Unique Mitral Valve Mass: Think Beyond Vegetation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Infective Endocarditis in Neonates
Arch Dis Child: first published as 10.1136/adc.63.1.53 on 1 January 1988. Downloaded from Archives of Disease in Childhood, 1988, 63, 53-57 Infective endocarditis in neonates C O'CALLAGHAN AND P MCDOUGALL Department of Neonatology, Royal Children's Hospital, Melbourne, Australia SUMMARY Five patients with neonatal infective endocarditis were reviewed, two of whom survived. Infection was caused by Staphylococcus aureus in four and by Candida albicans in one. All cases of bacterial endocarditis had clinical signs of septicaemia, positive blood cultures, thrombocytopenia, microscopic haematuria, and heart murmurs. Three developed skin abscesses early in their illnesses. Three patients had two dimensional echocardiographic studies that showed bacterial vegetations. One of these studies was done before the heart murmur could be heard. We suggest that echocardiography in conjunction with the clinical picture described may help in making an early diagnosis of endocarditis in neonates. Bacterial endocarditis in neonates is a rare and and tracheal aspirates; he was treated with intra- usually fatal disease; the first survivor was reported venous vancomycin. in 1983.1 2We became interested in the disease after At 26 days of age the baby had not improved and two patients in our neonatal unit survived. We a systolic murmur could be heard. Echocardio- therefore reviewed all five cases of neonatal infec- graphy showed vegetation round the mitral valve. tive endocarditis seen at this hospital over the past Despite the addition of fusidic acid to his treatment 10 years to see if we could find similarities that could he continued to deteriorate and died at 28 days. -

Refractory Chest Pain Or Treating Cardiologist’S Bane: a Case Report
THIEME Case Report 49 Refractory Chest Pain or Treating Cardiologist’s Bane: A Case Report Anupama V. Hegde1 Abhinay Tibdewal1 Vadagenalli S. Prakash1 Sarthak Sahoo1 1 Department of Cardiology, M. S. Ramaiah Medical College and Address for correspondence Anupama V. Hegde, MBBS, DNB Hospitals, Bengaluru, Karnataka, India (Medicine), DNB (Cardiology), Department of Cardiology, M. S. Ramaiah Medical College and Hospitals, Bengaluru 560054, Indian J Cardiovasc Dis Women-WINCARS 2017;2:49–53. Karnataka, India (e-mail: [email protected]). Abstract Microvascular angina is caused by dysfunction of small-resistance coronary arteries (< 500 µm) and is of heterogenous origin. The major epicardial coronaries are normal and commonly seen in women. Prognosis is variable, with disabling angina in many patients and can be a cause of mortality, especially in those who are refractory to Keywords treatment. In this background, we present a case of 56-year-old post valve replacement ► aortic valve with normally functioning aortic valve and recurrent episodes of microvascular angina. The replacement patient had normal epicardial coronaries. She had recurrent episodes of angina refractory ► coronary to various antianginals associated with hemodynamic instability. Microvascular angina angiography can curtail routine activity, frequent hospitalization, and repeated noninvasive and invasive ► microvascular angina investigations. Thus, it is a high social and economical disease, especially pertinent to ► refractory chest pain women. Introduction induced angina and normal coronary angiograms. However, the use of this term has not always been limited to this specific The first mention of chest pain with normal coronaries was meaning.4 made in 1981 by Opherk and coworkers.1 Among patients undergoing coronary angiography (CAG) for ischemic signs Case Report and symptoms, approximately10 to 30%have angiographically normal coronaries. -

Left Atrial Vegetation After Pulmonary Vein Isolation Sean Gaine,1 John Joseph Coughlan ,2 Richard Szirt,3 Sadat Ali Edroos 4
