Infectious Endocarditis Causing Ventricular Wall Rupture
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Unique Mitral Valve Mass: Think Beyond Vegetation
Published online: 2021-08-09 CASE REPORT Unique mitral valve mass: Think beyond vegetation Mahmoud Farhoud, Husam Bakdash Department of Internal Medicine, University of Kansas School of Medicine, Wichita, Kansas, United States Access this article online ABSTRACT Website: www.avicennajmed.com DOI: 10.4103/2231-0770.140661 Osteosarcoma is a rare cardiac malignant tumor. This case of cardiac osteosarcoma presented Quick Response Code: with atrial fibrillation. Initial echocardiogram demonstrated mitral valve echodensity and mitral valve regurgitation. Surgery and histopathological examination identified the tumor as an osteosarcoma. Tumor grade appeared to be prognostically important in cardiac sarcoma, with poor prognosis in high‑grade tumors. Key words: Atrial fibrillation, cardiac osteosarcoma, mitral valve, vegetation INTRODUCTION An electrocardiogram showed AF with RVR and no specific ST segment or T wave abnormalities. The patient was A primary cardiac malignant tumor is very rare. About 75% admitted to the telemetry ward and started on diltiazem drip. of primary cardiac tumors are benign, and 75% of these are atrial myxomas.[1] Most cardiac malignant tumors are Transthoracic echocardiography demonstrated normal metastatic tumors from melanoma, lung carcinoma, and systolic function and the anterior mitral valve leaflet was breast carcinoma.[2] Primary cardiac osteosarcomas usually severely thickened, with extensive vegetation/mass involving originate in the left atrium.[3] In contrast, osteosarcomas the whole leaflet [Figure 1 and Video 1]. There were severe metastatic to the heart most commonly involve the right mitral regurgitation and moderate mitral stenosis. Blood cardiac chambers.[4] We present a patient who had atrial cultures and serologies for cat scratch disease, brucella, fibrillation (AF) and mitral valve mass. -

Infective Endocarditis in Neonates
Arch Dis Child: first published as 10.1136/adc.63.1.53 on 1 January 1988. Downloaded from Archives of Disease in Childhood, 1988, 63, 53-57 Infective endocarditis in neonates C O'CALLAGHAN AND P MCDOUGALL Department of Neonatology, Royal Children's Hospital, Melbourne, Australia SUMMARY Five patients with neonatal infective endocarditis were reviewed, two of whom survived. Infection was caused by Staphylococcus aureus in four and by Candida albicans in one. All cases of bacterial endocarditis had clinical signs of septicaemia, positive blood cultures, thrombocytopenia, microscopic haematuria, and heart murmurs. Three developed skin abscesses early in their illnesses. Three patients had two dimensional echocardiographic studies that showed bacterial vegetations. One of these studies was done before the heart murmur could be heard. We suggest that echocardiography in conjunction with the clinical picture described may help in making an early diagnosis of endocarditis in neonates. Bacterial endocarditis in neonates is a rare and and tracheal aspirates; he was treated with intra- usually fatal disease; the first survivor was reported venous vancomycin. in 1983.1 2We became interested in the disease after At 26 days of age the baby had not improved and two patients in our neonatal unit survived. We a systolic murmur could be heard. Echocardio- therefore reviewed all five cases of neonatal infec- graphy showed vegetation round the mitral valve. tive endocarditis seen at this hospital over the past Despite the addition of fusidic acid to his treatment 10 years to see if we could find similarities that could he continued to deteriorate and died at 28 days. -

Refractory Chest Pain Or Treating Cardiologist’S Bane: a Case Report
THIEME Case Report 49 Refractory Chest Pain or Treating Cardiologist’s Bane: A Case Report Anupama V. Hegde1 Abhinay Tibdewal1 Vadagenalli S. Prakash1 Sarthak Sahoo1 1 Department of Cardiology, M. S. Ramaiah Medical College and Address for correspondence Anupama V. Hegde, MBBS, DNB Hospitals, Bengaluru, Karnataka, India (Medicine), DNB (Cardiology), Department of Cardiology, M. S. Ramaiah Medical College and Hospitals, Bengaluru 560054, Indian J Cardiovasc Dis Women-WINCARS 2017;2:49–53. Karnataka, India (e-mail: [email protected]). Abstract Microvascular angina is caused by dysfunction of small-resistance coronary arteries (< 500 µm) and is of heterogenous origin. The major epicardial coronaries are normal and commonly seen in women. Prognosis is variable, with disabling angina in many patients and can be a cause of mortality, especially in those who are refractory to Keywords treatment. In this background, we present a case of 56-year-old post valve replacement ► aortic valve with normally functioning aortic valve and recurrent episodes of microvascular angina. The replacement patient had normal epicardial coronaries. She had recurrent episodes of angina refractory ► coronary to various antianginals associated with hemodynamic instability. Microvascular angina angiography can curtail routine activity, frequent hospitalization, and repeated noninvasive and invasive ► microvascular angina investigations. Thus, it is a high social and economical disease, especially pertinent to ► refractory chest pain women. Introduction induced angina and normal coronary angiograms. However, the use of this term has not always been limited to this specific The first mention of chest pain with normal coronaries was meaning.4 made in 1981 by Opherk and coworkers.1 Among patients undergoing coronary angiography (CAG) for ischemic signs Case Report and symptoms, approximately10 to 30%have angiographically normal coronaries. -

