4C. O&SC Work Programme May 17 Appx3 LBL Slam Trigger Template MHOA , Item 4. PDF
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Kjl MSATCALLS on HAWAI ARMY
Kamehameha irrsrlT 3:30 Pay Races 3fS TTrrvv nirffmr and Polo Editio 1 vn- 1 . PHR K FIVK KNTS i r.;r iiDNorri-i'- . tkkritoi.y or ii.wn. Trft A i iA yjj ww v Jl TCALLS ON HAWAI ARMY MEN (G k MSA ffiY OFFICERS M WAIIANS IN GREA T OUTPOURING PA Y TRIBUTE POSSIBLE SERVICE IN FRANCE TO MEMORY OF BELOVED RULER,. KAMEHAMEHA Oil PERMIT'S OR COMMAND ON MAINLAND IS STAFF IN PARIS IN SATURDAY NIGHT CABLEGRAM to Lord Northciiffe Comes LGEN. strong ordered to report to . war depart to Represent British America ment EVERY OFFICER WHO CAN BE SPARED FOR DUTY Mission; King George Honors In states ITIilllCU -- -- - U. O. J i w. ... -- C; a.," - The Associated Press ,"at Every army officer in the Hawaiian department who can been by - up , the be spared for duty in the United States has called the coon- today summed " r i day's events in the war zones t war department, the call to take effect at the earliest possi- as follows:. r, ble date. "The .British today, fought In a cablegram received Saturday evening, Brig. -- Gen. forward to a decided advance Frederick S. Strong, commanding the Hawaiian department, ' - - k, south of Messines and have re IV! , s ? was ordered to report as soon as possible the names of local sumed their strong ,l trench officers who are not imperatively needed for service in Hawaii 70-ini- ' v v le : ' big- "'tf. ; J ' I ' This Is regarded one of the raids along a front. - : v. .;,. " hv." r is Jiaye; launched gest orders that has been received at The Italians . -

Appointment Brief Chief Operating Officer August 2020
Appointment brief Chief Operating Officer August 2020 Introduction South London and Maudsley NHS Foundation Trust (SLaM) is an exceptional organisation. Everything we do as a Trust is to support people to recover from mental illness and to help them improve their lives. Benefitting from world-class research and innovation, award-winning services and a world-renowned brand, we are uniquely placed to provide the best possible services to our local communities and beyond. Our biggest asset is our passionate and highly skilled workforce, who are dedicated to providing the best quality care to the people who use our services, often in difficult circumstances. We have managed the many challenges that COVID-19 has presented with great success and this has only been possible through the hard work and commitment of our staff. We are pleased with our internal patient experience survey results, where 96% of respondents said they found staff kind and caring and 87% of respondents to the NHS Friends and Families Test said that they would recommend the Trust to their friends and families based on their experience of the services provided. Operating across more than 90 sites, including Bethlem Royal Hospital and Maudsley Hospital, we provide a staggering range of services, ranging from core mental health services to our local boroughs, and more than 50 specialist mental health services across the UK. We are rated ‘Good’ overall by the Care Quality Commission, including for the ‘Well Led’ domain. With our strong commitment to working in partnership with our service users, carers and local communities, and to quality improvement, we believe we are capable of delivering truly outstanding services across all our teams We know that we will only achieve this if SLaM truly is a great place to work, where all our staff feel valued, developed and supported. -

