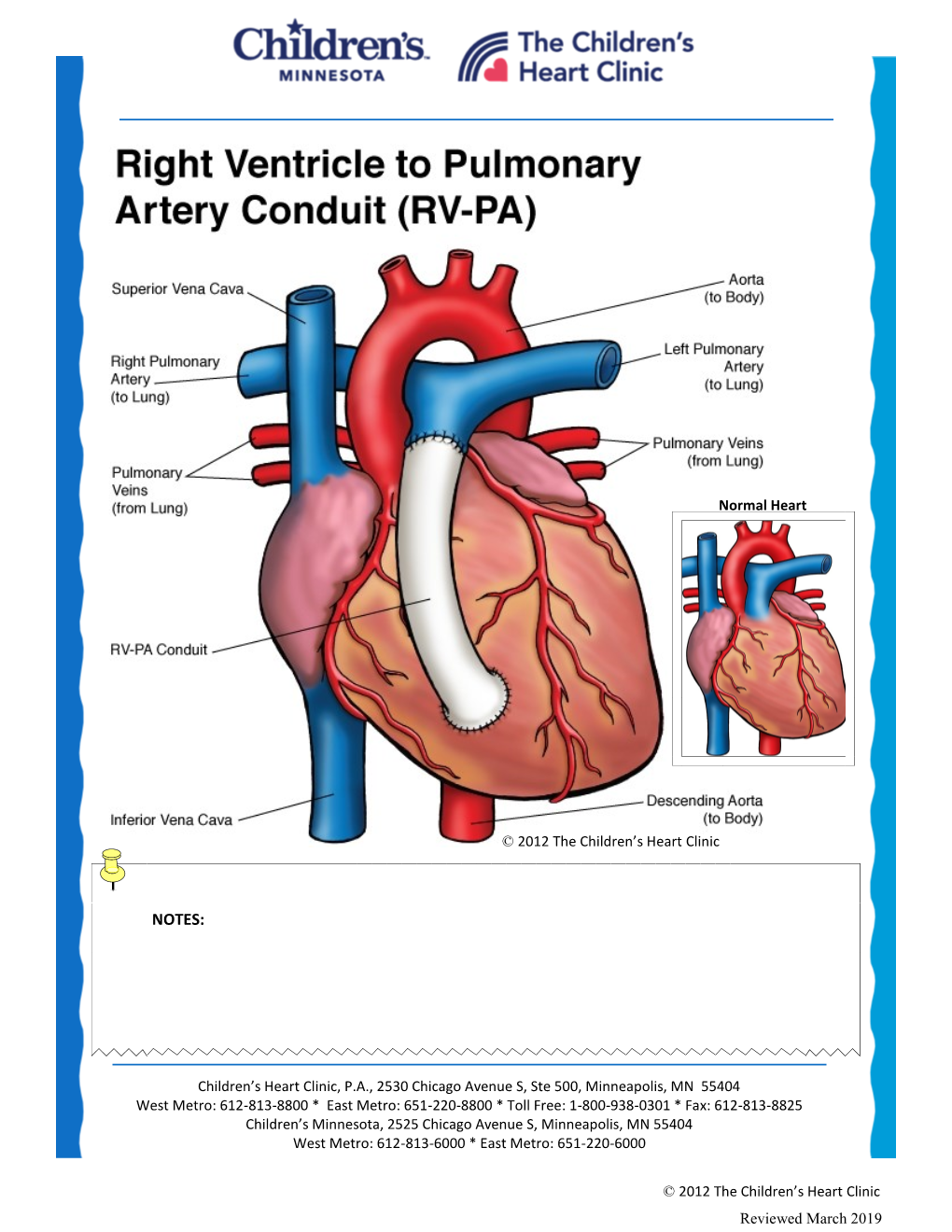
Placement of Right Ventricle to Pulmonary Artery Conduit
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Prep for Practical II
Images for Practical II BSC 2086L "Endocrine" A A B C A. Hypothalamus B. Pineal Gland (Body) C. Pituitary Gland "Endocrine" 1.Thyroid 2.Adrenal Gland 3.Pancreas "The Pancreas" "The Adrenal Glands" "The Ovary" "The Testes" Erythrocyte Neutrophil Eosinophil Basophil Lymphocyte Monocyte Platelet Figure 29-3 Photomicrograph of a human blood smear stained with Wright’s stain (765). Eosinophil Lymphocyte Monocyte Platelets Neutrophils Erythrocytes "Blood Typing" "Heart Coronal" 1.Right Atrium 3 4 2.Superior Vena Cava 5 2 3.Aortic Arch 6 4.Pulmonary Trunk 1 5.Left Atrium 12 9 6.Bicuspid Valve 10 7.Interventricular Septum 11 8.Apex of The Heart 9. Chordae tendineae 10.Papillary Muscle 7 11.Tricuspid Valve 12. Fossa Ovalis "Heart Coronal Section" Coronal Section of the Heart to show valves 1. Bicuspid 2. Pulmonary Semilunar 3. Tricuspid 4. Aortic Semilunar 5. Left Ventricle 6. Right Ventricle "Heart Coronal" 1.Pulmonary trunk 2.Right Atrium 3.Tricuspid Valve 4.Pulmonary Semilunar Valve 5.Myocardium 6.Interventricular Septum 7.Trabeculae Carneae 8.Papillary Muscle 9.Chordae Tendineae 10.Bicuspid Valve "Heart Anterior" 1. Brachiocephalic Artery 2. Left Common Carotid Artery 3. Ligamentum Arteriosum 4. Left Coronary Artery 5. Circumflex Artery 6. Great Cardiac Vein 7. Myocardium 8. Apex of The Heart 9. Pericardium (Visceral) 10. Right Coronary Artery 11. Auricle of Right Atrium 12. Pulmonary Trunk 13. Superior Vena Cava 14. Aortic Arch 15. Brachiocephalic vein "Heart Posterolateral" 1. Left Brachiocephalic vein 2. Right Brachiocephalic vein 3. Brachiocephalic Artery 4. Left Common Carotid Artery 5. Left Subclavian Artery 6. Aortic Arch 7. -

Pulmonary Valve Guideline
Pulmonary Valve What the Nurse Caring for a Patient with CHD Needs to Know Catherine Baxter, MSN, RN, CPNP-AC Nurse Practitioner, Pediatric Cardiac Surgery, Levine Children’s Hospital, Charlotte, NC Misty Ellis, MSN, CPNP-PC/AC Pediatric Cardiac Intensive Care Nurse Practitioner University of Louisville, Kosair Children’s Hospital Victoria Winter RN, MSN, CNS, CCRN Clinical Nurse IV, Adjunct Professor, Children’s Hospital Los Angeles and Azusa Pacific University School of Nursing Louise Callow, MSN, RN, CPNP Pediatric Cardiac Surgery Nurse Practitioner, University of Michigan, CS Mott Children’s Hospital Mary Rummell, MN, RN, CPNP, CNS, FAHA Clinical Nurse Specialist, Pediatric Cardiology/Cardiac Services, Oregon Health & Science University (Retired) Embryology Occurrence: o Defects of cardiac valves are the most common subtype of cardiac malformations o Account for 25% to 30% of all congenital heart defects o Most costly and relevant CHD o Wide spectrum of congenital defects in pulmonary valve Development of the heart valves occurs during the fourth to eighth weeks of gestation- after tubular heart looping o Walls of the tubular heart consist of an outer lining of myocardium and an inner lining of endocardial cells o Cardiac jelly, extensive extracellular matrix (ECM), separates the two layers o Cardiac jelly expands to form cardiac cushions at the sites of future valves . Outflow track (OT) valves = aortic and pulmonic valves Final valves derived from endothelial-mesenchymal cells with neural crest cells from the brachial arches Valves (Semilunar) have 3 equal cusp-shaped leaflets Aortic valve incorporates coronary arteries . Atrioventricular (AV) valves = mitral and tricuspid Final valves derived entirely from endocardial cushion tissue Leaflet formed without a cusp 1 Two leaflets associated with left ventricle (mitral) Three leaflets associated with right ventricle (tricuspid) Coordinated by complex interplay of: o Genetics o Signaling pathways that regulate cell apoptosis and proliferation o Environmental factors . -

