agency) AGETIER Agence d’extcution des Travaux d’hfiastructure et d’Equipements Ruraux (Infrastructure and Rural Equipment Works Execution Agency) ASPEN Africa Safeguards Policy Enhancement BOAD Banque Ouest Afhcaine de DCveloppement CAS Country Assistance Strategy CDD Community Driven Development CETAC Technical Committee of Support to Towns CFAA Country Financial Accountability Assessment CFAF Franc ofthe French Community ofAfhca CMDT Compagnie Malienne pour le Ddveloppement des Textiles (Malian Textile Development Company) -

Mli0006 Ref Region De Kayes A3 15092013
MALI - Région de Kayes: Carte de référence (Septembre 2013) Limite d'Etat Limite de Région MAURITANIE Gogui Sahel Limite de Cercle Diarrah Kremis Nioro Diaye Tougoune Yerere Kirane Coura Ranga Baniere Gory Kaniaga Limite de Commune Troungoumbe Koro GUIDIME Gavinane ! Karakoro Koussane NIORO Toya Guadiaba Diafounou Guedebine Diabigue .! Chef-lieu de Région Kadiel Diongaga ! Guetema Fanga Youri Marekhaffo YELIMANE Korera Kore ! Chef-lieu de Cercle Djelebou Konsiga Bema Diafounou Fassoudebe Soumpou Gory Simby CERCLES Sero Groumera Diamanou Sandare BAFOULABE Guidimakan Tafasirga Bangassi Marintoumania Tringa Dioumara Gory Koussata DIEMA Sony Gopela Lakamane Fegui Diangounte Goumera KAYES Somankidi Marena Camara DIEMA Kouniakary Diombougou ! Khouloum KENIEBA Kemene Dianguirde KOULIKORO Faleme KAYES Diakon Gomitradougou Tambo Same .!! Sansankide Colombine Dieoura Madiga Diomgoma Lambidou KITA Hawa Segala Sacko Dembaya Fatao NIORO Logo Sidibela Tomora Sefeto YELIMANE Diallan Nord Guemoukouraba Djougoun Cette carte a été réalisée selon le découpage Diamou Sadiola Kontela administratif du Mali à partir des données de la Dindenko Sefeto Direction Nationale des Collectivités Territoriales Ouest (DNCT) BAFOULABE Kourounnikoto CERCLE COMMUNE NOM CERCLE COMMUNE NOM ! BAFOULABE KITA BAFOULABE Bafoulabé BADIA Dafela Nom de la carte: Madina BAMAFELE Diokeli BENDOUGOUBA Bendougouba DIAKON Diakon BENKADI FOUNIA Founia Moriba MLI0006 REF REGION DE KAYES A3 15092013 DIALLAN Dialan BOUDOFO Boudofo Namala DIOKELI Diokeli BOUGARIBAYA Bougarybaya Date de création: -

Avis D'appel D'offres International
RÉPUBLIQUE DU MALI Un Peuple – Un But –Une Foi ----------------------- MINISTERE DE L’AGRICULTURE ------------------------- SECRÉTARIAT GENERAL ------------------------- Agence d'Exécution des Travaux d'Infrastructures et d'Équipements Ruraux (AGETIER) Projet 1 du Programme de Renforcement de la Résilience a l’insécurité alimentaire et nutritionnelle au Sahel (P2RS) Travaux de construction de Micro Barrages, de surcreusement de Mares et d’aménagement de Bas-Fonds dans les cercles de Diéma et Nioro (Région de Kayes) ; Banamba, Kolokani et Nara (Région de Koulikoro) en cinq (05) lots AVIS D’APPEL D’OFFRES INTERNATIONAL Date : 06/03/2019 AOI N°: 04/ DG/AGETIER/ 2019 Micro barrages : Prêt FAD N° : 2100150032043 : 100% Mares : Protocole d’Accord de Don ° 2100155028523 : 100% Bas-fonds : - Prêt FAD N° 2100150032043 : 95% - Bénéficiaires : 5% N° d’identification Projet : P-Z1-AAZ-018 1. Le présent avis d’appel d’offres international (AAOI) suit l’avis général de passation des marchés du projet paru sur le site Développent Business et sur le portail de la Banque (www.afdb.org) le 15/10/2015, et dans l’Essor, quotidien national d’information du Mali N° 18037 du 22/10/2015. 2. Le Gouvernement de la République du Mali a reçu un financement de la Banque Africaine de Développement en divers monnaies, pour couvrir le coût du Projet 1 du Programme de Renforcement de la Résilience a l’insécurité alimentaire et nutritionnelle au Sahel (P2RS), et entend affecter une partie du produit de ce financement aux paiements relatifs aux marchés pour les Travaux de construction de Micro Barrages, de surcreusement de Mares et d’aménagement de Bas-Fonds dans les cercles de Diéma et Nioro (Région de Kayes) ; Banamba, Kolokani et Nara (Région de Koulikoro). -