Images in… BMJ Case Rep: first published as 10.1136/bcr-2020-235833 on 17 August 2020. Downloaded from Left atrial vegetation after pulmonary vein isolation Sean Gaine,1 John Joseph Coughlan ,2 Richard Szirt,3 Sadat Ali Edroos 4 1Cardiology, St James’s Hospital, DESCRIPTION Dublin, Ireland A- 67- year old man presented with acute left hemi- 2 Cardiology, University Hospital paresis 6 weeks after pulmonary vein isolation Limerick, Limerick, Ireland (PVI) for atrial fibrillation. His medical history 3Department of Cardiology, St was notable for hypertension and a metallic aortic George Hospital, Kogarah, New South Wales, Australia valve which was implanted 23 years previously for 4St James’s Hospital, Dublin, bicuspid aortic stenosis. He was warfarinised for his Ireland metallic valve and his warfarin had been suspended for 5 days prior to ablation. Correspondence to Clinical examination demonstrated left upper Dr Sean Gaine; sgaine@ tcd. ie and lower limb weakness. CT brain suggested right Figure 2 Gated cardiac CT confirming the presence of middle cerebral artery branch occlusion. His inter- the vegetation in proximity to the oesophagus. It did not Accepted 29 June 2020 national normalised ratio was high at 4.6 ruling find any evidence of an atrio- oesophageal fistula (black out thrombolysis. The hemiparesis resolved within arrow). hours, and he was admitted for observation. He deteriorated the next day with bilateral weakness of left lower and right upper limbs. Following seizure to permit long- term antibiotics in the context of activity, the patient dropped his Glasgow Coma sepsis, prior to committing to a permanent device. Scale and required intubation. -

Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use
Otterbein University Digital Commons @ Otterbein Nursing Student Class Projects (Formerly MSN) Student Research & Creative Work Summer 7-30-2018 Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use Kaleigh Cline Otterbein University, [email protected] Follow this and additional works at: https://digitalcommons.otterbein.edu/stu_msn Part of the Cardiovascular Diseases Commons, and the Nursing Commons Recommended Citation Cline, Kaleigh, "Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use" (2018). Nursing Student Class Projects (Formerly MSN). 286. https://digitalcommons.otterbein.edu/stu_msn/286 This Project is brought to you for free and open access by the Student Research & Creative Work at Digital Commons @ Otterbein. It has been accepted for inclusion in Nursing Student Class Projects (Formerly MSN) by an authorized administrator of Digital Commons @ Otterbein. For more information, please contact [email protected]. Pathophysiology of Infective Endocarditis (IE) Associated with Intravenous Drug Use Kaleigh Cline BSN, RN Otterbein University, Westerville, Ohio Underlying Pathophysiology Significance of Pathophysiology Conclusion Introduction Underlying Lesion: Degenerative processes such as fibrosis, calcification, congenital heart diseases, mechanical IE is a significant diagnosis because of its ability to affect almost every vital body system. lesions secondary to material implantation, and turbulent blood flows (IVDU) causes endocardial • Infective Endocarditis is a •Intravenous drug use (IVDU) poses many risks to those who use them. One of damage. This then exposes the extracellular matrix and results in apoptosis of endocardial cells which • Heart Failure - Heart failure is the most common complication from IE and can often leads to surgical serious condition associated that the risks being infective endocarditis. then produces tissue factor and a non-bacterial thrombus formation. -

Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism
ASE GUIDELINES AND STANDARDS Guidelines for the Use of Echocardiography in the Evaluation of a Cardiac Source of Embolism Muhamed Saric, MD, PhD, FASE, Chair, Alicia C. Armour, MA, BS, RDCS, FASE, M. Samir Arnaout, MD, Farooq A. Chaudhry, MD, FASE, Richard A. Grimm, DO, FASE, Itzhak Kronzon, MD, FASE, Bruce F. Landeck, II, MD, FASE, Kameswari Maganti, MD, FASE, Hector I. Michelena, MD, FASE, and Kirsten Tolstrup, MD, FASE, New York, New York; Durham, North Carolina; Beirut, Lebanon; Cleveland, Ohio; Aurora, Colorado; Chicago, Illinois; Rochester, Minnesota; and Albuquerque, New Mexico Embolism from the heart or the thoracic aorta often leads to clinically significant morbidity and mortality due to transient ischemic attack, stroke or occlusion of peripheral arteries. Transthoracic and transesophageal echo- cardiography are the key diagnostic modalities for evaluation, diagnosis, and management of stroke, systemic and pulmonary embolism. This document provides comprehensive American Society of Echocardiography guidelines on the use of echocardiography for evaluation of cardiac sources of embolism. It describes general mechanisms of stroke and systemic embolism; the specific role of cardiac and aortic sour- ces in stroke, and systemic and pulmonary embolism; the role of echocardiography in evaluation, diagnosis, and management of cardiac and aortic sources of emboli including the incremental value of contrast and 3D echocardiography; and a brief description of alternative imaging techniques and their role in the evaluation of cardiac sources of emboli. Specific guidelines are provided for each category of embolic sources including the left atrium and left atrial appendage, left ventricle, heart valves, cardiac tumors, and thoracic aorta. In addition, there are recommen- dation regarding pulmonary embolism, and embolism related to cardiovascular surgery and percutaneous procedures. -