In the Pulmonary Arteries, Capillaries, and Veins
Longitudinal Distribution of Vascular Resistance in the Pulmonary Arteries, Capillaries, and Veins JEROME S. BRODY, EDWARD J. STEMMLER, and ARTHu B. DuBois From the Department of Physiology, Division of Graduate Medicine, University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania 19104 A B S T R A C T A new method has been described monary artery pressure averaged 20.4 cm H2O, for measuring the pressure and resistance to blood and pulmonary vein pressure averaged 9.2 cm flow in the pulmonary arteries, capillaries, and H2O. These techniques also provide a way of ana- veins. Studies were performed in dog isolated lyzing arterial, capillary, and venous responses to lung lobes perfused at constant flow with blood various pharmacologic and physiologic stimuli. from a donor dog. Pulmonary artery and vein volume and total lobar blood volume were mea- INTRODUCTION sured by the ether plethysmograph and dye- dilution techniques. The longitudinal distribution The arterioles are the major resistance vessels in of vascular resistance was determined by analyzing the systemic vascular bed (1, 2), but it is uncer- the decrease in perfusion pressure caused by a tain whether the greatest resistance to blood flow bolus of low viscosity liquid introduced into the in the lungs is in the arteries, capillaries, or veins vascular inflow of the lobe. (1, 3, 4). The pulmonary arteries were responsible for Piiper (5), in 1958, reasoned from Poiseuille's 46% of total lobar vascular resistance, whereas law that, during constant perfusion, injection into the pulmonary capillaries and veins accounted for the bloodstream of a bolus of fluid with viscosity 34 and 20% of total lobar vascular resistance different from that of blood would cause a per- respectively. -

Chapter 12 the Cardiovascular System: the Heart Pages
CHAPTER 12 THE CARDIOVASCULAR SYSTEM: THE HEART PAGES 388 - 411 LOCATION & GENERAL FEATURES OF THE HEART TWO CIRCUIT CIRCULATORY SYSTEM DIVISIONS OF THE HEART FOUR CHAMBERS Right Atrium Left Atrium Receives blood from Receives blood from the systemic circuit the pulmonary circuit FOUR CHAMBERS Right Ventricle Left Ventricle Ejects blood into the Ejects blood into the pulmonary circuit systemic circuit FOUR VALVES –ATRIOVENTRICULAR VALVES Right Atrioventricular Left Atrioventricular Valve (AV) Valve (AV) Tricuspid Valve Bicuspid Valve and Mitral Valve FOUR VALVES –SEMILUNAR VALVES Pulmonary valve Aortic Valve Guards entrance to Guards entrance to the pulmonary trunk the aorta FLOW OF BLOOD MAJOR VEINS AND ARTERIES AROUND THE HEART • Arteries carry blood AWAY from the heart • Veins allow blood to VISIT the heart MAJOR VEINS AND ARTERIES ON THE HEART Coronary Circulation – Supplies blood to the muscle tissue of the heart ARTERIES Elastic artery: Large, resilient vessels. pulmonary trunk and aorta Muscular artery: Medium-sized arteries. They distribute blood to skeletal muscles and internal organs. external carotid artery of the neck Arteriole: Smallest of arteries. Lead into capillaries VEINS Large veins: Largest of the veins. Superior and Inferior Vena Cava Medium-sized veins: Medium sized veins. Pulmonary veins Venules: the smallest type of vein. Lead into capillaries CAPILLARIES Exchange of molecules between blood and interstitial fluid. FLOW OF BLOOD THROUGH HEART TISSUES OF THE HEART THE HEART WALL Pericardium Outermost layer Serous membrane Myocardium Middle layer Thick muscle layer Endocardium Inner lining of pumping chambers Continuous with endothelium CARDIAC MUSCLE Depend on oxygen to obtain energy Abundant in mitochondria In contact with several other cardiac muscles Intercalated disks – interlocking membranes of adjacent cells Desmosomes Gap junctions CONNECTIVE TISSUE Wrap around each cardiac muscle cell and tie together adjacent cells. -