Cercle De Kayes
Cercle de Kayes REPERTOIRE Des fonds clos du Cercle de Kayes (Document provisoire) 275 CARTONS- 30,25 METRES LINEAIRES Août 2010 LES ARCHIVES Les archives jouent un rôle important dans la vie administrative, économique, sociale et culturelle d’un pays. Le développement économique, social et culturel d’un pays dépend de la bonne organisation de ses archives. Les documents d’archives possèdent une valeur probatoire, sans eux, rien ne pourrait être affirmé avec certitude, car le témoignage humain est sujet à l’erreur et à l’oubli. Les documents d’archives doivent fonctionner comme le rouage essentiel de l’Administration, et fournissent des ressources indispensables à la recherche. Les archives représentent la mémoire d’un pays. La bonne organisation des archives est un des aspects de la bonne organisation administrative. Il faut que chacun ait conscience que chaque fois qu’on détruit ou laisse détruire des archives, c’est une possibilité de gouverner qui disparaît, c’est-à-dire une part du passé de notre nation. La vigilance est un devoir. 2 Série A – Actes officiels Carton A/1–A/2-A/3 : A/1 : - Projet de constitution (1958) - Loi (1959) - Loi n˚52-130 du 6 février 1952 relative à la formation des Assemblées locales - document endommagé (1952) - Loi électorale adoptée en première lecture le 24 avril 1951 par l’Assemblée nationale (1951) - Projet de loi relatif à la formation des Assemblées du Groupe et des Assemblées locales de l’AOF, l’AEF, Cameroun, Togo et Madagascar (1951) A/2 : - Ordonnance désignant un agent d’exécution. Ordonnance -
![Course Title]](https://docslib.b-cdn.net/cover/9193/course-title-1129193.webp)
Course Title]
[School] [Course title] UNIVERSITE DES LETTRES ET DES SCIENCES HUMAINES DE BAMAKO Départements sciences de l’éducation/ Sociologie et anthropologie B.P. E3637 .Bamako – Mali Women in Law And Development in Africa Tél. (223) 76 30 54 42 OU 76 19 69 99 / E-mail : [email protected] - http:// www.ulshb.edu.ml Femmes, Droit et Développement en [email protected] Afrique BP 7755, Lomé Togo Tél. : (228) 22-61 26 79 - Fax : (228) 22 61 73 90 E-mail : [email protected] ou [email protected] RECHERCHE-ACTION Lutter contre les mariages précoces par l’autonomisation des filles au Mali RAPPORT CONSOLIDE DE L’ETUDE DE BASE Bamako, 07 Mai 2017 1 TABLE DES MATIERES Table des matières TABLE DES MATIERES ......................................................................................................... 2 LISTE DES ENCADRES .......................................................................................................... 3 LISTE DES CHANSONS LOCALES PORTANT SUR LE MARIAGE PRECOCE .............. 3 LISTE DES TABLEAUX .......................................................................................................... 3 SIGLES ET ACRONYMES ...................................................................................................... 5 RESUME EXECUTIF ............................................................................................................... 6 INTRODUCTION .................................................................................................................... 10 APPROCHE METHODOLOGIQUE ..................................................................................... -

