A-Guide-To-Y90-Radioembolization-And-Its-Dosimetry.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Investigation Study Radiation Profile on a 20 Gbq Therasphere Dose Vial
Attachment 14 NUCLEAR MEDICINE M Nordion KANATA OPERATIONS INVESTIGATION STUDY PD99099003.08 Page No: I of 4 Investigation Study Radiation Profile on a 20 GBq TheraSphere Dose Vial I Signatures Prepared by: Date: ý - Al -; Approved by:. Date: 2•-O--c "Y (Richard Decaire CAHT) Document History Date Version''• •Comments Prepared by . Reviewed by Approved by PD99099003.08 Page Investigation No: 2 of 4 Study Radiation Profile on a 20 GBq TheraSphere Dose Vial 1. INTRODUCTION The United States Nuclear Regulatory Commission had requested information to support MDS Nordion application for the registration of TheraSphere. This request is contained in a letter dated November 23, 1999 from a Dr John P. Jankovich. This report contains data collected to address question 7 parts a, b, and c. The question poised is as follows: "Regarding external radiation levels, NRC needs information on the device itself, not on the radiation levels around the patient as addressed in the application. Therefore, please specify: a. External radiation levels around the lucite vial containing the maximum dose of 20 GBq (540 mCi). Provide the data, preferably, at the surface, and at 5, 30, and 100 cm. If there are no meaningful readings at these locations, please state so. b. Provide similar external radiation levels, if any, outside the lead pot with the lucite vial inside containing a maximum dose of microspheres. c. Please specify the instrument which you used to perform the radiation profile measurements by listing the instrument manufacturers, model numbers, calibration dates, sensitivity, etc." To address these questions, information was provided from previous development work. -

3Rd Quarter 2001 Bulletin
In This Issue... Promoting Colorectal Cancer Screening Important Information and Documentaion on Promoting the Prevention of Colorectal Cancer ....................................................................................................... 9 Intestinal and Multi-Visceral Transplantation Coverage Guidelines and Requirements for Approval of Transplantation Facilities12 Expanded Coverage of Positron Emission Tomography Scans New HCPCS Codes and Coverage Guidelines Effective July 1, 2001 ..................... 14 Skilled Nursing Facility Consolidated Billing Clarification on HCPCS Coding Update and Part B Fee Schedule Services .......... 22 Final Medical Review Policies 29540, 33282, 67221, 70450, 76090, 76092, 82947, 86353, 93922, C1300, C1305, J0207, and J9293 ......................................................................................... 31 Outpatient Prospective Payment System Bulletin Devices Eligible for Transitional Pass-Through Payments, New Categories and Crosswalk C-codes to Be Used in Coding Devices Eligible for Transitional Pass-Through Payments ............................................................................................ 68 Features From the Medical Director 3 he Medicare A Bulletin Administrative 4 Tshould be shared with all General Information 5 health care practitioners and managerial members of the General Coverage 12 provider/supplier staff. Hospital Services 17 Publications issued after End Stage Renal Disease 19 October 1, 1997, are available at no-cost from our provider Skilled Nursing Facility -

Review of Intra-Arterial Therapies for Colorectal Cancer Liver Metastasis
cancers Review Review of Intra-Arterial Therapies for Colorectal Cancer Liver Metastasis Justin Kwan * and Uei Pua Department of Vascular and Interventional Radiology, Tan Tock Seng Hospital, Singapore 388403, Singapore; [email protected] * Correspondence: [email protected] Simple Summary: Colorectal cancer liver metastasis occurs in more than 50% of patients with colorectal cancer and is thought to be the most common cause of death from this cancer. The mainstay of treatment for inoperable liver metastasis has been combination systemic chemotherapy with or without the addition of biological targeted therapy with a goal for disease downstaging, for potential curative resection, or more frequently, for disease control. For