Annual Report and Financial Statements 2019 / 2020 the Maudsley Charity Is the Largest NHS Mental Health Charity in the United Kingdom
Annual Report and Financial Statements 2019 / 2020 The Maudsley Charity is the largest NHS mental health charity in the United Kingdom We back better mental health by working together with our partners, South London and Maudsley NHS Foundation Trust (SLaM) and King’s College London (KCL), two world-leading organisations, to deliver a vision that is genuinely enabling us to improve the lives of people with mental illness. Kairos Community Trust, a Maudsley Charity funded Community and Connection project. Mental Health In 2018 This means more than A snapshot of mental health in the UK provided there were 16 people per day took by the Mental Health Foundation their life 6,154 It is estimated that suicides in 10-25 times that number Great Britain. attempt suicide The UK has one of the highest 1 in 4 people experience self-harm rates mental health issues each year in Europe 1.25 million people in the UK have an eating disorder (1 in 50) and more than 1 in 7 young women(1) 30-50% Every year mental ill health costs the UK economy an of people 24% of women estimated £70bn in lost productivity at work, benefit with a severe and 13% of men payments and health care expenditure. That is more than mental illness double the cost of cancer, heart disease and stroke combined(2) also have in England are diagnosed with problems with depression in their lifetime substance use Source: Mental Health Foundation: https://mhfaengland.org/mhfa-centre/research-and-evaluation/mental-health-statistics/ (1) Micali, N. et al “The incidence of eating disorders in the -

Records of Patients in London Hospitals
RESEARCH GUIDE 35 - Records of Patients in London Hospitals CONTENTS Introduction Hospital Archives Guides to Hospital Records Lying In Hospitals Access to Patients Records Other sources of information about hospital patients Registers of patients in psychiatric hospitals Introduction Many of the monastic hospitals which had cared for the sick poor of medieval London were suppressed on the dissolution of the monasteries in the 1530s and 1540s. St. Bartholomew's Hospital, St. Thomas' Hospital, and Bethlem Royal Hospital were saved by the City of London Corporation, which obtained grants of the hospitals and their endowments from King Henry VIII and from his son, Edward VI. The hospitals were refounded as secular institutions, St. Bartholomew's and St. Thomas' caring for the physically sick and Bethlem for the insane. Over time they established their virtual independence from the City of London. Thomas Guy, a London publisher and bookseller, left the fortune which he made out of the South Sea Bubble, to found Guy's Hospital which opened in 1725. Other major London hospitals, including the Westminster, Royal London, Middlesex, and St. George's Hospitals, were established in the 18th century on the voluntary principle. Medical men gave their services free while wealthy subscribers gave money each year to support the hospitals, in return for which they gained a share in the government of the hospital and the right to nominate patients. Medical schools developed in association with the hospitals. Many categories of the sick, including pregnant women, the mentally ill, and patients suffering from incurable or infectious diseases were excluded from most hospitals. -

APPOINTMENTS. Child from Infancy up to the End of School Life
JANUARY, 1938 13 State now systematically supervises the health of the APPOINTMENTS. child from infancy up to the end of school life. The benefits reaped by the nation from these State Services are most impressive. Thus, in 1901-10, the infant mortality rate AS81STANT SECRETARY. was 125 ; in 1936, it was 59 per thousand live births. International Council OP Nurses, 51, Palace Street, Westminster, S.W.-Miss Margaret J. Matheson, S.R.N., by Examination, Venereal diseases fall on the just as well as on the unjust. March lSth, 1935, S.C.M., M.A. (Edin.) in Modem Languages, The Public Health (Venereal Diseases) Regulations, 1916, has been appointed Assistant Secretary. She was trained and directed each County and County Borough to set up a certificated 1931-1934 at St. Bartholomew’s Hospital, London, scheme for the treatment of venereal diseases. The work and at the Royal Maternity Hospital, Edinburgh, and has been has met and is meeting with success. Nursing Sister at the British Sanatorium, Montana, Switzerland. The establishment of the Ministry of Health in 1919 was MATRON. the outward expression of Parliamentary decision that Highgate Hcspital, Dattmouth Park HilI, London, N.19.- Miss the National Health is of supreme and vital importance. Constance A. Stanier, S.R.N., S.C.M., has been appointed Matron. A central authority was expressly created for the purpose She was trained at the Mile End Hospital, London, E., where she was Staff Nurse, Sister, Sister Tutor, and Home Sister, of supervising the health of the people as a whole, and for and at the East End Maternity Hospital, London. -