Rheumatic Mitral Valve Stenosis: Diagnosis and Treatment Options
Current Cardiology Reports (2019) 21: 14 https://doi.org/10.1007/s11886-019-1099-7 STRUCTURAL HEART DISEASE (RJ SIEGEL AND NC WUNDERLICH, SECTION EDITORS) Rheumatic Mitral Valve Stenosis: Diagnosis and Treatment Options Nina C. Wunderlich1 & Bharat Dalvi2 & Siew Yen Ho3 & Harald Küx1 & Robert J. Siegel4 Published online: 28 February 2019 # Springer Science+Business Media, LLC, part of Springer Nature 2019 Abstract Purpose of Review This review provides an update on rheumatic mitral stenosis. Acute rheumatic fever (RF), the sequela of group A β-hemolytic streptococcal infection, is the major etiology for mitral stenosis (MS). Recent Findings While the incidence of acute RF in the Western world had substantially declined over the past five decades, this trend is reversing due to immigration from non-industrialized countries where rheumatic heart disease (RHD) is higher. Pre- procedural evaluation for treatment of MS using a multimodality approach with 2D and 3D transthoracic and transesophageal echo, stress echo, cardiac CT scanning, and cardiac MRI as well as hemodynamic assessment by cardiac catheterization is discussed. The current methods of percutaneous mitral balloon commissurotomy (PMBC) and surgery are also discussed. New data on long-term follow-up after PMBC is also presented. Summary For severe rheumatic MS, medical therapy is ineffective and definitive therapy entails PMBC in patients with suitable morphological mitral valve (MV) characteristics, or surgery. As procedural outcomes depend heavily on appropriate case selection, definitive imaging and interpretation are crucial. It is also important to understand the indications as well as morpho- logical MV characteristics to identify the appropriate treatment with PMBC or surgery. -

Left Atrial Vegetation After Pulmonary Vein Isolation Sean Gaine,1 John Joseph Coughlan ,2 Richard Szirt,3 Sadat Ali Edroos 4
Images in… BMJ Case Rep: first published as 10.1136/bcr-2020-235833 on 17 August 2020. Downloaded from Left atrial vegetation after pulmonary vein isolation Sean Gaine,1 John Joseph Coughlan ,2 Richard Szirt,3 Sadat Ali Edroos 4 1Cardiology, St James’s Hospital, DESCRIPTION Dublin, Ireland A- 67- year old man presented with acute left hemi- 2 Cardiology, University Hospital paresis 6 weeks after pulmonary vein isolation Limerick, Limerick, Ireland (PVI) for atrial fibrillation. His medical history 3Department of Cardiology, St was notable for hypertension and a metallic aortic George Hospital, Kogarah, New South Wales, Australia valve which was implanted 23 years previously for 4St James’s Hospital, Dublin, bicuspid aortic stenosis. He was warfarinised for his Ireland metallic valve and his warfarin had been suspended for 5 days prior to ablation. Correspondence to Clinical examination demonstrated left upper Dr Sean Gaine; sgaine@ tcd. ie and lower limb weakness. CT brain suggested right Figure 2 Gated cardiac CT confirming the presence of middle cerebral artery branch occlusion. His inter- the vegetation in proximity to the oesophagus. It did not Accepted 29 June 2020 national normalised ratio was high at 4.6 ruling find any evidence of an atrio- oesophageal fistula (black out thrombolysis. The hemiparesis resolved within arrow). hours, and he was admitted for observation. He deteriorated the next day with bilateral weakness of left lower and right upper limbs. Following seizure to permit long- term antibiotics in the context of activity, the patient dropped his Glasgow Coma sepsis, prior to committing to a permanent device. Scale and required intubation. -