patients with dominant liver metastatic disease or limited extrahepatic disease, liver-directed intra-arterial therapies including hepatic arterial chemotherapy infusion, chemoembolization and radioembolization are alternative treatment strategies that have shown promising results, most commonly in the salvage setting in patients with chemo-refractory disease. In recent years, their role in the first-line setting in conjunction with concurrent systemic chemotherapy has also been explored. This review aims to provide an update on the current evidence regarding liver-directed intra-arterial treatment strategies and to discuss potential trends for the future. Abstract: The liver is frequently the most common site of metastasis in patients with colorectal cancer, occurring in more than 50% of patients. While surgical resection remains the only potential Citation: Kwan, J.; Pua, U. Review of curative option, it is only eligible in 15–20% of patients at presentation. In the past two decades, Intra-Arterial Therapies for Colorectal major advances in modern chemotherapy and personalized biological agents have improved overall Cancer Liver Metastasis. -
Variations in the Practice of Molecular Radiotherapy and Implementation Of
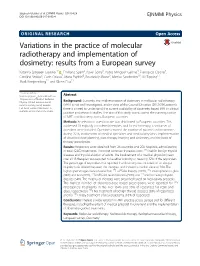
Sjögreen Gleisner et al. EJNMMI Physics (2017) 4:28 EJNMMI Physics DOI 10.1186/s40658-017-0193-4 ORIGINAL RESEARCH Open Access Variations in the practice of molecular radiotherapy and implementation of dosimetry: results from a European survey Katarina Sjögreen Gleisner1* , Emiliano Spezi2, Pavel Solny3, Pablo Minguez Gabina4, Francesco Cicone5, Caroline Stokke6, Carlo Chiesa7, Maria Paphiti8, Boudewijn Brans9, Mattias Sandström10, Jill Tipping11, Mark Konijnenberg12 and Glenn Flux13 * Correspondence: [email protected] Abstract 1Department of Medical Radiation Physics, Clinical Sciences Lund, Background: Currently, the implementation of dosimetry in molecular radiotherapy Lund University, Lund, Sweden (MRT) is not well investigated, and in view of the Council Directive (2013/59/Euratom), Full list of author information is there is a need to understand the current availability of dosimetry-based MRT in clinical available at the end of the article practice and research studies. The aim of this study was to assess the current practice of MRT and dosimetry across European countries. Methods: An electronic questionnaire was distributed to European countries. This addressed 18 explicitly considered therapies, and for each therapy, a similar set of questions were included. Questions covered the number of patients and treatments during 2015, involvement of medical specialties and medical physicists, implementation of absorbed dose planning, post-therapy imaging and dosimetry, and the basis of therapy prescription. Results: Responses were obtained from 26 countries and 208 hospitals, administering in total 42,853 treatments. The most common therapies were 131I-NaI for benign thyroid diseases and thyroid ablation of adults. The involvement of a medical physicist (mean over all 18 therapies) was reported to be either minority or never by 32% of the responders. -

Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors
UnitedHealthcare® Commercial Medical Policy Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors Policy Number: 2021T0445S Effective Date: August 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policy Coverage Rationale ........................................................................... 1 • Abnormal Uterine Bleeding and Uterine Fibroids Documentation Requirements......................................................... 1 Definitions ........................................................................................... 2 Community Plan Policy Applicable Codes .............................................................................. 2 • Implantable Beta-Emitting Microspheres for Treatment of Malignant Tumors Description of Services ..................................................................... 3 Clinical Evidence ............................................................................... 3 Medicare Advantage Coverage Summary U.S. Food and Drug Administration ..............................................15 • Brachytherapy Procedures References .......................................................................................15 Policy History/Revision Information..............................................18 Instructions for Use .........................................................................19 Coverage Rationale Transarterial radioembolization (TARE) using yttrium-90 (90Y) microspheres is proven and medically necessary for the following: • When used -