IBM News - Mali
OCTOBER5 OCTOBER 2016 2016 IBM News - Mali Immigration and Border Management Technical Cooperation National Police graduates at the IOM training course on border management, Sikasso, 2016 Ucita det publica venatua vic tere consident vit vidium es contere, nicaudam oc mis cultorTibus nonsequo HIGHLIGHTSmaximolo quis vid ut poriatibea doles dusciis serecusdaes etus dolorum iuscia et pre occulles ea cus repelic Working with the Malian Building border control posts Training the Police and other Government and UN partners and installing migration IBM agencies in border on developing the National management IT systems management and travel Border Policy and IBM Strategy (MIDAS) in Gogui and Sona document examination IBM in Mali Welcome to the Newsletter of the IBM programme at the IOM Mission in Mali. IBM stands for Immigration and Border Management technical assistance that IOM has been providing globally, including to the Member States in the Sahel region. IOM works closely with the Malian Government on IBM matters. Since 2012 Mali, a conflict-affected state facing stabilization challenges, is engaged in an ongoing political and technical dialogue with the international community tackling the root causes of instability. This Newsletter provides a glimpse of recent IOM IBM activities and border management developments in Mali. CONTACTS IBM Tel: +223 20 22 76 97 [email protected] 17, Route des Morillons, IOM Mission in Mali Fax:+223 20 22 76 98 CH-1211 Geneva 19, Magnambougou https://mali.iom.int/ Switzerland Badalabogou Est +41.22.717.9111 BPE 288, Bamako, Mali © 2016 | INTERNATIONAL ORGANIZATION FOR MIGRATION OCTOBER 2016 5 NOVEMB Borders, Security and Development In Mali, as elsewhere in the Sahel region, governance challenges and need for stronger institutional capacity to manage security threats are high on the policy agenda. -

SITUATION DES FOYERS DE FEUX DE BROUSSE DU 15 Au 17 OCTOBRE 2014 SELON LE
MINISTERE DE L’ENVIRONNEMENT REPUBLIQUE DU MALI DE L’EAU ET DE l’ASSAINISSEMENT UN PEUPLE-UN BUT-UNE FOI DIRECTION NATIONALE DES EAUX ET FORETS(DNEF) SYSTEME D’INFORMATION FORESTIER (SIFOR) SITUATION DES FOYERS DE FEUX DE BROUSSE DU 15 au 17 OCTOBRE 2014 SELON LE SATTELITE MODIS. LATITUDES LONGITUDES VILLAGES COMMUNES CERCLES REGIONS 12,3150000000 -9,9470000000 SITAOULI KOULOU KITA KAYES 12,5960000000 -9,0010000000 GORO MAKANO KITA KAYES 12,8610000000 -9,0410000000 KOUNSALA SEBEKORO KITA KAYES 13,9030000000 -9,0520000000 BAMBARA MADINA KITA KAYES 14,1980000000 -9,0870000000 BENDOUGOU DIANGUIRDE DIEMA KAYES 14,1600000000 -9,3100000000 SAKORA GUEMOUKOURABA KITA KAYES 14,2880000000 -8,8900000000 SAGABARA-S MADINA KITA KAYES 14,2330000000 -11,014000000 MOUNITACO DIAMOU KAYES KAYES 14,3000000000 -11,082000000 MAMACITA SEGALA KAYES KAYES 14,3550000000 -11,093000000 DRAMECO SEGALA KAYES KAYES 14,3600000000 -11,099000000 DRAMECO DIAMOU KAYES KAYES 14,5710000000 -11,553000000 SOMANKIDI BANGASSI KAYES KAYES 14,4740000000 -10,883000000 KOUBINE MARINTOUMANIA KAYES KAYES 14,5570000000 -11,972000000 TOUBABOUNK FALEME KAYES KAYES 14,0910000000 -8,9470000000 BENDOUGOU GUEMOUKOURABA KITA KAYES 14,5380000000 -12,035000000 SOBOKOU FALEME KAYES KAYES 14,0590000000 -8,9220000000 BENDOUGOU MADINA KITA KAYES 13,8760000000 -8,5030000000 BORO ET SO MADINA KITA KAYES 14,3090000000 -11,717000000 MARENA-GAD SADIOLA KAYES KAYES 14,3000000000 -11,718000000 SOUKOURANI SADIOLA KAYES KAYES 13,7870000000 -8,7100000000 SAMAKOULOU MADINA KITA KAYES 13,6810000000 -8,9260000000 -

