Blood Flow Dynamics at the Pulmonary Artery Bifurcation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prep for Practical II
Images for Practical II BSC 2086L "Endocrine" A A B C A. Hypothalamus B. Pineal Gland (Body) C. Pituitary Gland "Endocrine" 1.Thyroid 2.Adrenal Gland 3.Pancreas "The Pancreas" "The Adrenal Glands" "The Ovary" "The Testes" Erythrocyte Neutrophil Eosinophil Basophil Lymphocyte Monocyte Platelet Figure 29-3 Photomicrograph of a human blood smear stained with Wright’s stain (765). Eosinophil Lymphocyte Monocyte Platelets Neutrophils Erythrocytes "Blood Typing" "Heart Coronal" 1.Right Atrium 3 4 2.Superior Vena Cava 5 2 3.Aortic Arch 6 4.Pulmonary Trunk 1 5.Left Atrium 12 9 6.Bicuspid Valve 10 7.Interventricular Septum 11 8.Apex of The Heart 9. Chordae tendineae 10.Papillary Muscle 7 11.Tricuspid Valve 12. Fossa Ovalis "Heart Coronal Section" Coronal Section of the Heart to show valves 1. Bicuspid 2. Pulmonary Semilunar 3. Tricuspid 4. Aortic Semilunar 5. Left Ventricle 6. Right Ventricle "Heart Coronal" 1.Pulmonary trunk 2.Right Atrium 3.Tricuspid Valve 4.Pulmonary Semilunar Valve 5.Myocardium 6.Interventricular Septum 7.Trabeculae Carneae 8.Papillary Muscle 9.Chordae Tendineae 10.Bicuspid Valve "Heart Anterior" 1. Brachiocephalic Artery 2. Left Common Carotid Artery 3. Ligamentum Arteriosum 4. Left Coronary Artery 5. Circumflex Artery 6. Great Cardiac Vein 7. Myocardium 8. Apex of The Heart 9. Pericardium (Visceral) 10. Right Coronary Artery 11. Auricle of Right Atrium 12. Pulmonary Trunk 13. Superior Vena Cava 14. Aortic Arch 15. Brachiocephalic vein "Heart Posterolateral" 1. Left Brachiocephalic vein 2. Right Brachiocephalic vein 3. Brachiocephalic Artery 4. Left Common Carotid Artery 5. Left Subclavian Artery 6. Aortic Arch 7. -

In the Pulmonary Arteries, Capillaries, and Veins
Longitudinal Distribution of Vascular Resistance in the Pulmonary Arteries, Capillaries, and Veins JEROME S. BRODY, EDWARD J. STEMMLER, and ARTHu B. DuBois From the Department of Physiology, Division of Graduate Medicine, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania 19104 A B S T R A C T A new method has been described monary artery pressure averaged 20.4 cm H2O, for measuring the pressure and resistance to blood and pulmonary vein pressure averaged 9.2 cm flow in the pulmonary arteries, capillaries, and H2O. These techniques also provide a way of ana- veins. Studies were performed in dog isolated lyzing arterial, capillary, and venous responses to lung lobes perfused at constant flow with blood various pharmacologic and physiologic stimuli. from a donor dog. Pulmonary artery and vein volume and total lobar blood volume were mea- INTRODUCTION sured by the ether plethysmograph and dye- dilution techniques. The longitudinal distribution The arterioles are the major resistance vessels in of vascular resistance was determined by analyzing the systemic vascular bed (1, 2), but it is uncer- the decrease in perfusion pressure caused by a tain whether the greatest resistance to blood flow bolus of low viscosity liquid introduced into the in the lungs is in the arteries, capillaries, or veins vascular inflow of the lobe. (1, 3, 4). The pulmonary arteries were responsible for Piiper (5), in 1958, reasoned from Poiseuille's 46% of total lobar vascular resistance, whereas law that, during constant perfusion, injection into the pulmonary capillaries and veins accounted for the bloodstream of a bolus of fluid with viscosity 34 and 20% of total lobar vascular resistance different from that of blood would cause a per- respectively. -

