Indolent Lymphoma in Dogs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Lymphoproliferative Disorders
Lymphoproliferative disorders Dr. Mansour Aljabry Definition Lymphoproliferative disorders Several clinical conditions in which lymphocytes are produced in excessive quantities ( Lymphocytosis) Lymphoma Malignant lymphoid mass involving the lymphoid tissues (± other tissues e.g : skin ,GIT ,CNS …) Lymphoid leukemia Malignant proliferation of lymphoid cells in Bone marrow and peripheral blood (± other tissues e.g : lymph nods ,spleen , skin ,GIT ,CNS …) Lymphoproliferative disorders Autoimmune Infection Malignant Lymphocytosis 1- Viral infection : •Infectious mononucleosis ,cytomegalovirus ,rubella, hepatitis, adenoviruses, varicella…. 2- Some bacterial infection: (Pertussis ,brucellosis …) 3-Immune : SLE , Allergic drug reactions 4- Other conditions:, splenectomy, dermatitis ,hyperthyroidism metastatic carcinoma….) 5- Chronic lymphocytic leukemia (CLL) 6-Other lymphomas: Mantle cell lymphoma ,Hodgkin lymphoma… Infectious mononucleosis An acute, infectious disease, caused by Epstein-Barr virus and characterized by • fever • swollen lymph nodes (painful) • Sore throat, • atypical lymphocyte • Affect young people ( usually) Malignant Lymphoproliferative Disorders ALL CLL Lymphomas MM naïve B-lymphocytes Plasma Lymphoid cells progenitor T-lymphocytes AML Myeloproliferative disorders Hematopoietic Myeloid Neutrophils stem cell progenitor Eosinophils Basophils Monocytes Platelets Red cells Malignant Lymphoproliferative disorders Immature Mature ALL Lymphoma Lymphoid leukemia CLL Hairy cell leukemia Non Hodgkin lymphoma Hodgkin lymphoma T- prolymphocytic -

Antibody Drug Conjugates in Lymphoma
Review: Clinical Trial Outcomes Nathwani & Chen Antibody drug conjugates in lymphoma 6 Review: Clinical Trial Outcomes Antibody drug conjugates in lymphoma Clin. Investig. (Lond.) Antibody drug conjugates (ADCs) are comprised of monoclonal antibodies physically Nitya Nathwani1 & Robert linked to cytotoxic molecules. They expressly target cancer cells by delivering cytotoxic Chen*,1 agents to cells displaying specific antigens, and minimize damage to normal tissue. The 1Department of Hematology & Hematopoietic Cell Transplantation, City efficacy and tolerability of these agents are primarily determined by the target antigen, of Hope, Duarte, CA, USA the cytotoxic agent and the linker connecting the cytotoxic agent to the monoclonal *Author for correspondence: antibody. Following advances in technology, clinical trials have demonstrated greater Tel.: +626 256 4673 (ext. 65298) efficacy for ADCs compared with the corresponding naked monoclonal antibodies. Fax: +626 301 8116 This review summarizes the features of current clinically active ADCs in lymphoma and [email protected] emphasizes recent clinical data elucidating the benefit of antibody-directed delivery of cytotoxic agents to tumor cells. Keywords: antibody drug conjugates • lymphoma • monoclonal antibodies Lymphoma is the most common hematologic concentration and poor performance status malignancy, and is subdivided into two main are adverse prognostic factors. SEER (Sur- types: Hodgkin lymphoma (HL) and non- veillance, Epidemiology and End Results) Hodgkin lymphoma (NHL). In the United data from the National Cancer Institute, States, there are an estimated 731,277 people 2013 has revealed a significant improvement 10.4155/CLI.14.73 living with or in remission from lymphoma. in survival rates in this group of diseases in In 2013, there were an estimated 79,030 new the last four decades. -
Arrhythmia Burden in Patients with Indolent Lymphoma
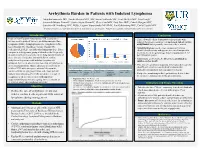
Arrhythmia Burden in Patients with Indolent Lymphoma Mujtaba Soniwala DO1, Saadia Sherazi MD1, MS, Susan Schleede MS1, Scott McNitt MS1, Tina Faugh2, Jeremiah Moore PharmD2, Justin Foster PharmD1, Clive Zent MD2, Paul Barr MD2, Patrick Reagan MD2, Jonathan W Friedberg MD2, MSSc, Eugene Storozynsky MD PhD1, Ilan Goldenberg MD1, Carla Casulo MD2 1Department of Medicine, University of Rochester School of Medicine and Dentistry; 2Wilmot Cancer Institute, University of Rochester Medical Center Introduction Results Conclusions Indolent Non-Hodgkin lymphomas (NHL) comprise a • This real-world cohort demonstrates that patients with heterogeneous group of diseases including marginal zone indolent lymphoma could have an increased risk of cardiac lymphoma (MZL), lymphoplasmacytic lymphoma (LPL), arrhythmias that is possibly exacerbated by treatment. small lymphocytic lymphoma/chronic lymphocytic • Atrial fibrillation was the most common arrhythmia leukemia (SLL/CLL), and follicular lymphoma (FL). These identified in this study and appears increased compared to compose a heterogenous group of disorders that frequently the incidence in the general age matched population (1-1.8 measures survival in years due to the long natural history of per 100 person-years). these diseases. Frequency and morbidity of cardiac • Surprisingly, of 80 deaths, 8 (10%) were attributed to arrhythmias in patients with indolent lymphoma is Arrhythmia Incidence Subtype of Indolent Lymphoma sudden cardiac death. unknown, but recent observations note that arrhythmias are • This data set contributes important information that can help an increasing problem. Due to advances in treatment for Arrhythmia incidence by CLL = 89 (53%) FL = 35 (21%) MZL = 27 (16%) LPL = 17 (10%) lymphoma subtype of total identify patients at increased risk of cardiovascular indolent NHL with emergence of novel therapeutics, (N = 168) Arrhythmia incidence Combination Targeted Therapy = Monoclonal Chemotherapy morbidity and mortality that can impact treatment. -

