Mantle Cell Lymphoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Lymphoma and Multiple Myeloma Center
The Lymphoma and Multiple Myeloma Center What Sets Us Apart We provide multidisciplinary • Experienced, nationally and internationally recognized physicians dedicated exclusively to treating patients with lymphoid treatment for optimal survival or plasma cell malignancies and quality of life for patients • Cellular therapies such as Chimeric Antigen T-Cell (CAR T) therapy for relapsed/refractory disease with all types and stages of • Specialized diagnostic laboratories—flow cytometry, cytogenetics, and molecular diagnostic facilities—focusing on the latest testing lymphoma, chronic lymphocytic that identifies patients with high-risk lymphoid malignancies or plasma cell dyscrasias, which require more aggresive treatment leukemia, multiple myeloma and • Novel targeted therapies or intensified regimens based on the other plasma cell disorders. cancer’s genetic and molecular profile • Transplant & Cellular Therapy program ranked among the top 10% nationally in patient outcomes for allogeneic transplant • Clinical trials that offer tomorrow’s treatments today www.roswellpark.org/partners-in-practice Partners In Practice medical information for physicians by physicians We want to give every patient their very best chance for cure, and that means choosing Roswell Park Pathology—Taking the best and Diagnosis to a New Level “ optimal front-line Lymphoma and myeloma are a diverse and heterogeneous group of treatment.” malignancies. Lymphoid malignancy classification currently includes nearly 60 different variants, each with distinct pathophysiology, clinical behavior, response to treatment and prognosis. Our diagnostic approach in hematopathology includes the comprehensive examination of lymph node, bone marrow, blood and other extranodal and extramedullary tissue samples, and integrates clinical and diagnostic information, using a complex array of diagnostics from the following support laboratories: • Bone marrow laboratory — Francisco J. -

Low-Grade Non-Hodgkin Lymphoma Book
Low-grade non-Hodgkin lymphoma Low-grade non-Hodgkin lymphoma Follicular lymphoma Mantle cell lymphoma Marginal zone lymphomas Lymphoplasmacytic lymphoma Waldenström’s macroglobulinaemia This book has been researched and written for you by Lymphoma Action, the only UK charity dedicated to people affected by lymphoma. We could not continue to support you, your clinical team and the wider lymphoma community, without the generous donations of our incredible supporters. As an organisation we do not receive any government or NHS funding and so every penny received is truly valued. To make a donation towards our work, please visit lymphoma-action.org.uk/Donate 2 Your lymphoma type and stage Your treatment Key contact Name: Role: Contact details: Job title/role Name and contact details GP Consultant haematologist/ oncologist Clinical nurse specialist or key worker Treatment centre 3 About this book Low-grade (or indolent) non-Hodgkin lymphoma is a type of blood cancer that develops from white blood cells called lymphocytes. It is a broad term that includes lots of different types of lymphoma. This book explains what low-grade non-Hodgkin lymphoma is and how it is diagnosed and treated. It includes tips on coping with treatment and dealing with day-to-day life. The book is split into chapters. You can dip in and out of it and read the sections that are relevant to you at any given time. Important and summary points are written in the chapter colour. Lists practical tips and chapter summaries. Gives space for questions and notes. Lists other resources you might find useful, some of which are online. -