Surgical Techniques for Repair of Peripheral Pulmonary Artery Stenosis
STATE OF THE ART Surgical Techniques for Repair of Peripheral Pulmonary Artery Stenosis Richard D. Mainwaring, MD, and Frank L. Hanley, MD Peripheral pulmonary artery stenosis (PPAS) is a rare form of congenital heart disease that is most frequently associated with Williams and Alagille syndromes. These patients typically have systemic level right ventricular pressures secondary to obstruction at the lobar, segmental, and subseg- mental branches. The current management of patients with PPAS remains somewhat controversial. We have pioneered an entirely surgical approach for the reconstruction of PPAS. This approach initially entailed a surgical patch augmentation of all major lobar branches and effectively reduced the right ventricular pressures by more than half. This was the first report demonstrat- ing an effective approach to this disease. Over the past 5 years, we have An illustration demonstrating key steps in the surgical gradually evolved our technique of reconstruction to include segmental and technique for reconstruction of peripheral pulmonary artery stenosis. subsegmental branch stenoses. An important technical aspect of this approach entails the division of the main pulmonary and separation of the Central Message branch pulmonary arteries to access the lower lobe branches. Pulmonary artery homograft patches are used to augment hypoplastic pulmonary artery This article provides a detailed description of branches. In addition, we perform a Heinecke-Miculicz–type ostioplasty for the surgical techniques that have been devel- oped for the surgical reconstruction of periph- isolated ostial stenoses. The technical details of the surgical approach to eral pulmonary artery stenosis. PPAS are outlined in this article and can also be used for other complex peripheral pulmonary artery reconstructions. -

The Aorta, and Pulmonary Blood Flow
Br Heart J: first published as 10.1136/hrt.36.5.492 on 1 May 1974. Downloaded from British HeartJournal, I974, 36, 492-498. Relation between fetal flow patterns, coarctation of the aorta, and pulmonary blood flow Elliot A. Shinebourne and A. M. Elseed From the Department of Paediatrics, Brompton Hospital, National Heart and Chest Hospitals, London Intracardiac anomalies cause disturbances in fetal flow patterns which in turn influence dimensions of the great vessels. At birth the aortic isthmus, which receives 25 per cent of the combinedfetal ventricular output, is normally 25 to 30 per cent narrower than the descending aorta. A shelf-like indentation of the posterior aortic wall opposite the ductus characterizes thejunction of the isthmus with descending aorta. In tetralogy ofFallot, pulmonary atresia, and tricuspid atresia, when pulmonary blood flow is reduced from birth, the main pul- monary artery is decreased and ascending aorta increased in size. Conversely in intracardiac anomalies where blood is diverted away from the aorta to the pulmonary artery, isthmal narrowing or the posterior indentation may be exaggerated. Analysis of I62 patients with coarctation of the aorta showed 83 with an intracardiac anomaly resulting in increased pulmonary bloodflow and 21 with left-sided lesions present from birth. In contrast no patients with coarctation were found with diminished pulmonary flow or right-sided obstructive lesions. From this evidence the hypothesis is developed that coarctation is prevented whenflow in the main pulmonary artery is reduced in thefetus. http://heart.bmj.com/ The association of coarctation with left-sided establishing the complete intracardiac diagnosis in I62 obstructive lesions such as mitral and aortic stenosis patients with coarctation. -