Spontaneous Hemopericardium Leading to Cardiac Tamponade in a Patient with Essential Thrombocythemia
SAGE-Hindawi Access to Research Cardiology Research and Practice Volume 2011, Article ID 247814, 3 pages doi:10.4061/2011/247814 Case Report Spontaneous Hemopericardium Leading to Cardiac Tamponade in a Patient with Essential Thrombocythemia Anand Deshmukh,1, 2 Shanmuga P. Subbiah,3 Sakshi Malhotra,4 Pooja Deshmukh,4 Suman Pasupuleti,1 and Syed Mohiuddin1, 4 1 Department of Cardiovascular Medicine, Creighton University Medical Center, Omaha, NE 68131, USA 2 Creighton Cardiac Center, 3006 Webster Street, Omaha, NE 68131, USA 3 Department of Hematology and Oncology, Creighton University Medical Center, Omaha, NE 68131, USA 4 Department of Internal Medicine, Creighton University Medical Center, Omaha, NE 68131, USA Correspondence should be addressed to Anand Deshmukh, [email protected] Received 30 October 2010; Accepted 29 December 2010 Academic Editor: Syed Wamique Yusuf Copyright © 2011 Anand Deshmukh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Acute cardiac tamponade requires urgent diagnosis and treatment. Spontaneous hemopericardium leading to cardiac tamponade as an initial manifestation of essential thrombocythemia (ET) has never been reported in the literature. We report a case of a 72-year-old Caucasian female who presented with spontaneous hemopericardium and tamponade requiring emergent pericardiocentesis. The patient was subsequently diagnosed to have ET. ET is characterized by elevated platelet counts that can lead to thrombosis but paradoxically it can also lead to a bleeding diathesis. Physicians should be aware of this complication so that timely life-saving measures can be taken if this complication arises. -

Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use
Otterbein University Digital Commons @ Otterbein Nursing Student Class Projects (Formerly MSN) Student Research & Creative Work Summer 7-30-2018 Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use Kaleigh Cline Otterbein University, [email protected] Follow this and additional works at: https://digitalcommons.otterbein.edu/stu_msn Part of the Cardiovascular Diseases Commons, and the Nursing Commons Recommended Citation Cline, Kaleigh, "Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use" (2018). Nursing Student Class Projects (Formerly MSN). 286. https://digitalcommons.otterbein.edu/stu_msn/286 This Project is brought to you for free and open access by the Student Research & Creative Work at Digital Commons @ Otterbein. It has been accepted for inclusion in Nursing Student Class Projects (Formerly MSN) by an authorized administrator of Digital Commons @ Otterbein. For more information, please contact [email protected]. Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use Kaleigh Cline BSN, RN Otterbein University, Westerville, Ohio Underlying Pathophysiology Significance of Pathophysiology Conclusion Introduction Underlying Lesion: Degenerative processes such as fibrosis, calcification, congenital heart diseases, mechanical IE is a significant diagnosis because of its ability to affect almost every vital body system. lesions secondary to material implantation, and turbulent blood flows (IVDU) causes endocardial • Infective Endocarditis is a •Intravenous drug use (IVDU) poses many risks to those who use them. One of damage. This then exposes the extracellular matrix and results in apoptosis of endocardial cells which • Heart Failure - Heart failure is the most common complication from IE and can often leads to surgical serious condition associated that the risks being infective endocarditis. then produces tissue factor and a non-bacterial thrombus formation. -

Anticoagulant-Induced Hemopericardium with Tamponade: a Case Report and Review of the Literature
JCEI / Ertaş et al. Hemopericardium with tamponade 2013; 4 (2): 229-233229 Journal of Clinical and Experimental Investigations doi: 10.5799/ahinjs.01.2013.02.0273 CASE REPORT Anticoagulant-induced hemopericardium with tamponade: A case report and review of the literature Antikoagülasyonun indüklediği hemoperikardiyumlu tamponad: Olgu sunumu ve literatür incelemesi Faruk Ertaş, Nihat Polat, Abdulkadir Yıldız, Mustafa Oylumlu, Mehmet Sıddık Ülgen ABSTRACT ÖZET Acute cardiac tamponade requires urgent diagnosis and Akut kardiyak tamponad acil tanı ve tedavi gerektirir. Biz treatment. We report a case of a 43-year-old man who 43 yaşında, erkek ve mitral valv replasmanı sonrası sekiz was receiving warfarin treatment for 8 months following aydır warfarin tedavisi alan bir olguyu aldık. Hastanın bir- mitral valve replacement. The patient had complaint of kaç gündir başlayan nefes darlığı ve halsizlik şikayetikleri dyspnea and fatigue for a few days. Cardiac tamponade mevcuttu. Kardiyak tamponad tanısı konuldu ve 1400 ml was diagnosed, and the INR at that time was 10.4. Urgent mai perikardiyosentezle acil olarak drene edildi. Tanı sı- pericardiocentesis were undertaken and 1400 ml of peri- rasında İNR değeri çok yüksek olan hastaya Vitamin K cardial blood was drained. Following surgery the patient’s antagonistleri ve taze donmuş plazma verilerek yuksek recovery was uneventful. An intravenous vitamin K injec- koagülasyon durumu geriye döndürüldü. Patolojik incele- tion and fresh frozen plasma transfusion were adminis- me sonucunda enfeksiyon ve malingnensi saptanmadı. tered to reverse the patient’s over-anticoagulated state. Hastada kronik inflamasyon düşünüldü. Sonuç olarak The final pathology revealed chronic inflammation and warfarin overdoz acil bir durum olup hemoperikardiyumla there was no malignancy, and no bacteria or mycobacte- tamponada yol açabilmektedir. -