Allogeneic Stem Cell Transplantation in Mantle Cell Lymphoma in the Era of New Drugs and CAR-T Cell Therapy
cancers Review Allogeneic Stem Cell Transplantation in Mantle Cell Lymphoma in the Era of New Drugs and CAR-T Cell Therapy Miriam Marangon 1, Carlo Visco 2 , Anna Maria Barbui 3, Annalisa Chiappella 4, Alberto Fabbri 5, Simone Ferrero 6,7 , Sara Galimberti 8 , Stefano Luminari 9,10 , Gerardo Musuraca 11, Alessandro Re 12 , Vittorio Ruggero Zilioli 13 and Marco Ladetto 14,15,* 1 Department of Hematology, Azienda Sanitaria Universitaria Giuliano Isontina, 34129 Trieste, Italy; [email protected] 2 Section of Hematology, Department of Medicine, University of Verona, 37134 Verona, Italy; [email protected] 3 Hematology Unit, ASST Papa Giovanni XXIII, 24127 Bergamo, Italy; [email protected] 4 Division of Hematology, Fondazione IRCCS, Istituto Nazionale dei Tumori, 20133 Milan, Italy; [email protected] 5 Hematology Division, Department of Oncology, Azienda Ospedaliero-Universitaria Senese, 53100 Siena, Italy; [email protected] 6 Hematology Division, Department of Molecular Biotechnologies and Health Sciences, Università di Torino, 10126 Torino, Italy; [email protected] 7 Hematology 1, AOU Città della Salute e della Scienza di Torino, 10126 Torino, Italy 8 Hematology Unit, Department of Clinical and Experimental Medicine, University of Pisa, 56126 Pisa, Italy; [email protected] 9 Hematology Unit, Azienda Unità Sanitaria Locale IRCCS di Reggio Emilia, 42123 Modena, Italy; [email protected] 10 Surgical, Medical and Dental Department of Morphological Sciences Related -

Antibody Drug Conjugates in Lymphoma
Review: Clinical Trial Outcomes Nathwani & Chen Antibody drug conjugates in lymphoma 6 Review: Clinical Trial Outcomes Antibody drug conjugates in lymphoma Clin. Investig. (Lond.) Antibody drug conjugates (ADCs) are comprised of monoclonal antibodies physically Nitya Nathwani1 & Robert linked to cytotoxic molecules. They expressly target cancer cells by delivering cytotoxic Chen*,1 agents to cells displaying specific antigens, and minimize damage to normal tissue. The 1Department of Hematology & Hematopoietic Cell Transplantation, City efficacy and tolerability of these agents are primarily determined by the target antigen, of Hope, Duarte, CA, USA the cytotoxic agent and the linker connecting the cytotoxic agent to the monoclonal *Author for correspondence: antibody. Following advances in technology, clinical trials have demonstrated greater Tel.: +626 256 4673 (ext. 65298) efficacy for ADCs compared with the corresponding naked monoclonal antibodies. Fax: +626 301 8116 This review summarizes the features of current clinically active ADCs in lymphoma and [email protected] emphasizes recent clinical data elucidating the benefit of antibody-directed delivery of cytotoxic agents to tumor cells. Keywords: antibody drug conjugates • lymphoma • monoclonal antibodies Lymphoma is the most common hematologic concentration and poor performance status malignancy, and is subdivided into two main are adverse prognostic factors. SEER (Sur- types: Hodgkin lymphoma (HL) and non- veillance, Epidemiology and End Results) Hodgkin lymphoma (NHL). In the United data from the National Cancer Institute, States, there are an estimated 731,277 people 2013 has revealed a significant improvement 10.4155/CLI.14.73 living with or in remission from lymphoma. in survival rates in this group of diseases in In 2013, there were an estimated 79,030 new the last four decades. -
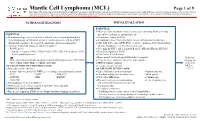
Mantle Cell Lymphoma (MCL)
Mantle Cell Lymphoma (MCL) Page 1 of 9 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. PATHOLOGIC DIAGNOSIS INITIAL EVALUATION ESSENTIAL: ● Physical exam: attention to node-bearing areas, including Waldeyer's ring, ESSENTIAL: size of liver and spleen, and patient’s age ● Hematopathology review of all slides with at least one tumor paraffin block. ● Performance status (ECOG) Hematopathology confirmation of classic versus aggressive variant of MCL ● B symptoms (fever, drenching night sweats, unintentional weight loss) (blastoid/pleomorphic). Re-biopsy if consult material is non-diagnostic. ● CBC with differential, LDH, BUN, creatinine, albumin, AST, total bilirubin, 1 ● Adequate immunophenotype to confirm diagnosis alkaline phosphatase, serum calcium, uric acid ○ Paraffin panel: ● Screening for HIV 1 and 2, hepatitis B and C (HBcAb, HBaAg, HCVAb) - Pan B-cell marker (CD19, CD20, PAX5), CD3, CD5, CD10, and cyclin D1 ● Beta-2 microglobulin (B2M) - Ki-67 (proliferation rate) ● Chest x-ray, PA and lateral or ● Bone marrow bilateral biopsy with unilateral aspirate Induction ○ Flow cytometry immunophenotyping: -