Continuous Monitoring of Pulmonary Artery Pressure Via an Implanted
2016 Continuous monitoring of pulmonary artery pres- sure via an implanted leadless and battery less pres- sure sensor for the management of patients with moderate to severe heart failure (New York Heart As- sociation class III) A single technology assessment Title Continuous monitoring of pulmonary artery pressure via an implanted leadless and battery less pressure sensor for the management of patients with moderate to severe heart failure (New York Heart Association class III). A single technology assessment. Norwegian title Kontinuerlig monitorering av trykk i pulmonalarterien via en implantert trådløs sensor uten batteri for håndtering av pasienter med moderat til alvorlig hjertesvikt (New York Heart Association class III). Hurtigmetodevurdering. Institution Norwegian Institute of Public Health (Folkehelseinstitutttet) Camilla Stoltenberg, Director Authors Pike, Eva, (Project leader), senior researcher Bjerkan, Anne Mette, senior researcher Fagerlund, Beate Charlotte, health economist Hamidi, Vida, health economist Harboe, Ingrid, research librarian Klemp, Marianne, research director, Norwegian institute of public health ISBN 978-82-8082-771-5 Type of report A single technology assessment (Hurtigmetodevurdering) No. of pages 52, 72 including appendices) Client The Ordering Forum (Bestillerforum RHF) Subject heading Heart Failure; Blood Pressure Monitoring; Ambulatory; (MeSH) Wireless Technology Citation Pike E, Bjerkan AM, Fagerlund BC, Hamidi V, Harboe I, Klemp M. Continuous monitoring of pulmonary artery pressure via an implanted leadless and battery less pressure sensor for the management of patients with moderate to severe heart failure (New York Heart Association class III). A single technology assessment from Norwegian Institute of Public Health (Folkehelseinstitutttet). Oslo: Norwegian Institute of Public Health, 2016. Norwegian Institute of Public Health Oslo, October 2016 1 Executive summary Executive summary Background In Norway the prevalence of chronic heart failure has been estimated to be 2 per- cent, meaning 80 000 – 100 000 people. -

Circulatory System WARM-UP
_____ 1. Of the following, which is NOT involved in pulmonary circulation? a. Coronary Artery c. Right Ventricle b. Left Atrium d. Pulmonary Vein a. CORONARY ARTERY _____ 2. The heart of a human contains ______ chamber(s). a. One c. three b. Two d. four d. FOUR _____ 3. Blood is a tissue that consists of ____________. a. Cells c. liquid b. Cell fragments d. all of the above d. all of the above _____ 4. Of the following, which is NOT involved in systemic circulation? a. Aorta c. inferior vena cava b. Superior vena cava d. Pulmonary artery d. Pulmonary artery _____ 5. Of the following, which is NOT a function of blood? a. Digestion c. Carries oxygen b. Carries waste products d. Carries nutrients a. Digestion MATCH THE ANSWER WITH THE GIVEN QUESTION a. Capillaries f. Atria b. Pulmonary circulation g. Coronary circulation c. Arteries h. Ventricles d. Systemic Circulation i. Veins e. Blood Pressure _____ 6. Upper chambers of the heart f. Atria (plural form of Atrium) MATCH THE ANSWER WITH THE GIVEN QUESTION a. Capillaries f. Atria b. Pulmonary circulation g. Coronary circulation c. Arteries h. Ventricles d. Systemic Circulation i. Veins e. Blood Pressure _____ 7. Vessels that move blood toward the heart i. Veins MATCH THE ANSWER WITH THE GIVEN QUESTION a. Capillaries f. Atria b. Pulmonary circulation g. Coronary circulation c. Arteries h. Ventricles d. Systemic Circulation i. Veins e. Blood Pressure _____8. Vessels that move blood away from the heart c. arteries MATCH THE ANSWER WITH THE GIVEN QUESTION a. Capillaries f. -