Note: Before Reading the Specific Defect
Pulmonary Valve Stenosis and Regurgitation What is it? The pulmonary valve opens to let blood flow from the right ventricle to the lungs. Narrowing of the pulmonary valve, known as valvular pulmonary stenosis (PS) causes the right ventricle to pump harder to get blood past the blockage. Normally the pulmonary valve has three cusps. If these cusps are malformed, the valve may become narrowed (stenotic) or leaky (regurgitant or insufficiency). Pulmonary valve stenosis is much more common than regurgitation. The stenosis and regurgitation or both can be mild, moderate or severe. What causes it? In most cases, the cause isn’t known. It’s a common type of heart defect. Babies born to mothers who had rubella (German measles) during pregnancy were more likely to develop pulmonary stenosis along with deafness and patent ductus arteriosus. Some patients can have other heart defects along with PS. How does it affect the heart? Normally the right side of the heart pumps blood to the lungs. In a person with PS, the pressure in the right-heart pumping chamber (right ventricle) is much higher than normal and the heart must work harder to pump blood out into the lung arteries. Over time this can cause damage to the overworked heart muscle. When the valve is regurgitant it can cause the right ventricle to enlarge. How does the PS affect me? If the PS is severe, adults may complain of chest pain, exercise intolerance or have no symptoms. Cyanosis is rare and usually occurs only when there is an atrial or ventricular septal defect as well. -

Surgical Techniques for Repair of Peripheral Pulmonary Artery Stenosis
STATE OF THE ART Surgical Techniques for Repair of Peripheral Pulmonary Artery Stenosis Richard D. Mainwaring, MD, and Frank L. Hanley, MD Peripheral pulmonary artery stenosis (PPAS) is a rare form of congenital heart disease that is most frequently associated with Williams and Alagille syndromes. These patients typically have systemic level right ventricular pressures secondary to obstruction at the lobar, segmental, and subseg- mental branches. The current management of patients with PPAS remains somewhat controversial. We have pioneered an entirely surgical approach for the reconstruction of PPAS. This approach initially entailed a surgical patch augmentation of all major lobar branches and effectively reduced the right ventricular pressures by more than half. This was the first report demonstrat- ing an effective approach to this disease. Over the past 5 years, we have An illustration demonstrating key steps in the surgical gradually evolved our technique of reconstruction to include segmental and technique for reconstruction of peripheral pulmonary artery stenosis. subsegmental branch stenoses. An important technical aspect of this approach entails the division of the main pulmonary and separation of the Central Message branch pulmonary arteries to access the lower lobe branches. Pulmonary artery homograft patches are used to augment hypoplastic pulmonary artery This article provides a detailed description of branches. In addition, we perform a Heinecke-Miculicz–type ostioplasty for the surgical techniques that have been devel- oped for the surgical reconstruction of periph- isolated ostial stenoses. The technical details of the surgical approach to eral pulmonary artery stenosis. PPAS are outlined in this article and can also be used for other complex peripheral pulmonary artery reconstructions. -