CD20-Negative Diffuse Large B-Cell Lymphomas: Biology and Emerging Therapeutic Options
Expert Review of Hematology ISSN: 1747-4086 (Print) 1747-4094 (Online) Journal homepage: http://www.tandfonline.com/loi/ierr20 CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options Jorge J Castillo, Julio C Chavez, Francisco J Hernandez-Ilizaliturri & Santiago Montes-Moreno To cite this article: Jorge J Castillo, Julio C Chavez, Francisco J Hernandez-Ilizaliturri & Santiago Montes-Moreno (2015) CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options, Expert Review of Hematology, 8:3, 343-354, DOI: 10.1586/17474086.2015.1007862 To link to this article: http://dx.doi.org/10.1586/17474086.2015.1007862 Published online: 01 Feb 2015. Submit your article to this journal Article views: 165 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ierr20 Download by: [North Shore Med Ctr], [Jorge Castillo] Date: 16 March 2016, At: 07:44 Review CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options Expert Rev. Hematol. 8(3), 343–354 (2015) Jorge J Castillo*1, CD20-negative diffuse large B-cell lymphoma (DLBCL) is a rare and heterogeneous group of Julio C Chavez2, lymphoproliferative disorders. Known variants of CD20-negative DLBCL include plasmablastic Francisco J lymphoma, primary effusion lymphoma, large B-cell lymphoma arising in human herpesvirus 8-associated multicentric Castleman disease and anaplastic lymphoma kinase-positive DLBCL. Hernandez-Ilizaliturri3 Given the lack of CD20 expression, atypical cellular morphology and aggressive clinical and Santiago 4 behavior characterized by chemotherapy resistance and inferior survival rates, CD20-negative Montes-Moreno DLBCL represents a challenge from the diagnostic and therapeutic perspectives. -