Hemopericardium by Gunshot Without Cardiac Injury, Description of a Trauma Mechanism
Rev Colomb Cir. 2020;35:108-12 https://doi.org/10.30944/20117582.594 PRESENTACIÓN DE CASO Hemopericardium by gunshot without cardiac injury, description of a trauma mechanism Hemopericardio por disparo sin lesión cardíaca, descripción de un mecanismo de trauma Bruno José da Costa Medeiros1, Antonio Oliveira Araujo2, Adriana Daumas Pinheiro Guimarães3 1. General surgeon, Instituto de Cirurgia do Estado do Amazonas - ICEA. Manaus, AM 69053610, Phone number: 5592984490880 e-mail: [email protected] 2. Vascular Surgeon, Instituto de Cirurgia do Estado do Amazonas - ICEA. Manaus, AM 69053610, Phone number: 55929992247630 3. General Surgeon, Instituto de Cirurgia do Estado do Amazonas - ICEA. Manaus, AM 69053610, Phone number: 5592991420229 Resumen Introducción. Durante muchos siglos, las heridas del corazón se consideraron fatales. Actualmente, el trauma cardíaco sigue siendo una de las lesiones más letales. Los resultados de pacientes con lesión cardíaca penetrante pueden variar de lesiones letales a arritmias que se resuelven espontáneamente. El hemopericardio en el trauma generalmente es debido a la lesión cardíaca penetrante, pero el saco pericárdico puede llenarse de sangre de grandes vasos y de la ruptura de la arteria pericardiofrénica asociada a laceración pericárdica contusa. Métodos. Para la organización de este estudio, se realizó una búsqueda bibliográfica en la literatura científica. Dos casos fueron observados por el equipo de Cirugía General al describir este raro mecanismo de trauma. Resultados. Descripción de una causa diferente de hemopericardio, ocasionada por la sangre de la cavidad peritoneal. Discusión. En los casos presentados, la lesión por arma de fuego rompió la barrera entre las cavidades pericár- dica y peritoneal (diafragma), colocando cavidades con diferentes niveles de presión , favoreciendo la entrada de sangre de la cavidad peritoneal al saco pericárdico. -

Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism
ASE GUIDELINES AND STANDARDS Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism Muhamed Saric, MD, PhD, FASE, Chair, Alicia C. Armour, MA, BS, RDCS, FASE, M. Samir Arnaout, MD, Farooq A. Chaudhry, MD, FASE, Richard A. Grimm, DO, FASE, Itzhak Kronzon, MD, FASE, Bruce F. Landeck, II, MD, FASE, Kameswari Maganti, MD, FASE, Hector I. Michelena, MD, FASE, and Kirsten Tolstrup, MD, FASE, New York, New York; Durham, North Carolina; Beirut, Lebanon; Cleveland, Ohio; Aurora, Colorado; Chicago, Illinois; Rochester, Minnesota; and Albuquerque, New Mexico Embolism from the heart or the thoracic aorta often leads to clinically significant morbidity and mortality due to transient ischemic attack, stroke or occlusion of peripheral arteries. Transthoracic and transesophageal echo- cardiography are the key diagnostic modalities for evaluation, diagnosis, and management of stroke, systemic and pulmonary embolism. This document provides comprehensive American Society of Echocardiography guidelines on the use of echocardiography for evaluation of cardiac sources of embolism. It describes general mechanisms of stroke and systemic embolism; the specific role of cardiac and aortic sour- ces in stroke, and systemic and pulmonary embolism; the role of echocardiography in evaluation, diagnosis, and management of cardiac and aortic sources of emboli including the incremental value of contrast and 3D echocardiography; and a brief description of alternative imaging techniques and their role in the evaluation of cardiac sources of emboli. Specific guidelines are provided for each category of embolic sources including the left atrium and left atrial appendage, left ventricle, heart valves, cardiac tumors, and thoracic aorta. In addition, there are recommen- dation regarding pulmonary embolism, and embolism related to cardiovascular surgery and percutaneous procedures. -