CD20-Negative Diffuse Large B-Cell Lymphomas: Biology and Emerging Therapeutic Options
Expert Review of Hematology ISSN: 1747-4086 (Print) 1747-4094 (Online) Journal homepage: http://www.tandfonline.com/loi/ierr20 CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options Jorge J Castillo, Julio C Chavez, Francisco J Hernandez-Ilizaliturri & Santiago Montes-Moreno To cite this article: Jorge J Castillo, Julio C Chavez, Francisco J Hernandez-Ilizaliturri & Santiago Montes-Moreno (2015) CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options, Expert Review of Hematology, 8:3, 343-354, DOI: 10.1586/17474086.2015.1007862 To link to this article: http://dx.doi.org/10.1586/17474086.2015.1007862 Published online: 01 Feb 2015. Submit your article to this journal Article views: 165 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=ierr20 Download by: [North Shore Med Ctr], [Jorge Castillo] Date: 16 March 2016, At: 07:44 Review CD20-negative diffuse large B-cell lymphomas: biology and emerging therapeutic options Expert Rev. Hematol. 8(3), 343–354 (2015) Jorge J Castillo*1, CD20-negative diffuse large B-cell lymphoma (DLBCL) is a rare and heterogeneous group of Julio C Chavez2, lymphoproliferative disorders. Known variants of CD20-negative DLBCL include plasmablastic Francisco J lymphoma, primary effusion lymphoma, large B-cell lymphoma arising in human herpesvirus 8-associated multicentric Castleman disease and anaplastic lymphoma kinase-positive DLBCL. Hernandez-Ilizaliturri3 Given the lack of CD20 expression, atypical cellular morphology and aggressive clinical and Santiago 4 behavior characterized by chemotherapy resistance and inferior survival rates, CD20-negative Montes-Moreno DLBCL represents a challenge from the diagnostic and therapeutic perspectives. -

Divergent Clonal Evolution of a Common Precursor to Mantle Cell Lymphoma and Classic Hodgkin Lymphoma
Downloaded from molecularcasestudies.cshlp.org on September 23, 2021 - Published by Cold Spring Harbor Laboratory Press Divergent clonal evolution of a common precursor to mantle cell lymphoma and classic Hodgkin lymphoma Hammad Tashkandi1, Kseniya Petrova-Drus1, Connie Lee Batlevi2, Maria Arcila1, Mikhail Roshal1, Filiz Sen1, Jinjuan Yao1, Jeeyeon Baik1, Ashley Bilger2, Jessica Singh2, Stephanie de Frank2, Anita Kumar2, Ruth Aryeequaye1, Yanming Zhang1, Ahmet Dogan1, Wenbin Xiao1,* 1Department of Pathology, 2Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY *Correspondence: Wenbin Xiao, MD, PhD Department of Pathology Memorial Sloan Kettering Cancer Center 1275 York Avenue New York, NY 10065 [email protected] Running title: Clonally related mantle cell lymphoma and classic Hodgkin lymphoma Words: 1771 Figures: 2 Tables: 1 Reference: 14 Supplemental materials: Figure S1-S2, Table S1-S4 Downloaded from molecularcasestudies.cshlp.org on September 23, 2021 - Published by Cold Spring Harbor Laboratory Press Abstract: Clonal heterogeneity and evolution of mantle cell lymphoma (MCL) remain unclear despite the progress in our understanding of its biology. Here we report a 71 years old male patient with an aggressive MCL and depict the clonal evolution from initial diagnosis of typical MCL to relapsed blastoid MCL. During the course of disease, the patient was diagnosed with Classic Hodgkin lymphoma (CHL), and received CHL therapeutic regimen. Molecular analysis by next generation sequencing of both MCL and CHL demonstrated clonally related CHL with characteristic immunophenotype and PDL1/2 gains. Moreover, our data illustrate the clonal heterogeneity and acquisition of additional genetic aberrations including a rare fusion of SEC22B-NOTCH2 in the process of clonal evolution. -