Pulmonary Embolism
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES Pulmonary Embolism Part 1 Blood flows through the lungs from the right side of the heart to pick up oxygen and get rid of carbon dioxide (called Pulmonary Embolism gas exchange). The blood then flows from the lungs back to the left side of the heart to be pumped out to the rest of the body. A pulmonary embolism (PE) is a blood clot that gets Left into blood vessels in the lungs and prevents normal flow of Right atrium atrium blood in that area. This blockage causes problems with gas Right Left ventricle ventricle exchange. Depending on how big a clot and number of vessels involved, it can be a life-threatening event. Most blood clots that end up in the lungs first form in In addition, because of blockage, pressure increases the legs as deep vein thrombosis (DVT). This fact sheet back on the right side of the heart. The right heart can will discuss the diagnosis of pulmonary embolism. Part gets stretched and work harder. This can also affect the 2 will discuss treatment and prevention of pulmonary left side of the heart which get squeezed because of embolism. ballooned up (distended) right heart. If the left side of the heart is not able to pump enough blood, a person’s blood What is an acute pulmonary embolism? pressure also drops. Embolism (Em-bo-liz-m) refers to a blood clot (embolus) that has broken off and is floating freely All of these effects can lead to death, either suddenly, or if left untreated, in a short period after the pulmonary CLIP AND COPY AND CLIP in the blood vessel. -
Placement of Right Ventricle to Pulmonary Artery Conduit
Normal Heart © 2012 The Children’s Heart Clinic NOTES: Children’s Heart Clinic, P.A., 2530 Chicago Avenue S, Ste 500, Minneapolis, MN 55404 West Metro: 612-813-8800 * East Metro: 651-220-8800 * Toll Free: 1-800-938-0301 * Fax: 612-813-8825 Children’s Minnesota, 2525 Chicago Avenue S, Minneapolis, MN 55404 West Metro: 612-813-6000 * East Metro: 651-220-6000 © 2012 The Children’s Heart Clinic Reviewed March 2019 Right Ventricle to Pulmonary Artery (RV-PA) Conduit A right ventricle to pulmonary artery (RV-PA) conduit is a means to supply blood flow to the lungs. They can be placed for a variety of heart defects, including tetralogy of Fallot, pulmonary atre- sia, or pulmonary stenosis. RV-PA conduits are also part of a many complex surgeries for congen- ital heart disease, including the Ross procedure, Rastelli procedure, or in the Sano modification of the Norwood procedure. They can be placed to fix a regurgitant (leaky) or stenotic (narrowed) pulmonary valve. RV-PA conduits can also be used to replace an absent right ventricular outflow tract. There are many types of materials used for RV-PA conduits. Depending on the surgical plan and patient’s anatomy, conduits made of Gore-tex®(Gore), homograft (cadaver valved tissue), Contegra® conduits (Medtronic)(valved bovine (cow) jugular vein), or Hancock® conduits (Medtronic) (Dacron tube graft containing a porcine (pig) valve) can be used. A median sternotomy (incision through the middle of the chest) is done through the patient’s prior incision, if present. The patient is placed on cardiopulmonary bypass (heart–lung machine). -

Initial Isolated Takayasu's Arteritis of Bilateral Pulmonary Artery Branches
r e v b r a s r e u m a t o l . 2 0 1 7;5 7(6):626–629 REVISTA BRASILEIRA DE REUMATOLOGIA w ww.reumatologia.com.br Case report Initial isolated Takayasu’s arteritis of bilateral pulmonary artery branches Arterite de Takayasu com acometimento inicial isolado de ramos bilaterais da artéria pulmonar a a a b,∗ Yu-Hui Zhang , Wei-Min Song , Mei Wu , Jing Zhu a People’s Hospital of Bozhou, Department of Rheumatology, Bozhou, Anhui, China b Sichuan Provincial People’s Hospital, Department of Rheumatology, Chengdu, Sichuan, China a r t i c l e i n f o Article history: Received 3 April 2015 Accepted 13 October 2015 Available online 11 March 2016 dyspnea for 8 months. Tw o months ago, she was admitted to Introduction the department of cardiology in our hospital. Blood pressure was 126/83 mmHg without difference between bilateral arms. Takayasu’s arteritis chiefly affects the aorta and its major The echocardiography (ECHO) showed excessive stenosis of branches, including the pulmonary artery. Clinical presenta- both branches of pulmonary artery, the initial portion of the tions of TA are protean and not specific, the vast majority right branch with a lumen of 14 mm and the left 16 mm, and of patients presented vascular insufficiency such as stenosis, a significantly high pulmonary artery pressure of 118 mmHg occlusion, or aneurysm. Such features confuse TA with those (Fig. 1A–B). Dual source computed tomography (DSCT) verified of chronic thromboembolic diseases, fibrosing mediastinitis 1 a considerable partial stenosis of both branches of pulmonary or neoplasia, resulting in an erroneous initial diagnosis. -
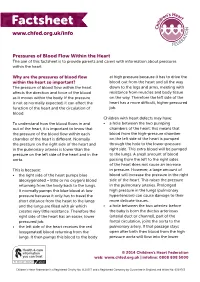
Why Are the Pressures of Blood Flow Within the Heart So Important?
Pressures of Blood Flow Within the Heart The aim of this factsheet is to provide parents and carers with information about pressures within the heart. Why are the pressures of blood flow at high pressure because it has to drive the within the heart so important? blood out from the heart and all the way The pressure of blood flow within the heart down to the legs and arms, meeting with affects the direction and force of the blood resistance from muscles and body tissue as it moves within the body. If the pressure on the way. Therefore the left side of the is not as normally expected, it can affect the heart has a more difficult, higher pressured function of the heart and the circulation of job. blood. Children with heart defects may have: To understand how the blood flows in and • a hole between the two pumping out of the heart, it is important to know that chambers of the heart: this means that the pressure of the blood flow within each blood from the high-pressure chamber chamber of the heart is different. Normally on the left side of the heart is pumped the pressure on the right side of the heart and through the hole to the lower-pressure in the pulmonary arteries is lower than the right side. This extra blood will be pumped pressure on the left side of the heart and in the to the lungs. A small amount of blood aorta. passing from the left to the right sides of the heart does not cause an increase This is because: in pressure. -