Slam Mental Health of Older Adults
Public Document Pack JOINT HEALTH OVERVIEW AND SCRUTINY COMMITTEE - SLAM MENTAL HEALTH OF OLDER ADULTS Date: MONDAY, 6 NOVEMBER 2017 at 7.00 pm Committee Room 1 Civic Suite Catford SE6 4RU Enquiries to: John Bardens Telephone: 0208 314 9976 MEMBERS Councillor Carole Bonner Councillor Jacqui Dyer Councillor Alan Hall Councillor Robert Hill Councillor Rebecca Lury Councillor John Muldoon Councillor Andy Stranack Councillor Bill Williams The public are welcome to attend our committee meetings, however occasionally committees may have to consider some business in private. Copies of reports can be made available in additional formats on request. Members are summoned to attend this meeting Barry Quirk Chief Executive Lewisham Town Hall Catford London SE6 4RU Date: 26 October 2017 The public are welcome to attend our committee meetings, however occasionally committees may have to consider some business in private. Copies of reports can be made available in additional formats on request. ORDER OF BUSINESS – PART 1 AGENDA Item Page No No 1. Appointing a Chair and Vice-Chair 2. Declarations of interest 1 - 3 3. Terms of reference 4 - 6 4. Mental health of older adults 7 - 26 5. Committee recommendations The public are welcome to attend our committee meetings, however occasionally committees may have to consider some business in private. Copies of reports can be made available in additional formats on request. Agenda Item 2 Joint Health Overview and Scrutiny Committee SLaM Mental Health of Older Adults Title Declaration of interests Contributor Chief Executive Item 2 Class Part 1 (open) 6 November 2017 Declaration of interests Members are asked to declare any personal interest they have in any item on the agenda. -

An Independent Investigation Into the Care and Treatment of Mr R
An Independent Investigation into the Care and Treatment of Mr R February 2012 A report for Undertaken by Niche Health & Social Care Consulting Contents 1.0 INTRODUCTION......................................................................................................................1 2.0 PURPOSE AND SCOPE OF INVESTIGATION ..............................................................................1 3.0 SUMMARY OF THE INCIDENT .................................................................................................1 4.0 CONDOLENCES TO THE FAMILY OF MR Q ...............................................................................3 5.0 ACKNOWLEDGEMENT OF PARTICIPANTS................................................................................3 6.0 TERMS OF REFERENCE............................................................................................................3 7.0 THE INDEPENDENT INVESTIGATION TEAM .............................................................................6 8.0 INVESTIGATION METHODOLOGY............................................................................................6 9.0 SOURCES OF INFORMATION...................................................................................................9 10. CHRONOLOGY......................................................................................................................10 11.0 REVIEW OF THE MENTAL HEALTH CARE AND TREATMENT PROVIDED BY THE TRUST TO MR R FROM HIS FIRST CONTACT TO THE TIME OF THE OFFENCE AND THE SUITABILITY OF -
Everything We Do Is to Improve the Lives of the People and Communities We Serve and to Promote Mental Health and Wellbeing for All
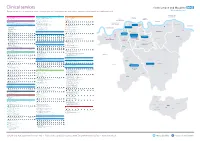
Clinical services Everything we do is to improve the lives of the people and communities we serve and to promote mental health and wellbeing for all No. Borough Clinical Academic Group No. Borough Clinical Academic Group No. Borough Clinical Academic Group Bexley Lambeth Southwark 1 Drug and Alcohol Service (Bexley) - 01322 357 940 Addictions 29 Psychosis Promoting Recovery (Lambeth South) - 020 3228 8100 Psychosis 55 Drug and Alcohol Service (Southwark) - 020 3228 9400 Addictions Drug Intervention Programme (Bexley) - 01322 357 940 South Asian Community Mental Health Service (Lambeth) - 020 3228 8100 151 Blackfriars Road, London SE1 8EL Erith Health Centre, 50 Pier Road, Erith DA8 1AT 380 Streatham High Road, London SW16 6HP Southwark Erith Streatham 56 Smoking Service - 020 3228 3848 30 Placements Assessments Monitoring Services - 020 3228 7000 Marina House, 63-65 Denmark Hill, London SE5 8RS Bromley Social Inclusion, Hope and Recovery Project (Lambeth) - 020 3228 7050 Denmark Hill 308 - 312 Brixton Road, London SW9 6AA 2 Bethlem Royal Hospital 57 Forensic Community Service (Southwark) - 020 3228 7168 Behavioural and Monks Orchard Road, Beckenham BR3 3BX Brixton Chaucer Resource Centre, 13 Ann Moss Way, London SE16 2TH Developmental Psychiatry 31 Psychosis Promoting Recovery (Lambeth Central) - 020 3228 6940 Eden Park West Wickham Bromley South then bus 119 East Croydon then bus 119, 194 or 198. Canada Water Surrey Quays Psychosis Promoting Recovery (Lambeth North East) - 020 3228 6940 A bus service runs between Bethlem and Maudsley -