The International Commission on Radiological Protection: Historical Overview
Topical report The International Commission on Radiological Protection: Historical overview The ICRP is revising its basic recommendations by Dr H. Smith Within a few weeks of Roentgen's discovery of gamma rays; 1.5 roentgen per working week for radia- X-rays, the potential of the technique for diagnosing tion, affecting only superficial tissues; and 0.03 roentgen fractures became apparent, but acute adverse effects per working week for neutrons. (such as hair loss, erythema, and dermatitis) made hospital personnel aware of the need to avoid over- Recommendations in the 1950s exposure. Similar undesirable acute effects were By then, it was accepted that the roentgen was reported shortly after the discovery of radium and its inappropriate as a measure of exposure. In 1953, the medical applications. Notwithstanding these observa- ICRU recommended that limits of exposure should be tions, protection of staff exposed to X-rays and gamma based on consideration of the energy absorbed in tissues rays from radium was poorly co-ordinated. and introduced the rad (radiation absorbed dose) as a The British X-ray and Radium Protection Committee unit of absorbed dose (that is, energy imparted by radia- and the American Roentgen Ray Society proposed tion to a unit mass of tissue). In 1954, the ICRP general radiation protection recommendations in the introduced the rem (roentgen equivalent man) as a unit early 1920s. In 1925, at the First International Congress of absorbed dose weighted for the way different types of of Radiology, the need for quantifying exposure was radiation distribute energy in tissue (called the dose recognized. As a result, in 1928 the roentgen was equivalent in 1966). -

MIRD Pamphlet No. 22 - Radiobiology and Dosimetry of Alpha- Particle Emitters for Targeted Radionuclide Therapy
Alpha-Particle Emitter Dosimetry MIRD Pamphlet No. 22 - Radiobiology and Dosimetry of Alpha- Particle Emitters for Targeted Radionuclide Therapy George Sgouros1, John C. Roeske2, Michael R. McDevitt3, Stig Palm4, Barry J. Allen5, Darrell R. Fisher6, A. Bertrand Brill7, Hong Song1, Roger W. Howell8, Gamal Akabani9 1Radiology and Radiological Science, Johns Hopkins University, Baltimore MD 2Radiation Oncology, Loyola University Medical Center, Maywood IL 3Medicine and Radiology, Memorial Sloan-Kettering Cancer Center, New York NY 4International Atomic Energy Agency, Vienna, Austria 5Centre for Experimental Radiation Oncology, St. George Cancer Centre, Kagarah, Australia 6Radioisotopes Program, Pacific Northwest National Laboratory, Richland WA 7Department of Radiology, Vanderbilt University, Nashville TN 8Division of Radiation Research, Department of Radiology, New Jersey Medical School, University of Medicine and Dentistry of New Jersey, Newark NJ 9Food and Drug Administration, Rockville MD In collaboration with the SNM MIRD Committee: Wesley E. Bolch, A Bertrand Brill, Darrell R. Fisher, Roger W. Howell, Ruby F. Meredith, George Sgouros (Chairman), Barry W. Wessels, Pat B. Zanzonico Correspondence and reprint requests to: George Sgouros, Ph.D. Department of Radiology and Radiological Science CRB II 4M61 / 1550 Orleans St Johns Hopkins University, School of Medicine Baltimore MD 21231 410 614 0116 (voice); 413 487-3753 (FAX) [email protected] (e-mail) - 1 - Alpha-Particle Emitter Dosimetry INDEX A B S T R A C T......................................................................................................................... -

Of Richard Martin on Yttrium-90 Microsphere Brachytherapy