Pulsatile Flow in Pulmonary Artery, Capillary, and Vein in the Dog'
Cardiovascular Research, 1974, 8, 330-337. Pulsatile flow in pulmonary artery, capillary, and vein in the dog' Downloaded from https://academic.oup.com/cardiovascres/article/8/3/330/298317 by guest on 25 September 2021 WARREN G. GUNTHEROTH, RICHARD GOULD, JOHN BUTLER, and EDWIN KINNEN~ With the technical assistance of Donald Breazeale, George McGough, and John Mendenhall From the Departments of Pediatrics and Medicine, University of Washington School of Medicine, Seattle, Washington 98195, USA AUTHORS' SYNoPsis The temporal relationship of flow pulses in the pulmonary artery, capil- laries, and veins was investigated in 10 chronic dog preparations with pulsed ultrasonic flowmeters and a nitrous oxide-body plethysmograph for capillary flow. Implanted pressure transducers in the left atrium provided reference to the conventional atrial pulses: A, C, X-descent, V, and Y-descent. Left atrial contraction produced an A-wave pressure transient followed by retrograde flow up the veins. The C-pressure pulse occasionally produced a minimal trough in the venous flow pattern. Early in ventricular systole, X-descent in left atrial pressure preceded a venous flow pulse of modest amplitude, which began prior to the onset of the pulse of capillary flow. On average, right ventricular ejection was followed in 37 msec by the major flow pulse in the capillaries, which in turn was fol- lowed 68 msec later by the onset of venous flow. This venous flow pulse was simultaneous with a rise in left atrial pressure, the V-wave. With the onset of diastole, the Y-descent in atrial pressure pre- ceded a major venous flow pulse. With accelerated heart rate, separation of the V and Y venous flow pulses was lost, and a monophasic pulse was found. -

Left Common Carotid Artery Arising from the Pulmonary Artery in A
82 Heart 1996;76:82-83 CASE REPORT Left common carotid artery arising from the Heart: first published as 10.1136/hrt.76.1.82 on 1 July 1996. Downloaded from pulmonary artery in a patient with DiGeorge syndrome Shiu-Feng Huang, Mei-Hwan Wu Abstract Keywords: aortic arch anomaly; congenital vascular A female infant, born at 33 weeks' gesta- anomaly; DiGeorge syndrome; tetralogy of Fallot tion with tetralogy ofFallot, died ofsevere perinatal asphyxia 6 hours after birth. Patients with a right aortic arch can be classi- Necropsy disclosed two associated vascu- fied into several types according to the nature of lar anomalies: a right aortic arch with a the origin of the branches of the arch. The left common carotid artery arising from most common type is mirror image branches, the pulmonary artery (isolated left com- the second is aberrant left subclavian artery, Department of mon carotid artery) and an aberrant left and the third is isolation of the left subclavian Pathology, College of subclavian artery arising from the artery. Isolation of the left innominate artery is Medicine, National descending aorta. Agenesis of the thymus very rare, because its occurrence requires par- Taiwan University, and was also found, Taipei, Taiwan parathyroid gland tial regression of the aortic sac and the left S-F Huang suggesting that the child also had fourth aortic arch in early fetal life, which is Department of DiGeorge syndrome. Origin of the left very uncommon. Only six cases have been Pediatrics, College of common carotid artery from the pul- reported. 1-6 Isolation of the left common Medicine, National monary artery is exceedingly rare.