Tricuspid Valve Endocarditis with Large Vegetation in a Non Drug Addict Patient
Cas Clinique TRICUSPID VALVE ENDOCARDITIS WITH LARGE VEGETATION IN A NON DRUG ADDICT PATIENT L. ABID, L. LAROUSSI, S. CHTOUROU, CH. HAMZA, S KRICHÈNE, D. ABID, M. AKROUT, S. MALLEK, F. TRIKI, M. HENTATI, S. KAMMOUN Cardiology department, Hedi Chaker hospital, Sfax University -Tunisia Summary We report a case of streptococcal tricuspid valve endocard itis in a patient with no history of intravenous drug abuse. Echocardiography revealed large vegetation on the septal cusp and complicating a ventricular septal defect. The evolution was very rapid and the patient died at 48 hours because of respiratory and heart failure with breathlessness and rebel septic shock. Key Words : Tricuspid valve endocarditis, vegetation, ventricular septal defect, streptococcus INTRODUCTION Electrocardiographic showed a regular sinusal tachycardia and a right bundle block. The chest X- Tricuspid valve endocarditis (TVE) accounts for Ray film showed cardiomegaly with opacity in the 5% to 10% of all cases of infective endocarditis right upper lung field. Transthoracic and and most commonly occurs in intra venous drug transesophageal echocardiography showed very users. Congenital cardiac lesions associated with mobile vegetation attached to the septal cusp of the left to right shunt (ventricular septal defect and tricuspid valve and an important tricuspid patent ductus arteriosus) also predispose to TVE. regurgitation. The vegetation was especially large We report a case of streptococcal tricuspid valve with a diameter of 19*13mm.This endocarditis endocarditis associated with large vegetation in a complicated an asymptomatic ventricular septal non drug addict patient in whom we found a defect partially closed by a membranous fortuitous ventricular septal defect. pseudoaneurysm (fig 1). -
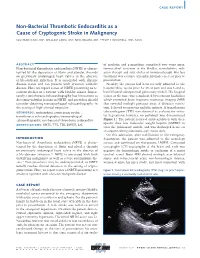
Non-Bacterial Thrombotic Endocarditis As a Cause of Cryptogenic Stroke in Malignancy
CASE REPORT Non-Bacterial Thrombotic Endocarditis as a Cause of Cryptogenic Stroke in Malignancy SULEMAN ILYAS, MD; WILLIAM LANG, MD; NEEL BELANI, MD; PHILIP STOCKWELL, MD, FACC 63 66 EN ABSTRACT of cisplatin and gemcitabine completed two years prior, Non-bacterial thrombotic endocarditis (NBTE) is charac- transurethral resection of the bladder, consolidative radi- terized by the deposition of fibrin and platelet thrombi ation therapy and four cycles of immunotherapy. His last on previously undamaged heart valves in the absence treatment was a course of pembrolizumab, one year prior to of bloodstream infection. It is associated with chronic presentation. disease states and can present with systemic embolic Notably, the patient had been recently admitted to the disease. Here we report a case of NBTE presenting as re- hospital three weeks prior for chest pain and was found to current strokes in a patient with bladder cancer. Impor- have bilateral subsegmental pulmonary emboli. His hospital tantly, transthoracic echocardiography has limitations to course at the time was complicated by recurrent headaches detecting valvular lesions in NBTE, and providers should which prompted brain magnetic resonance imaging (MRI) consider obtaining transesophageal echocardiography in that revealed multiple punctate areas of diffusion restric- the setting of high clinical suspicion. tion, believed to represent embolic infarcts. A transthoracic KEYWORDS: endocarditis; cryptogenic stroke; echocardiogram (TTE) was obtained to evaluate for valvu- transthoracic echocardiography; transesophageal lar vegetations; however, no pathology was demonstrated echocardiography; non-bacterial thrombotic endocarditis (Figure 1). The patient received anticoagulation with ther- apeutic dose low molecular weight heparin (LMWH) to ABBREVIATIONS: NBTE; TTE; TEE; LMWH; LSE treat the pulmonary emboli, and was discharged home on enoxaparin 80 mg subcutaneously twice daily. -
Recommendations for the Practice of Echocardiography in Infective Endocarditis