Drug Resistance in Non-Hodgkin Lymphomas
International Journal of Molecular Sciences Review Drug Resistance in Non-Hodgkin Lymphomas Pavel Klener 1,2,* and Magdalena Klanova 1,2 1 First Department of Internale Medicine-Hematology, University General Hospital in Prague, 128 08 Prague, Czech Republic; [email protected] 2 Institute of Pathological Physiology, First Faculty of Medicine, Charles University, Prague, 128 53 Prague, Czech Republic * Correspondence: [email protected] or [email protected] Received: 3 February 2020; Accepted: 15 March 2020; Published: 18 March 2020 Abstract: Non-Hodgkin lymphomas (NHL) are lymphoid tumors that arise by a complex process of malignant transformation of mature lymphocytes during various stages of differentiation. The WHO classification of NHL recognizes more than 90 nosological units with peculiar pathophysiology and prognosis. Since the end of the 20th century, our increasing knowledge of the molecular biology of lymphoma subtypes led to the identification of novel druggable targets and subsequent testing and clinical approval of novel anti-lymphoma agents, which translated into significant improvement of patients’ outcome. Despite immense progress, our effort to control or even eradicate malignant lymphoma clones has been frequently hampered by the development of drug resistance with ensuing unmet medical need to cope with relapsed or treatment-refractory disease. A better understanding of the molecular mechanisms that underlie inherent or acquired drug resistance might lead to the design of more effective front-line treatment algorithms based on reliable predictive markers or personalized salvage therapy, tailored to overcome resistant clones, by targeting weak spots of lymphoma cells resistant to previous line(s) of therapy. This review focuses on the history and recent advances in our understanding of molecular mechanisms of resistance to genotoxic and targeted agents used in clinical practice for the therapy of NHL. -

Non-Hodgkin Lymphoma
Non-Hodgkin Lymphoma Rick, non-Hodgkin lymphoma survivor This publication was supported in part by grants from Revised 2013 A Message From John Walter President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma Society (LLS) believes we are living at an extraordinary moment. LLS is committed to bringing you the most up-to-date blood cancer information. We know how important it is for you to have an accurate understanding of your diagnosis, treatment and support options. An important part of our mission is bringing you the latest information about advances in treatment for non-Hodgkin lymphoma, so you can work with your healthcare team to determine the best options for the best outcomes. Our vision is that one day the great majority of people who have been diagnosed with non-Hodgkin lymphoma will be cured or will be able to manage their disease with a good quality of life. We hope that the information in this publication will help you along your journey. LLS is the world’s largest voluntary health organization dedicated to funding blood cancer research, education and patient services. Since 1954, LLS has been a driving force behind almost every treatment breakthrough for patients with blood cancers, and we have awarded almost $1 billion to fund blood cancer research. Our commitment to pioneering science has contributed to an unprecedented rise in survival rates for people with many different blood cancers. Until there is a cure, LLS will continue to invest in research, patient support programs and services that improve the quality of life for patients and families. -

Relapsed Mantle Cell Lymphoma: Current Management, Recent Progress, and Future Directions
Journal of Clinical Medicine Review Relapsed Mantle Cell Lymphoma: Current Management, Recent Progress, and Future Directions David A Bond 1,*, Peter Martin 2 and Kami J Maddocks 1 1 Division of Hematology, The Ohio State University, Columbus, OH 43210, USA; [email protected] 2 Division of Hematology and Oncology, Weill Cornell Medical College, New York, NY 11021, USA; [email protected] * Correspondence: [email protected] Abstract: The increasing number of approved therapies for relapsed mantle cell lymphoma (MCL) provides patients effective treatment options, with increasing complexity in prioritization and se- quencing of these therapies. Chemo-immunotherapy remains widely used as frontline MCL treatment with multiple targeted therapies available for relapsed disease. The Bruton’s tyrosine kinase in- hibitors (BTKi) ibrutinib, acalabrutinib, and zanubrutinib achieve objective responses in the majority of patients as single agent therapy for relapsed MCL, but differ with regard to toxicity profile and dosing schedule. Lenalidomide and bortezomib are likewise approved for relapsed MCL and are active as monotherapy or in combination with other agents. Venetoclax has been used off-label for the treatment of relapsed and refractory MCL, however data are lacking regarding the efficacy of this approach particularly following BTKi treatment. Anti-CD19 chimeric antigen receptor T-cell (CAR-T) therapies have emerged as highly effective therapy for relapsed MCL, with the CAR-T treatment brexucabtagene autoleucel now approved for relapsed MCL. In this review the authors summarize evidence to date for currently approved MCL treatments for relapsed disease including Citation: Bond, D.A; Martin, P.; sequencing of therapies, and discuss future directions including combination treatment strategies Maddocks, K.J Relapsed Mantle Cell and new therapies under investigation. -