2Nd Despatch
Page 1 Agenda Item 4 JHOSC JHOSC 4: SessionFeedbackandRecommendations Consultation Health Services for Lambeth Services for Health Improving Inpatient Mental Mental Inpatient Improving Page 2 Purpose 2 What we are going to cover 1) Scope of the Consultation A brief refresher of the scope of the public consultation 2) Feedback Report and Key Metrics Key metrics arising from the independent analysis of the consultation feedback 3) Key Feedback Themes and Recommendations Page 3 The main themes that were raised within the consultation, our assessment of those areas and recommendations where appropriate 4) The Decision Making Process An overview of the decision making process and recommendations for the Lambeth Together Strategic Board 5) Further Considerations Arising from the Consultation Key issues raised that are outside of the direct scope of the public consultation but of importance to the be followed through Section 1: Page 4 Consultation Scope 4 Scope of the Consultation • The public consultation The public consultation which ran from March 4th 2020 to May 31st looked at the future of adult acute inpatient wards and a psychiatric intensive care unit currently located at the Lambeth Hospital and proposed two options. • Option 1: Remain as we are (do nothing) • Option 2: [Preferred] Relocate four acute wards and the Psychiatric Intensive Care Unit (PICU) to the Maudsley site • Other engagement not within the scope of the public consultation To ensure that Members had a clear view of the broader programme of changes outside the scope -

Visiting Professional Programme: Clinical Genetics Visiting Professional Programme – Clinical Genetics 1
Visiting Professional Programme: Clinical Genetics Visiting Professional Programme – Clinical Genetics 1 Introduction The Guy’s and St Thomas’ NHS Foundation Trust Clinical Genetics Visiting Professional Programme (VPP) is designed to provide international visiting professionals with the opportunity to experience our highly acclaimed genetics department first hand. The programme is a unique chance to be fully integrated within a genetics service which is at the forefront of clinical activity, training and research; regional genetics clinics offer services to diagnose and assess the risk of families inheriting a genetic condition; the genetic counselling service involves explanation and risk assessment with any available options for family members, the genetics clinic is part of the Division of Medical and Molecular Genetics at King’s College London and we also take part in the 10,000 Genomes Project which focuses on cancer and rare diseases. Our Genetics department is divided into a range of specialist or multidisciplinary services and clinics including: Bardet Biedl Syndrome, BRCA family services, Breast cancer risk assessment, Connective tissue disorder, Dermatology (cancer), Dermatology (general), Endocrine, Eye genetics, Fetal cardiology, Fetal medicine unit (FMU), Sickle cell and thalassaemia, Haemophilia genetics, Huntington's disease, Inherited Cardiac Conditions, Metabolic, Myotonic dystrophy, Neurofibromatosis (NF1 and NF2), Paediatric neurology/genetics, Pre-implanation genetic diagnosis (PGD), Pre-natal diagnostic service, Rapid access, Skeletal dysplasia, Tay Sachs, Von Hippel Lindau (VHL) and Xeroderma Pigmentosa (XP). We offer specialised visiting professional programmes within all of our services for those that wish to hone their expertise in a subspecialty area of interest in genetics. Alternatively visitors may apply to rotate throughout our genetics department and we even offer the opportunity for visitors to gain professional certification depending of the duration of their stay. -