Page 1 of 1 As of: 2/8/18 2:05 PM Received: February 08, 2018 Status: Pending~Post PUBLIC SUBMISSION Tracking No. lk2-91du-ys8n Comments Due: February 08, 2018 Submission Type: Web Docket: NRC-2017-0215 Yttrium-90 Microsphere Brachytherapy Sources and Devices Therasphere and SIR-Spheres Comment On: NRC-2017-0215-0024 Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres; Draft Guidance; Extension of Comment Period Document: NRC-2017-0215-DRAFT-0132 Comment on FR Doc# 2017-28271 Submitter Information Name: Richard Martin Organization: American Association of Physicists in Medicine General Comment See attached file(s) Attachments AAPM Comment NRC Y-90 Guidance Final RM SUNSI Review Complete Template= ADM - 013 E-RIDS= ADM-03 · Add= l.1 SCA.\), m )11 1lJ:. C) lch) K~~-t.ri11"1 MP.P ( Kris!) https://www.fdms.gov/fdms/getcontent?objectld=0900006482f01e40&format=xml&showorig=false 02/08/2018 ''l, :~:~~.::. ' ••• ·: ·.~ ••~ ~ •'<",• ··:. : •• · 1 • ~ • • • • • ' • • • j db AMERICAN ASSOCIATION ~l7ef PHYSICISTS IN MEDICINE February 8, 2018 May Ma Office of Administration Mail Stop: OWFN-2-A13 U.S. Nuclear Regulatory Commission Washington, DC 20555-0001 RE: Request for Comment: Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres Draft Guidance (NRC-2017-0215) Dear Ms. Ma: The American Association of Physicists in Medicine (AAPM)1 is pleased to submit comments to the U.S. Nuclear Regulatory Commission (NRC) regarding Yttrium-90 Microsphere Brachytherapy Sources and Devices TheraSphere and SIR-Spheres Draft Licensing Guidance (Revision 10). The AAPM commends the NRC on its work in providing the NRC with a set of standard criteria for evaluating a medical use license application for the use of TheraSpheres and SIR-Spheres. -
Residency Essentials Full Curriculum Syllabus
RESIDENCY ESSENTIALS FULL CURRICULUM SYLLABUS Please review your topic area to ensure all required sections are included in your module. You can also use this document to review the surrounding topics/sections to ensure fluidity. Click on the topic below to jump to that page. Clinical Topics • Gastrointestinal • Genitourinary • Men’s Health • Neurological • Oncology • Pain Management • Pediatrics • Vascular Arterial • Vascular Venous • Women’s Health Requisite Knowledge • Systems • Business and Law • Physician Wellness and Development • Research and Statistics Fundamental • Clinical Medicine • Intensive Care Medicine • Image-guided Interventions • Imaging and Anatomy Last revised: November 4, 2019 Gastrointestinal 1. Portal hypertension a) Pathophysiology (1) definition and normal pressures and gradients, MELD score (2) Prehepatic (a) Portal, SMV or Splenic (i) thrombosis (ii) stenosis (b) Isolated mesenteric venous hypertension (c) Arterioportal fistula (3) Sinusoidal (intrahepatic) (a) Cirrhosis (i) ETOH (ii) Non-alcoholic fatty liver disease (iii) Autoimmune (iv) Viral Hepatitis (v) Hemochromatosis (vi) Wilson's disease (b) Primary sclerosing cholangitis (c) Primary biliary cirrhosis (d) Schistosomiasis (e) Infiltrative liver disease (f) Drug/Toxin/Chemotherapy induced chronic liver disease (4) Post hepatic (a) Budd Chiari (Primary secondary) (b) IVC or cardiac etiology (5) Ectopic perianastomotic and stomal varices (6) Splenorenal shunt (7) Congenital portosystemic shunt (Abernethy malformation) b) Measuring portal pressure (1) Direct -

Radiation Glossary
Radiation Glossary Activity The rate of disintegration (transformation) or decay of radioactive material. The units of activity are Curie (Ci) and the Becquerel (Bq). Agreement State Any state with which the U.S. Nuclear Regulatory Commission has entered into an effective agreement under subsection 274b. of the Atomic Energy Act of 1954, as amended. Under the agreement, the state regulates the use of by-product, source, and small quantities of special nuclear material within said state. Airborne Radioactive Material Radioactive material dispersed in the air in the form of dusts, fumes, particulates, mists, vapors, or gases. ALARA Acronym for "As Low As Reasonably Achievable". Making every reasonable effort to maintain exposures to ionizing radiation as far below the dose limits as practical, consistent with the purpose for which the licensed activity is undertaken. It takes into account the state of technology, the economics of improvements in relation to state of technology, the economics of improvements in relation to benefits to