Mantle Cell Lymphoma
Leukemia (1998) 12, 1281–1287 1998 Stockton Press All rights reserved 0887-6924/98 $12.00 http://www.stockton-press.co.uk/leu Mantle cell lymphoma: a retrospective study of 121 cases H Samaha1, C Dumontet1, N Ketterer1, I Moullet1, C Thieblemont1, F Bouafia1, E Callet-Bauchu2, P Felman2, F Berger3, G Salles1 and B Coiffier1 1Service d’He´matologie, Centre Hospitalier Lyon-Sud, Hospices Civils de Lyon, and UPRES-JE 1879 ‘He´mopathies Lymphoides malignes’, Universite´ Claude Bernard, Pierre-Be´nite; 2Laboratoire d’He´matologie, Centre Hospitalier Lyon-Sud, Hospices Civils de Lyon, Pierre-Be´nite; and 3Laboratoire d’Anatomie Pathologique, Hoˆpital Edouard-Herriot, Hospices Civils de Lyon, France Mantle cell lymphoma (MCL) patients represent a difficult prob- phoma usually begins as a disseminated disease with wide- lem, sometimes to establish the diagnosis but mostly because spread involvement of lymph nodes, spleen, bone marrow of their refractoriness to standard lymphoma treatments. Which treatments to apply and to whom is not yet defined. In this and other extranodal sites, specially the gastrointestinal tract study, we attempted to analyze the clinical features, to identify and Waldeyer ring. However, patients usually present a good the major prognostic factors, and to evaluate the outcome of performance status (PS) at diagnosis although adverse prog- 121 MCL patients treated in our institution between 1979 and nostic factors, such as high serum lactic dehydrogenase (LDH) 1997. Clinical data, treatment modalities, and International and 2-microglobulin levels, may be present. Initially, these Prognostic Index (IPI) score were evaluated. Median age was 63 patients usually respond to different types of therapy, but years. -

Mantle Cell Lymphoma: Contemporary Diagnostic and Treatment Perspectives in the Age of Personalized Medicine
Himmelfarb Health Sciences Library, The George Washington University Health Sciences Research Commons Medicine Faculty Publications Medicine 9-1-2017 Mantle Cell Lymphoma: Contemporary Diagnostic and Treatment Perspectives in the Age of Personalized Medicine. Jose D Sandoval-Sus Eduardo M Sotomayor George Washington University Bijal D Shah Follow this and additional works at: https://hsrc.himmelfarb.gwu.edu/smhs_medicine_facpubs Part of the Medicine and Health Sciences Commons APA Citation Sandoval-Sus, J., Sotomayor, E., & Shah, B. (2017). Mantle Cell Lymphoma: Contemporary Diagnostic and Treatment Perspectives in the Age of Personalized Medicine.. Hematology/Oncology and Stem Cell Therapy, 10 (3). http://dx.doi.org/10.1016/ j.hemonc.2017.02.003 This Journal Article is brought to you for free and open access by the Medicine at Health Sciences Research Commons. It has been accepted for inclusion in Medicine Faculty Publications by an authorized administrator of Health Sciences Research Commons. For more information, please contact [email protected]. Hematol Oncol Stem Cell Ther (2017) 10,99– 115 Available at www.sciencedirect.com ScienceDirect journal homepage: www.elsevier.com/locate/hemonc Mantle Cell Lymphoma: Contemporary Diagnostic and Treatment Perspectives in the Age of Personalized Medicine Jose D. Sandoval-Sus a,*, Eduardo M. Sotomayor b, Bijal D. Shah a a Department of Malignant Hematology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA b Department of Hematology/Oncology, George Washington University, Washington, D.C., USA Received 6 October 2015; accepted 20 February 2017 Available online 6 April 2017 KEYWORDS Abstract Mantle cell lymphoma; Mantle cell lymphoma is a clinically heterogeneous disease occurring within a heterogeneous Prognosis; patient population, highlighting a need for personalized therapy to ensure optimal outcomes. -