Arts in Mind Festival Review
Contents Foreword 1 Introduction 2 Brain & mind #MagicCarpet 4 Losing One’s Sense of Self 6 Cerebral City 8 Narrating Plasticity 10 We Cannot Unsee 12 Mental illness, contemporary society & environment Urban Mind 14 MONSTER 16 Without Touch 18 Kitchen Revolution Supper Club 19 Addiction Unconditional 20 Heroin Bodies 22 Psychosis Talking Heads 24 Is it ‘Normal’ to be Psychotic? 26 Illusions 28 Mood & anxiety – local & global Sound Mind 30 DIE OR RUN 32 Headtrip 33 Weaving a New Story 34 Maternal Journal 36 Creative Arts Hub Zimbabwe 38 Carl Campbell’s Recycled Teenagers 40 Festival 2018 My Memory Forest 42 Chromotrope 43 Festival feedback 44 Postscript 46 Acknowledgments 48 Audience feedback ‘I think that the Festival will make me more aware of Foreword my actions and more understanding towards others [with psychotic symptoms] and how they act… because of being talked through a real-life experience.’ The symbiosis between arts and health is an area of growing interest for researchers and has long been part of our DNA at King’s College London. In 2001, King’s became the first university in the UK to create a D’Oyly Carte Chair of Medicine ‘I’m a fifth-year medic interested in psychiatry and and the Arts. Since that point, King’s has developed a distinctive approach neuroscience. Hearing about psychiatric topics from to working in partnership with artists and cultural organisations to consider all these different perspectives… helps me set goals research questions and to share findings in imaginative and accessible ways. regarding the ideal standards I want to achieve in Over recent years, researchers in our medical faculties have been engaged my career.’ in a number of collaborations with artists and cultural organisations through the university's Arts in Health programme. -
Other Hospitals at Which Clinical Instruction Is Given
Othek Special Hospitals. Bethlem Royal Hospital. National Hospital for the Paralysed and Epileptic, Queen's Square. Central London Throat and Ear Hospital, Gray's Inn Road. St. Peter's Hospital for Stone and Urinary Diseases, Co vent Garden. St. John's Hospital for Diseases of the Skin, 49, Leicester Square. OTHER HOSPITALS AT WHICH CLINICAL INSTRUCTION IS GIVEN. In addition to the regular medical schools mentioned above, many hospitals offer opportunities for clinical instruction, and students will do well in their fifth year to widen their clinical experience by resorting to some of them. It should be noted that several of the special hospitals have instituted more or less complete courses of lectures on their special subjects. It is especially desirable that students should obtain a good knowledge of those fevers which are excluded from the wards at general hospital*. For this purpose the hospitals of the Metropolitan Asylums Board are available. Apply at the offices, Norfolk Street, Strand. The following are a few of the hospitals in London open for clinical work :? General Hospitals. Great Northern Central Hospital. London Temperance Hospital. Seamen's Hospitals: The Dreadnought Hospital, Greenwich, and the Branch Hospital, Victoria and Albert Docks. WeBt London Hospital, Hammersmith Road. Children's Hospitals. Hospital for Sick Children, Great Ormond Street. East London Hospital for Children, Shadwell. North-Eastern Hospital for Children, Hackney Road, Shoreditch. Ophthalmic Hospitals. Royal London Ophthalmic Hospital, Moorfields. Royal Westminster Ophthalmic Hospital, King William Street, Strand. Royal Eye Hospital, Southwark. Diseases of the Chest. Hospital for Consumption and Diseases of the Chest, JtJrompton. City.of London Hospital for Diseases of the Chest, Victoria Park.