Glossary of Commonly Used Heart and Vascular Terms
Glossary of Commonly Used Terms • Angina: Chest pain that occurs when an area of the heart muscle does not receive enough oxygen-rich blood. • Aorta: The largest artery in the body, it receives blood from the heart that has been oxygenated in the lungs, and delivers this blood to the body and brain. • Aortic Stenosis: A progressive disease that affects the aortic valve of the heart. • Aortic valve: The heart valve that regulates the one-way flow of blood from the left ventricle to the aorta. • Arteries: The blood vessels that carry oxygen-rich blood away from the heart and lungs. • Atria: The two upper chambers of the heart that receive blood returning from the body. • Balloon valvuloplasty: A procedure performed to open a narrowed heart valve using a thin tube called a catheter with a small balloon at its tip. The catheter is inserted through a small incision in the groin and then threaded up to the opening of the narrowed heart valve. The balloon is then inflated to stretch the valve open and relieve valve obstruction. • Bi-leaflet: A valve that has two leaflets that regulate the flow of blood. A normal aortic valve has three leaflets. • Calcification: A disease state in which calcium from the blood collects in the body tissues. When this occurs on the leaflets of the heart’s valves, it may cause them to harden and reduce their ability to open and close properly. • Cardiopulmonary bypass: Bypass of the heart and lungs. During this technique, which is often used during heart surgery, a heart-lung machine temporarily takes over the function of the heart and lungs. -

PHV Short.Indd
Anatomy & physiology: The heart Cardiac electrical conductance A Sinoatrial (SA) node D Right bundle branch B Atrioventricular (AV) node E Left bundle branch A C Atrioventricular bundle of His F Purkinje fibres The sinoatrial (SA) node is the heart's natural pacemaker, B containing cells that generate electrical impulses which spread F through the atria, triggering contraction of the atria, forcing blood into the ventricles, and stimulating the atrioventricular A (AV) node. E The AV node is linked with the atrioventricular bundle of His C which transmits impulses to the left and right bundle branches and then to the Purkinje fibres which surround the ventricles. The electrical impulses travel through the Purkinje fibres D causing the ventricles to contract and blood forced out of the heart. F Electrocardiogram (ECG) Heart construction The heart is a muscular, cone-shaped organ located behind The ECG traces the course of the cardiac impulse by the sternum and is approximately the same size as the recording the change in electrical potential on the surface of patient's closed fist. the body. Various parts of the ECG are associated with the travel of electrical impulses though the heart. The heart walls are made up the three structures: the pericardium, myocardium and endocardium. The P wave represents atrial depolarisation which causes the atria to contract. The pericardium is a thick fibrous membrane which surrounds the heart. Its function is to anchor the heart and Q is when the impulses arrive at the atrioventricular (AV) prevents over distension (expanding too much). node. The myocardium is the central layer of the heart and is The QRS complex represents ventricular depolarisation and formed from cardiac muscle tissue, it is this muscle which atrial repolarisation (ventricles contract and atria relax and provides the force which pumps the blood around the body. -