the public health and safety, societal and socioeconomic considerations, and in relation to utilization of radioactive materials and licensed materials in the public interest. Alpha Particle A positively charged particle ejected spontaneously from the nuclei of some radioactive elements. It is identical to a helium nucleus, with a mass number of 4 and a charge of +2. Annual Limit on Intake (ALI) Annual intake of a given radionuclide by "Reference Man" which would result in either a committed effective dose equivalent of 5 rems or a committed dose equivalent of 50 rems to an organ or tissue. Attenuation The process by which radiation is reduced in intensity when passing through some material. -
External and Internal Dosimetry
Chapter 7 External and Internal Dosimetry H-117 – Introductory Health Physics Slide 1 Objectives ¾ Discuss factors influencing external and internal doses ¾ Define terms used in external dosimetry ¾ Discuss external dosimeters such as TLDs, film badges, OSL dosimeters, pocket chambers, and electronic dosimetry H-117 – Introductory Health Physics Slide 2 Objectives ¾ Define terms used in internal dosimetry ¾ Discuss dose units and limits ¾ Define the ALI, DAC and DAC-hr ¾ Discuss radiation signs and postings H-117 – Introductory Health Physics Slide 3 Objectives ¾ Discuss types of bioassays ¾ Describe internal dose measuring equipment and facilities ¾ Discuss principles of internal dose calculation and work sample problems H-117 – Introductory Health Physics Slide 4 External Dosimetry H-117 – Introductory Health Physics Slide 5 External Dosimetry Gamma, beta or neutron radiation emitted by radioactive material outside the body irradiates the skin, lens of the eye, extremities & the whole body (i.e. internal organs) H-117 – Introductory Health Physics Slide 6 External Dosimetry (cont.) ¾ Alpha particles cannot penetrate the dead layer of skin (0.007 cm) ¾ Beta particles are primarily a skin hazard. However, energetic betas can penetrate the lens of an eye (0.3 cm) and deeper tissue (1 cm) ¾ Beta sources can produce more penetrating radiation through bremsstrahlung ¾ Primary sources of external exposure are photons and neutrons ¾ External dose must be measured by means of appropriate dosimeters H-117 – Introductory Health Physics Slide 7 -

MG Selective Internal Radiation Therapy
Selective Internal Radiation Therapy Last Review Date: May 7, 2021 Number: MG.MM.RA.12d Medical Guideline Disclaimer Property of EmblemHealth. All rights reserved. The treating physician or primary care provider must submit to EmblemHealth the clinical evidence that the patient meets the criteria for the treatment or surgical procedure. Without this documentation and information, EmblemHealth will not be able to properly review the request for prior authorization. The clinical review criteria expressed below reflects how EmblemHealth determines whether certain services or supplies are medically necessary. EmblemHealth established the clinical review criteria based upon a review of currently available clinical information (including clinical outcome studies in the peer reviewed published medical literature, regulatory status of the technology, evidence-based guidelines of public health and health research agencies, evidence-based guidelines and positions of leading national health professional organizations, views of physicians practicing in relevant clinical areas, and other relevant factors). EmblemHealth expressly reserves the right to revise these conclusions as clinical information changes and welcomes further relevant information. Each benefit program defines which services are covered. The conclusion that a particular service or supply is medically necessary does not constitute a representation or warranty that this service or supply is covered and/or paid for by EmblemHealth, as some programs exclude coverage for services or supplies that EmblemHealth considers medically necessary. If there is a discrepancy between this guideline and a member's benefits program, the benefits program will govern. In addition, coverage may be mandated by applicable legal requirements of a state, the Federal Government or the Centers for Medicare & Medicaid Services (CMS) for Medicare and Medicaid members.