IMRAP, Interpeace. Self-Portrait of Mali on the Obstacles to Peace. March 2015
SELF-PORTRAIT OF MALI Malian Institute of Action Research for Peace Tel : +223 20 22 18 48 [email protected] www.imrap-mali.org SELF-PORTRAIT OF MALI on the Obstacles to Peace Regional Office for West Africa Tel : +225 22 42 33 41 [email protected] www.interpeace.org on the Obstacles to Peace United Nations In partnership with United Nations Thanks to the financial support of: ISBN 978 9966 1666 7 8 March 2015 As well as the institutional support of: March 2015 9 789966 166678 Self-Portrait of Mali on the Obstacles to Peace IMRAP 2 A Self-Portrait of Mali on the Obstacles to Peace Institute of Action Research for Peace (IMRAP) Badalabougou Est Av. de l’OUA, rue 27, porte 357 Tel : +223 20 22 18 48 Email : [email protected] Website : www.imrap-mali.org The contents of this report do not reflect the official opinion of the donors. The responsibility and the respective points of view lie exclusively with the persons consulted and the authors. Cover photo : A young adult expressing his point of view during a heterogeneous focus group in Gao town in June 2014. Back cover : From top to bottom: (i) Focus group in the Ségou region, in January 2014, (ii) Focus group of women at the Mberra refugee camp in Mauritania in September 2014, (iii) Individual interview in Sikasso region in March 2014. ISBN: 9 789 9661 6667 8 Copyright: © IMRAP and Interpeace 2015. All rights reserved. Published in March 2015 This document is a translation of the report L’Autoportrait du Mali sur les obstacles à la paix, originally written in French. -

World Bank Document
The World Bank RESTRUCTURING ISDS OMVS - TRANSMISSION EXPANSION PROJECT (P147921) Public Disclosure Authorized Integrated Safeguards Data Sheet Restructuring Stage Public Disclosure Authorized Restructuring Stage | Date ISDS Prepared/Updated: 26-Mar-2020| Report No: ISDSR29108 Public Disclosure Authorized Regional Vice President: Ousmane Diagana Country Director: Deborah L. Wetzel Regional Director: Riccardo Puliti Practice Manager: Charles Joseph Cormier Task Team Leader: Thierno Bah Public Disclosure Authorized The World Bank RESTRUCTURING ISDS OMVS - TRANSMISSION EXPANSION PROJECT (P147921) Note to Task Teams: The following sections are system generaed and can only be edited online in the Portal. I. BASIC INFORMATION 1. BASIC PROJECT DATA Project ID Project Name P147921 OMVS - TRANSMISSION EXPANSION PROJECT Task Team Leader(s) Country Thierno Bah Western Africa Approval Date Environmental Category 12-May-2017 Partial Assessment (B) Managing Unit IAWE2 PROJECT FINANCING DATA (US$, Millions) SUMMARY-NewFin1 Total Project Cost 103.00 Total Financing 103.00 Financing Gap 0.00 DETAILS-NewFinEnh1 World Bank Group Financing International Development Association (IDA) 97.00 IDA Credit 97.00 Non-World Bank Group Financing Counterpart Funding 6.00 Borrower/Recipient 6.00 The World Bank RESTRUCTURING ISDS OMVS - TRANSMISSION EXPANSION PROJECT (P147921) 2. PROJECT INFORMATION PROG_INF O Current Program Development Objective The project development objective is to enhance electricity trade among Mali, Mauritania, and Senegal. 3. PROJECT DESCRIPTION A. Project Status 1. The Government of Senegal is Recipient of an IDA financing in the amount of EUR 91.5 million (equivalent to US$97 million) to implement TEP. The IDA Credit 60330 was approved by the World Bank Board of Executive Directors on May 12, 2017.