Pulmonary Valve Preservation Strategies for Tetralogy of Fallot Repair Constantine Mavroudis, MD
Pulmonary Valve Preservation Strategies for Tetralogy of Fallot Repair Constantine Mavroudis, MD he optimal repair for tetralogy of Fallot is challenged by techniques and acceptance of high intraoperative right ventri- Tthe management of the small right ventricular outflow cular to left ventricular pressure ratios of 0.7 or less.6-10 tract (RVOT), which was initially solved by John Kirklin who Transannular patches, when necessary, involved a strategy of determined that the absence of the pulmonary valve could transatrial RVOT resection, transatrial VSD closure, and be well tolerated owing to low pulmonary artery pressure limited ventriculotomy, oftentimes not extending the incision and preserved right ventricular function.1 This assumption more than 1-2 cm. Under these circumstances, transannular was affirmed in a significant number of patients who tolerated patches were intentionally downsized and reconstructed the persistent effects of right ventricular volume overload for to result in right ventricular gradients of approximately many years. In a significant number of postoperative patients, 20 mm Hg.11,12 however, long-term complications of pulmonary regurgitation, More comprehensive valve-sparing techniques that in- residual ventricular septal defects (VSD), distal pulmonary cluded a supravalvar pantaloon autologous pericardial patch artery stenosis, right ventricular dysfunction, atrial or ven- for supravalvar pulmonary stenosis were highlighted by – tricular arrhythmias, and exercise intolerance2-5 required several authors.8 10 These -
Incidental Cardiac and Pericardial Abnormalities on Chest CT
PICTORIAL ESSAY Incidental Cardiac and Pericardial Abnormalities on Chest CT Soo-Hyun Lee, MD,*w Joon Beom Seo, MD,* Joon-Won Kang, MD,* Eun Jin Chae, MD,* Seong Hoon Park, MD,* and Tae-Hwan Lim, MD* of an acute myocardial infarction results in a series of Objective: Although there has been an increasing interest in changes in the left ventricular (LV) myocardium, char- diagnosing cardiac and pericardial diseases using electrocardio- acterized by acute ischemia, myocardial death, and gram-gated cardiac computed tomography (CT), radiologists chronic remodeling.1 Although early studies performed tend to neglect or overlook many incidentally detected on conventional, single-slice, whole-body CT scanners, abnormalities on conventional, nongated chest CT. The demonstrated that acute myocardial infarction could be objective of this study is to describe the imaging appearance identified as a region of lower attenuation than normal and clinical significance of such cardiac or pericardial diseases. enhanced myocardium, diagnostic accuracy using the Conclusions: Recognition and detection of various cardiac and conventional CT is very low in diagnosing the acute pericardial abnormalities on chest CT as the evaluation of myocardial events as the cause of acute chest pain. noncardiac disease is important for its early diagnosis and However, incidental detection of coronary calcification 2,3 proper management. identifies individuals at risk for acute coronary events. Coronary artery calcification correlates highly with Key Words: CT, thoracic, heart, pericardium plaque burden but its relationship to plaque instability (J Thorac Imaging 2008;23:216–226) is low (Fig. 1). A mild degree of calcification characterizes patients with acute coronary events, whereas diffused high-attenuation calcific plaques are associated with chronic coronary events.4 dvances in computed tomography (CT) and magnetic LV myocardial aneurysms are relatively common resonance imaging have brought renewed interest to A sequelae of transmural myocardial infarction. -