REVIEW Anti-CD20-Based Therapy of B Cell Lymphoma: State of The
Leukemia (2002) 16, 2004–2015 2002 Nature Publishing Group All rights reserved 0887-6924/02 $25.00 www.nature.com/leu REVIEW Anti-CD20-based therapy of B cell lymphoma: state of the art C Kosmas1, K Stamatopoulos2, N Stavroyianni2, N Tsavaris3 and T Papadaki4 1Department of Medicine, 2nd Division of Medical Oncology, ‘Metaxa’ Cancer Hospital, Piraeus, Greece; 2Department of Hematology, G Papanicolaou General Hospital, Thessaloniki, Greece; 3Oncology Unit, Department of Pathophysiology, Athens University School of Medicine, Laikon General Hospital, Athens, Greece; and 4Hemopathology Department, Evangelismos Hospital, Athens, Greece Over the last 5 years, studies applying the chimeric anti-CD20 ficulties in identifying a completely tumor-specific target; (2) MAb have renewed enthusiasm and triggered world-wide appli- the impracticality of constructing a unique antibody for each cation of anti-CD20 MAb-based therapies in B cell non-Hodg- kin’s lymphoma (NHL). Native chimeric anti-CD20 and isotope- patient; (3) the development of an immune response to murine 6 labeled murine anti-CD20 MAbs are currently employed with immunoglobulins (human anti-mouse antibodies, HAMA). By encouraging results as monotherapy or in combination with the end of the 1980s enthusiasm for therapeutic MAbs was conventional chemotherapy and in consolidation of remission waning; murine native (unconjugated), radioactively labeled after treatments with curative intent (ie after/ in combination or toxin-conjugated MAbs failed to yield significant clinical with high-dose chemotherapy and hematopoietic stem cell responses; moreover, they were not uncommonly associated rescue). On the available experience, anti-CD20 MAb-based therapeutic strategies will be increasingly integrated in the with toxicities, predominantly in the form of serum sickness treatment of B cell NHL and related malignancies. -

Non-Hodgkin Lymphoma
Non-Hodgkin Lymphoma Tom, non-Hodgkin lymphoma survivor Support for this publication provided by Revised 2016 A Message from Louis J. DeGennaro, PhD President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma Society (LLS) is the world’s largest voluntary health organization dedicated to finding cures for blood cancer patients. Our research grants have funded many of today’s most promising advances; we are the leading source of free blood cancer information, education and support; and we advocate for blood cancer patients and their families, helping to ensure they have access to quality, affordable and coordinated care. Since 1954, we have been a driving force behind nearly every treatment breakthrough for blood cancer patients. We have invested more than $1 billion in research to advance therapies and save lives. Thanks to research and access to better treatments, survival rates for many blood cancer patients have doubled, tripled and even quadrupled. Yet we are far from done. Until there is a cure for cancer, we will continue to work hard—to fund new research, to create new patient programs and services, and to share information and resources about blood cancer. This booklet has information that can help you understand non-Hodgkin lymphoma, prepare your questions, find answers and resources, and communicate better with members of your healthcare team. Our vision is that, one day, all people with non-Hodgkin lymphoma will be cured or will be able to manage their disease so that they can experience a great quality of life. Today, we hope that our sharing of expertise, knowledge and resources will make a difference in your journey. -
Indolent Lymphoid Disorders Lazy Nothingness Or Incurable Lethality?
Indolent Lymphoid Disorders Lazy nothingness or incurable lethality? Michael Tees, MD, MPH Hematology ~ Blood and Marrow Therapies Colorado Blood Cancer Institute Objectives Identify that indolent lymphomas should be considered indolent lymphoid disorders Understand the mortality implications of the indolent lymphoid disorders depending on age, treatment, and other prognostic factors Understand the long-term outcomes after hematopoietic cell transplantation Indolent Lymphoid Disorders Review What is indolent? Disease management and implications Survival and factors affecting mortality Indolent Lymphoid Disorders Review What is indolent? Disease management and implications Survival and factors affecting mortality Hematologic Malignancies Hematologic Disease US Incidence, 2015 estimate Total 162,020 Myeloid Acute Myeloid Leukemia 20,830 Chronic Myeloid Leukemia 6,660 Plasma Cell 26,850 Lymphoid Acute Lymphocytic Leukemia 6,250 Hodgkin Lymphoma 9,050 Non-Hodgkin Lymphoma 71,850 Chronic Lymphocytic Leukemia 14,620 Source: American Cancer Society, 2015 Hematopoiesis HSC Lymphoid Myeloid NK B T Indolent Lymphoid Disorders Review What is indolent? Disease management and implications Survival and factors affecting mortality Hematologic Malignancies Hematologic Disease US Incidence, 2015 estimate Total 162,020 Myeloid Acute Myeloid Leukemia 20,830 Chronic Myeloid Leukemia 6,660 Plasma Cell 26,850 Lymphoid Acute Lymphocytic Leukemia 6,250 Hodgkin Lymphoma 9,050 Non-Hodgkin Lymphoma 71,850 Chronic Lymphocytic Leukemia 14,620 Source: American Cancer