European Journal of Echocardiography (2010) 11, 202–219 RECOMMENDATIONS doi:10.1093/ejechocard/jeq004 Recommendations for the practice of echocardiography in infective endocarditis Gilbert Habib (France)*, Luigi Badano (Italy), Christophe Tribouilloy (France), Isidre Vilacosta (Spain), and Jose Luis Zamorano (Spain) Scientific Committee: Maurizio Galderisi (Italy), Jens-Uwe Voigt (Belgium), Rosa Sicari (Italy) Document Reviewers: Bernard Cosyns (Belgium), Kevin Fox (UK), Svend Aakhus (Norway) On behalf of the European Association of Echocardiography Service de Cardiologie, CHU La Timone, Bd Jean Moulin, 13005 Marseille, France Received 20 December 2009; accepted after revision 30 December 2009 Echocardiography plays a key role in the assessment of infective endocarditis (IE). It is useful for the diagnosis of endocarditis, the assessment of the severity of the disease, the prediction of short- and long-term prognosis, the prediction of embolic events, and the follow-up of patients under specific antibiotic therapy. Echocardiography is also useful for the diagnosis and management of the complications of IE, helping the physician in decision-making, particularly when a surgical therapy is considered. Finally, intraoperative echocardiography must be performed in IE to help the surgeon in the assessment and management of patients with IE during surgery. The current ‘recommendations for the practice of echocardiography in infective endocarditis’ aims to provide both an updated summary concerning the value and limitations of echocardiography in IE, and clear and simple recommendations for the optimal use of both transthoracic and transoesophageal echocardiography in IE. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Echocardiography † Endocarditis † Valve disease Table of Contents Introduction . 202 2. Echocardiographic follow-up under therapy . 212 Chapter 1: Echocardiography for the diagnosis of infective 3. -

Happyo Ozawa.Pdf
Advance Publication by-J-STAGE Circ J IMAGES IN CARDIOVASCULAR MEDICINE doi: 10.1253/circj.CJ-18-0632 genital and gastrointestinal tracts, frequently can lead to Infective Endocarditis Involving Mitral serious neonatal infections. Recently, invasive infections Annular Calcification Leading to Abscess due to Streptococcus agalactiae in aged adults have been reported. Although MAC has been considered a relatively Formation Rupture Into Pericardium benign pathology of the elderly, it has also recently been reported as an underestimated predisposing factor and 2 Takaya Ozawa, MD; Shoji Kawakami, MD, PhD; poor predictor for IE. Streptococcus agalactiae and MAC Manabu Matsumoto, MD, PhD; should not be ignored in aged patients with IE. Hatsue Ishibashi-Ueda, MD, PhD; Toshiyuki Nagai, MD, PhD; Disclosures Teruo Noguchi, MD, PhD; The authors declare no conflicts of interest. Satoshi Yasuda, MD, PhD References . 1 Bashore TM, Cabell C, Fowler V Jr. Update on infective 87-year-old woman presented with Streptococcus endocarditis. Curr Probl Cardiol 2006; 31: 274 – 352. 2. Wentzell S, Nair V. Rare case of infective endocarditis involving agalactiae bacteremia and mobile vegetation mitral annular calcification leading to hemopericardium and A attached to mitral annular calcification (MAC) of sudden cardiac death: A case report. Cardiovasc Pathol 2017; 33: the posterior mitral valve (Figure). Despite intensive care, 16 – 18. she died due to cardiac tamponade on the fourth day. Autopsy indicated vegetation of the posterior mitral valve and perivalvular abscess superimposed on MAC, Received May 28, 2018; revised manuscript received August 18, 2018; with the abscess penetrating into the pericardial cavity, accepted September 26, 2018; released online October 23, 2018 causing hemopericardium (Figure). -

CARDIAC INFECTIONS Rheumatic Heart Disease and Infective Endocarditis
CARDIAC INFECTIONS Rheumatic Heart Disease and Infective Endocarditis Jonas D. Del Rosario, MD, FPPS, FPCC Clinical Associate Professor UP College of Medicine RHEUMATIC FEVER RHEUMATIC HEART DISEASE RF to RHD “Rheumatic Fever is a disease the LICKS the joints but BITES heart.” RHD IS THE MOST SERIOUS COMPLICATION OF RF Rheumatic Fever • Most common cause of acquired heart disease in children & young adults worldwide • Diffuse inflammation of connective tissues of heart, joints, brain, blood vessels & subcutaneous tissues • Rheumatic process causes fibrosis of heart valves leading to RHD Epidemiology • Incidence of RF and RHD has not decreased in developing countries • Rheumatic Fever is principally a