Drug Resistance in Non-Hodgkin Lymphomas
International Journal of Molecular Sciences Review Drug Resistance in Non-Hodgkin Lymphomas Pavel Klener 1,2,* and Magdalena Klanova 1,2 1 First Department of Internale Medicine-Hematology, University General Hospital in Prague, 128 08 Prague, Czech Republic; [email protected] 2 Institute of Pathological Physiology, First Faculty of Medicine, Charles University, Prague, 128 53 Prague, Czech Republic * Correspondence: [email protected] or [email protected] Received: 3 February 2020; Accepted: 15 March 2020; Published: 18 March 2020 Abstract: Non-Hodgkin lymphomas (NHL) are lymphoid tumors that arise by a complex process of malignant transformation of mature lymphocytes during various stages of differentiation. The WHO classification of NHL recognizes more than 90 nosological units with peculiar pathophysiology and prognosis. Since the end of the 20th century, our increasing knowledge of the molecular biology of lymphoma subtypes led to the identification of novel druggable targets and subsequent testing and clinical approval of novel anti-lymphoma agents, which translated into significant improvement of patients’ outcome. Despite immense progress, our effort to control or even eradicate malignant lymphoma clones has been frequently hampered by the development of drug resistance with ensuing unmet medical need to cope with relapsed or treatment-refractory disease. A better understanding of the molecular mechanisms that underlie inherent or acquired drug resistance might lead to the design of more effective front-line treatment algorithms based on reliable predictive markers or personalized salvage therapy, tailored to overcome resistant clones, by targeting weak spots of lymphoma cells resistant to previous line(s) of therapy. This review focuses on the history and recent advances in our understanding of molecular mechanisms of resistance to genotoxic and targeted agents used in clinical practice for the therapy of NHL. -

Non-Hodgkin Lymphoma
Non-Hodgkin Lymphoma Rick, non-Hodgkin lymphoma survivor This publication was supported in part by grants from Revised 2013 A Message From John Walter President and CEO of The Leukemia & Lymphoma Society The Leukemia & Lymphoma Society (LLS) believes we are living at an extraordinary moment. LLS is committed to bringing you the most up-to-date blood cancer information. We know how important it is for you to have an accurate understanding of your diagnosis, treatment and support options. An important part of our mission is bringing you the latest information about advances in treatment for non-Hodgkin lymphoma, so you can work with your healthcare team to determine the best options for the best outcomes. Our vision is that one day the great majority of people who have been diagnosed with non-Hodgkin lymphoma will be cured or will be able to manage their disease with a good quality of life. We hope that the information in this publication will help you along your journey. LLS is the world’s largest voluntary health organization dedicated to funding blood cancer research, education and patient services. Since 1954, LLS has been a driving force behind almost every treatment breakthrough for patients with blood cancers, and we have awarded almost $1 billion to fund blood cancer research. Our commitment to pioneering science has contributed to an unprecedented rise in survival rates for people with many different blood cancers. Until there is a cure, LLS will continue to invest in research, patient support programs and services that improve the quality of life for patients and families. -

Relapsed Mantle Cell Lymphoma: Current Management, Recent Progress, and Future Directions
Journal of Clinical Medicine Review Relapsed Mantle Cell Lymphoma: Current Management, Recent Progress, and Future Directions David A Bond 1,*, Peter Martin 2 and Kami J Maddocks 1 1 Division of Hematology, The Ohio State University, Columbus, OH 43210, USA; [email protected] 2 Division of Hematology and Oncology, Weill Cornell Medical College, New York, NY 11021, USA; [email protected] * Correspondence: [email protected] Abstract: The increasing number of approved therapies for relapsed mantle cell lymphoma (MCL) provides patients effective treatment options, with increasing complexity in prioritization and se- quencing of these therapies. Chemo-immunotherapy remains widely used as frontline MCL treatment with multiple targeted therapies available for relapsed disease. The Bruton’s tyrosine kinase in- hibitors (BTKi) ibrutinib, acalabrutinib, and zanubrutinib achieve objective responses in the majority of patients as single agent therapy for relapsed MCL, but differ with regard to toxicity profile and dosing schedule. Lenalidomide and bortezomib are likewise approved for relapsed MCL and are active as monotherapy or in combination with other agents. Venetoclax has been used off-label for the treatment of relapsed and refractory MCL, however data are lacking regarding the efficacy of this approach particularly following BTKi treatment. Anti-CD19 chimeric antigen receptor T-cell (CAR-T) therapies have emerged as highly effective therapy for relapsed MCL, with the CAR-T treatment brexucabtagene autoleucel now approved for relapsed MCL. In this review the authors summarize evidence to date for currently approved MCL treatments for relapsed disease including Citation: Bond, D.A; Martin, P.; sequencing of therapies, and discuss future directions including combination treatment strategies Maddocks, K.J Relapsed Mantle Cell and new therapies under investigation. -