1. Right Coronary 2. Left Anterior Descending 3. Left
1. RIGHT CORONARY 2. LEFT ANTERIOR DESCENDING 3. LEFT CIRCUMFLEX 4. SUPERIOR VENA CAVA 5. INFERIOR VENA CAVA 6. AORTA 7. PULMONARY ARTERY 8. PULMONARY VEIN 9. RIGHT ATRIUM 10. RIGHT VENTRICLE 11. LEFT ATRIUM 12. LEFT VENTRICLE 13. PAPILLARY MUSCLES 14. CHORDAE TENDINEAE 15. TRICUSPID VALVE 16. MITRAL VALVE 17. PULMONARY VALVE Coronary Arteries Because the heart is composed primarily of cardiac muscle tissue that continuously contracts and relaxes, it must have a constant supply of oxygen and nutrients. The coronary arteries are the network of blood vessels that carry oxygen- and nutrient-rich blood to the cardiac muscle tissue. The blood leaving the left ventricle exits through the aorta, the body’s main artery. Two coronary arteries, referred to as the "left" and "right" coronary arteries, emerge from the beginning of the aorta, near the top of the heart. The initial segment of the left coronary artery is called the left main coronary. This blood vessel is approximately the width of a soda straw and is less than an inch long. It branches into two slightly smaller arteries: the left anterior descending coronary artery and the left circumflex coronary artery. The left anterior descending coronary artery is embedded in the surface of the front side of the heart. The left circumflex coronary artery circles around the left side of the heart and is embedded in the surface of the back of the heart. Just like branches on a tree, the coronary arteries branch into progressively smaller vessels. The larger vessels travel along the surface of the heart; however, the smaller branches penetrate the heart muscle. -

The Aorta, and Pulmonary Blood Flow
Br Heart J: first published as 10.1136/hrt.36.5.492 on 1 May 1974. Downloaded from British HeartJournal, I974, 36, 492-498. Relation between fetal flow patterns, coarctation of the aorta, and pulmonary blood flow Elliot A. Shinebourne and A. M. Elseed From the Department of Paediatrics, Brompton Hospital, National Heart and Chest Hospitals, London Intracardiac anomalies cause disturbances in fetal flow patterns which in turn influence dimensions of the great vessels. At birth the aortic isthmus, which receives 25 per cent of the combinedfetal ventricular output, is normally 25 to 30 per cent narrower than the descending aorta. A shelf-like indentation of the posterior aortic wall opposite the ductus characterizes thejunction of the isthmus with descending aorta. In tetralogy ofFallot, pulmonary atresia, and tricuspid atresia, when pulmonary blood flow is reduced from birth, the main pul- monary artery is decreased and ascending aorta increased in size. Conversely in intracardiac anomalies where blood is diverted away from the aorta to the pulmonary artery, isthmal narrowing or the posterior indentation may be exaggerated. Analysis of I62 patients with coarctation of the aorta showed 83 with an intracardiac anomaly resulting in increased pulmonary bloodflow and 21 with left-sided lesions present from birth. In contrast no patients with coarctation were found with diminished pulmonary flow or right-sided obstructive lesions. From this evidence the hypothesis is developed that coarctation is prevented whenflow in the main pulmonary artery is reduced in thefetus. http://heart.bmj.com/ The association of coarctation with left-sided establishing the complete intracardiac diagnosis in I62 obstructive lesions such as mitral and aortic stenosis patients with coarctation.