disease of childhood, with a median age of 10 years, although is also occurs in adults • Remains a major cause of morbidity and mortality in country Acute Rheumatic Fever Age and Sex Distribution ( N = 117 ) Frequency 30 25 20 Male 15 Female 10 5 0 Age <2 2-3 4-5 6-7 8-9 10-11 12-13 14-15 >16 Years PGH – Pedia 1986-90 Rheumatic Fever & Rheumatic Heart Disease Prevalence in school children: Developing countries 18.6 / 1000 Philippines 1971-1980 0.9 / 1000 1981-1990 0.6 / 1000 Developed countries USA 1971-1980 0.7 / 1000 Australia 1981-1990 12.3 / 1000 Group A β-Hemolytic Streptococcus (GAS) • Capsule – Non-antigenic • Cell wall – M-protein – Induces antibodies – Serotypes 5, 6, & 19 cross react with myosin Streptococcal Tonsillopharyngitis Pathophysiology • Rheumatic fever develops in some children and adolescents following PHARYNGITIS with -

Non-Infective Endocarditis
Education in Heart Heart: first published as 10.1136/heartjnl-2019-315204 on 6 May 2020. Downloaded from VALVULAR HEART DISEASES Non- infective endocarditis Harriet Hurrell, Ross Roberts-Thomson, Bernard D Prendergast ► Additional material is INTRODUCTION Learning objectives published online only. To view Endocarditis is defined as inflammation of the please visit the journal online endocardium, the lining of the cardiac chambers (http:// dx. doi. org/ 10. 1136/ To outline the causes and epidemiology of non- and valves, and characterised by vegetations, most ► heartjnl- 2019- 315204). infective endocarditis. commonly caused by infection with bacteria or To explore the pathophysiology of non- infective Department of Cardiology, St fungi. Non- infective endocarditis, also known as ► endocarditis. Thomas’ Hospital, London, UK non- bacterial thrombotic endocarditis (NBTE) To discuss the appropriate investigation or aseptic endocarditis, refers to a rare condi- ► Correspondence to of patients with suspected non- infective tion characterised by formation of sterile vegeta- Dr Harriet Hurrell, St Thomas’ endocarditis. Hospital Department of tions. Without treatment, these can lead to valve ► To highlight the key principles of management Cardiology, London, Greater dysfunction, heart failure, systemic embolism of non- infective endocarditis and when surgical London, UK; and death. Herein, we review the pathophysi- intervention should be considered. h. e. l. hurrell@ doctors. org. uk ology, clinical features, diagnosis and treatment Published -
Endocarditis
015Endocarditis // CONTENTS 140 Principles of Endocarditis 141 Native Valve Endocarditis 143 Complications of Native Valve Endocarditis 145 Right Heart Endocarditis 145 Prosthetic Valve Endocarditis 146 Pacemaker/Polymer-Associated Endocarditis 147 Non-Infective/Abacterial Endocarditis 148 Indications for Surgery 139 Alles_EchoFacts_140821_KD.indd 139 28.08.14 21:13 015 // ENDOCARDITIS NOTES PRINCIPLES OF ENDOCARDITIS The prevalence of Definition endocarditis associated with prothetic valves and Endovascular microbial infection of cardiovascular structures pacemaker leads is on the increase. Location • Valves • Large intrathoracic vessels • Ventricular and atrial endocardium • Prosthetic material • Polymere associated structures (lines) • Eustachian valve TRICUSPID VALVE ENDOCARDITIS – apical four- chamber view RV optimized/2D Endocarditis with a large vegetation attached to the native tricuspid valve. Thickened leafl ets TV vegetation Vegetation is an infected Pathophysiology of Endocarditis mass attached to endocardial structures, such as valves or implanted intracardiac material. On 2D Embolism echo they frequently appear as oscillating structures of variable size Active infection and morphology. Endocardial defect Post endocarditis Non-significant Healing with Perforation endocardial lesion/ calcification/ fibrosis fibrosis/thickening Principle of a ”super-infected” thrombus: The endothelial lesion initiates a repair process which involves thrombus formation. In the presence of bacteremia this thrombus may be super-infected. Further consequences include repair ad integrum, tissue destruction, embolism, and defect healing. 140 Alles_EchoFacts_140821_KD.indd 140 28.08.14 21:13 015 // ENDOCARDITIS PRINCIPLES OF ENDOCARDITIS NOTES Microbiology Staph. aureus infection predisposes to abscess Other 14% formation and complications of Culture negative 17% Staph. aureus 25% endocarditis! Staph. epidermidis 13% Enterococcus 11% Strept. bovis 20% MITRAL VALVE ENDOCARDITIS AMVL – PLAX zoomed/2D A vegetation is attached to the tip of the anterior mitral valve leaflet.