Tricuspid Valve Endocarditis with Large Vegetation in a Non Drug Addict Patient
Cas Clinique TRICUSPID VALVE ENDOCARDITIS WITH LARGE VEGETATION IN A NON DRUG ADDICT PATIENT L. ABID, L. LAROUSSI, S. CHTOUROU, CH. HAMZA, S KRICHÈNE, D. ABID, M. AKROUT, S. MALLEK, F. TRIKI, M. HENTATI, S. KAMMOUN Cardiology department, Hedi Chaker hospital, Sfax University -Tunisia Summary We report a case of streptococcal tricuspid valve endocard itis in a patient with no history of intravenous drug abuse. Echocardiography revealed large vegetation on the septal cusp and complicating a ventricular septal defect. The evolution was very rapid and the patient died at 48 hours because of respiratory and heart failure with breathlessness and rebel septic shock. Key Words : Tricuspid valve endocarditis, vegetation, ventricular septal defect, streptococcus INTRODUCTION Electrocardiographic showed a regular sinusal tachycardia and a right bundle block. The chest X- Tricuspid valve endocarditis (TVE) accounts for Ray film showed cardiomegaly with opacity in the 5% to 10% of all cases of infective endocarditis right upper lung field. Transthoracic and and most commonly occurs in intra venous drug transesophageal echocardiography showed very users. Congenital cardiac lesions associated with mobile vegetation attached to the septal cusp of the left to right shunt (ventricular septal defect and tricuspid valve and an important tricuspid patent ductus arteriosus) also predispose to TVE. regurgitation. The vegetation was especially large We report a case of streptococcal tricuspid valve with a diameter of 19*13mm.This endocarditis endocarditis associated with large vegetation in a complicated an asymptomatic ventricular septal non drug addict patient in whom we found a defect partially closed by a membranous fortuitous ventricular septal defect. pseudoaneurysm (fig 1). -
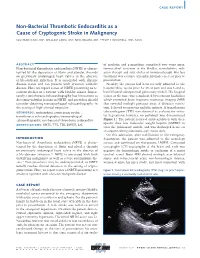
Non-Bacterial Thrombotic Endocarditis As a Cause of Cryptogenic Stroke in Malignancy
CASE REPORT Non-Bacterial Thrombotic Endocarditis as a Cause of Cryptogenic Stroke in Malignancy SULEMAN ILYAS, MD; WILLIAM LANG, MD; NEEL BELANI, MD; PHILIP STOCKWELL, MD, FACC 63 66 EN ABSTRACT of cisplatin and gemcitabine completed two years prior, Non-bacterial thrombotic endocarditis (NBTE) is charac- transurethral resection of the bladder, consolidative radi- terized by the deposition of fibrin and platelet thrombi ation therapy and four cycles of immunotherapy. His last on previously undamaged heart valves in the absence treatment was a course of pembrolizumab, one year prior to of bloodstream infection. It is associated with chronic presentation. disease states and can present with systemic embolic Notably, the patient had been recently admitted to the disease. Here we report a case of NBTE presenting as re- hospital three weeks prior for chest pain and was found to current strokes in a patient with bladder cancer. Impor- have bilateral subsegmental pulmonary emboli. His hospital tantly, transthoracic echocardiography has limitations to course at the time was complicated by recurrent headaches detecting valvular lesions in NBTE, and providers should which prompted brain magnetic resonance imaging (MRI) consider obtaining transesophageal echocardiography in that revealed multiple punctate areas of diffusion restric- the setting of high clinical suspicion. tion, believed to represent embolic infarcts. A transthoracic KEYWORDS: endocarditis; cryptogenic stroke; echocardiogram (TTE) was obtained to evaluate for valvu- transthoracic echocardiography; transesophageal lar vegetations; however, no pathology was demonstrated echocardiography; non-bacterial thrombotic endocarditis (Figure 1). The patient received anticoagulation with ther- apeutic dose low molecular weight heparin (LMWH) to ABBREVIATIONS: NBTE; TTE; TEE; LMWH; LSE treat the pulmonary emboli, and was discharged home on enoxaparin 80 mg subcutaneously twice daily.