Mantle Cell Lymphoma Presenting As Acute Abdominal Syndrome: a Rare Case Report and Literature Review
healthcare Case Report Mantle Cell Lymphoma Presenting as Acute Abdominal Syndrome: A Rare Case Report and Literature Review Fu-Chou Lee 1, Junn-Liang Chang 2 , Hung-Ming Chen 3,4, Wan-Chen Tsai 5,6 and Po-Jen Hsiao 7,8,9,10,* 1 Department of Surgery, Taoyuan Armed Forces General Hospital, Taoyuan 325, Taiwan; [email protected] 2 Department of Pathology and Laboratory Medicine, Taoyuan Armed Forces General Hospital, Taoyuan 325, Taiwan; [email protected] 3 Division of Hematology and Oncology, Department of Internal Medicine, Taoyuan Armed Forces General Hospital, Taoyuan 325, Taiwan; [email protected] 4 Division of Hematology and Oncology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei 114, Taiwan 5 Division of General Surgery, Department of Surgery, Taoyuan Armed Forces General Hospital, Taoyuan 325, Taiwan; [email protected] 6 Division of General Surgery, Department of Surgery, Tri-Service General Hospital, National Defense Medical Center, Taipei 114, Taiwan 7 Division of Nephrology, Department of Internal Medicine, Tri-Service General Hospital, National Defense Medical Center, Taipei 114, Taiwan 8 Division of Nephrology, Department of Internal Medicine, Taoyuan Armed Forces General Hospital, Taoyuan 325, Taiwan 9 Department of Life Sciences, National Central University, Taoyuan 325, Taiwan 10 Big Data Research Center, Fu-Jen Catholic University, New Taipei City 242, Taiwan * Correspondence: [email protected] or [email protected]; Tel.: +886-3-479-9595 Abstract: Background: Acute abdominal syndrome can be caused by several possible reasons. The Citation: Lee, F.-C.; Chang, J.-L.; most common causes are perforation of a gastroduodenal ulcer, peritonitis, intestinal obstructions, Chen, H.-M.; Tsai, W.-C.; Hsiao, P.-J. -

The Cytogenetics of Hematologic Neoplasms 1 5
The Cytogenetics of Hematologic Neoplasms 1 5 Aurelia Meloni-Ehrig that errors during cell division were the basis for neoplastic Introduction growth was most likely the determining factor that inspired early researchers to take a better look at the genetics of the The knowledge that cancer is a malignant form of uncon- cell itself. Thus, the need to have cell preparations good trolled growth has existed for over a century. Several biologi- enough to be able to understand the mechanism of cell cal, chemical, and physical agents have been implicated in division became of critical importance. cancer causation. However, the mechanisms responsible for About 50 years after Boveri’s chromosome theory, the this uninhibited proliferation, following the initial insult(s), fi rst manuscripts on the chromosome makeup in normal are still object of intense investigation. human cells and in genetic disorders started to appear, fol- The fi rst documented studies of cancer were performed lowed by those describing chromosome changes in neoplas- over a century ago on domestic animals. At that time, the tic cells. A milestone of this investigation occurred in 1960 lack of both theoretical and technological knowledge with the publication of the fi rst article by Nowell and impaired the formulations of conclusions about cancer, other Hungerford on the association of chronic myelogenous leu- than the visible presence of new growth, thus the term neo- kemia with a small size chromosome, known today as the plasm (from the Greek neo = new and plasma = growth). In Philadelphia (Ph) chromosome, to honor the city where it the early 1900s, the fundamental role of chromosomes in was discovered (see also Chap.