Dr. Barton Schmitt's Toilet Training Guidelines for Parents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
1-Intro Pages 3
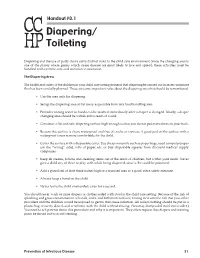
Handout #8.1 Diapering/ Toileting Diapering and the use of potty chairs carry distinct risks to the child care environment. Since the changing area is one of the places where germs which cause disease are most likely to live and spread, these activities must be handled with extreme care and attention to sanitation. The Diapering Area The health and safety of the children in your child care setting demand that diapering be carried out in an environment that has been carefully planned. These are some important rules about the diapering area that should be remembered: • Use the area only for diapering. • Set up the diapering area as far away as possible from any food handling area. • Provide running water so hands can be washed immediately after a diaper is changed. Ideally, a diaper changing area should be within arm’s reach of a sink. • Construct a flat and safe diapering surface high enough so that you do not put extra stress on your back. • Be sure this surface is clean, waterproof and free of cracks or crevices. A good pad on the surface with a waterproof cover is more comfortable for the child. • Cover the surface with a disposable cover. Use cheap materials such as paper bags, used computer paper (on the “wrong” side), rolls of paper, etc. or buy disposable squares from discount medical supply companies. • Keep all creams, lotions and cleaning items out of the reach of children, but within your reach. Never give a child any of these to play with while being diapered, since s/he could be poisoned. -

Is There an Association Between Urinary Tract Infection and Toilet Type?
Original Research / Özgün Araştırma Is There an Association Between Urinary Tract Infection and Toilet Type? İdrar Yolu Enfeksiyonu ile Tuvalet Tipi Arasında İlişki Var mı? Basri Furkan Dağcıoğlu*1, Erhan Şimşek1, Ramazan İlbey Tepeli1 ABSTRACT Aim: Many metabolic, physiological, and social factors play a role in the formation of infections. The results of the studies investigating the association between toilet type and urinary tract infection (UTI) are contradictory. This study aims to investigate the relationship between UTI and toilet habits and toilet type used. Methods: A cross-sectional study, including 344 participants between the ages of 18-60, was conducted. Sociodemographic information, toilet preferences, toilet habits, diagnosed chronic diseases, and histories of UTI were questioned with a structured questionnaire. Results: Front-to-back wiping, use of urinals in public places, and use of toilet paper were associated with a history of UTI in some genders. No significant relationship was observed between the parameters of general toilet preference, type of toilet preferred at home, and the frequency of water closet use, and UTI history in both genders. Conclusion: The toilet preference and some toileting habits may play a role in UTI. Further studies are required to reveal the real significance of this association. Keywords: Urinary tract infection, toilet type, water closet, squatting toilet, toileting behaviors. ÖZET Giriş: Enfeksiyonların oluşumunda birçok metabolik, fizyolojik ve sosyal faktör rol oynar. Tuvalet tipi ile idrar yolu enfeksiyonu (İYE) arasındaki ilişkiyi araştıran çalışmaların sonuçları çelişkilidir. Bu çalışmanın amacı, İYE ile tuvalet alışkanlıkları ve kullanılan tuvalet türü arasındaki ilişkiyi incelemektir. Yöntem: 18-60 yaş arası 344 katılımcının yer aldığı kesitsel bir çalışma gerçekleştirildi. -

Redalyc.Toilet Training
Jornal de Pediatria ISSN: 0021-7557 [email protected] Sociedade Brasileira de Pediatria Brasil Mota, Denise M.; Barros, Aluisio J. D. Toilet training: methods, parental expectations and associated dysfunctions Jornal de Pediatria, vol. 84, núm. 1, enero-febrero, 2008, pp. 9-17 Sociedade Brasileira de Pediatria Porto Alegre, Brasil Available in: http://www.redalyc.org/articulo.oa?id=399738157004 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative 0021-7557/08/84-01/9 Jornal de Pediatria Copyright © 2008 by Sociedade Brasileira de Pediatria REVIEW ARTICLE Toilet training: methods, parental expectations and associated dysfunctions Denise M. Mota,1 Aluisio J. D. Barros2 Abstract Objective: To review both the scientific literature and lay literature on toilet training, covering parents’ expectations, the methods available for achieving bladder and bowel control and associated morbidities. Sources: Articles published between 1960 and 2007, identified via the MEDLINE, Cochrane Collaboration, ERIC, Web of Science, LILACS and SciELO databases plus queries on the Google search engine; a search of related articles, references of articles, by author and of pediatrics societies. A total of 473 articles were examined and 85 of these were selected for this review. Summary of the findings: Parents have unrealistic expectations about the age at which diapers can be withdrawn, not taking child development into account. Toilet training strategies have not changed over recent decades, and in the majority of countries the age at which children are trained has been postponed. -

1 Robert P. Dillard, MD
Robert P. Dillard, MD Division of Pediatric Gastroenterology University of Kentucky Lexington, KY 1 Guideline for Constipation in Infants and Children Know approach to constipated infant & child Know organic causes of constipation Understand that functional constipation is common Know major historical and physical finding to differenti a te ftilfunctional from “i”“organic” constipation Know treatment 2 CC: “Something’s wrong with his bowels” HPI: Daily multiple episodes of stool into underwear Sticky, stains No regular BM Recalls huge stools (clogged toilet) Blood seen Used to stand in corner and hide Red face/wriggle Problem 1st around toilet training time Punishing done at day care Worried about starting school PMA Normal P/L/D/neonatal infancy Straining with change to formula ROS Generally healthy Normal growth No neurological/developmental problems Urination normal FH ‐ Mother has problem with constipation SH –parent, dog, cat, alligator, sister 3 Physical Exam Healthy appearing 50% ht/wt General exam nl Abdomen – distended, bowel sound present, palpable movable masses Back –intact, no hair tuff or pigmentation, buttocks normal contour Spine /sacrum– intact Perineum –anus normally placed, smear stool seen, stained underwear, normal sensation, normal anal wink, flattened anal canal, dilated rectum/hard stool mass, no urge to defecate moments after rectal exam, occult blood neg Neurological – cognition/behavior/tendon/cutaneous reflexes/tone –nl 4 SlStruggles to have BM Have to help Cries with pain Reports pain Didn’t help to spank Outcast at school Stomach ache Poor appetite 5 3% Visits: General Pediatric Clinic 10 ‐ 25% Visits: Pediatric GI Feels like 90% Laxatives $225 million/year business Estimated 1.5% of second grade school children are encopretic 3% of large clinic OPD pediatric visits are for constipation and soiling 10‐25% of pediatri c GI clin ic viiisits for constiiipation and soiling* *PCNA Vol. -

Toileting Policy
Tocumwal Pre-School SECTION: 2 - Children’s Health and Safety POLICY NO: 2.6.2 POLICY: Toileting REVIEW DATE: 7/6/18 DATE OF APPROVAL: Introduction Children can have specific health requirements and these often change over time and vary due to a range of factors. The centre will work closely with children and families to ensure that we support families and meet children’s specific requirements for comfort and welfare in relation to daily routines including toileting. The centre will minimise the spread and risks of infectious diseases between children, other children and staff, by maintaining high standards of hygiene. Effective hygiene practices assist significantly in reducing the likelihood of children becoming ill due to cross-infection or as a result of exposure to materials, surfaces, body fluids or other substances that may cause infection or illness. Goals – What are we going to do? Ensure that the dignity of children is upheld, and that family practices and beliefs are respected when toileting or changing children. Consistent approaches between the home and the education and care environment allow children to gain confidence in their abilities and develop independence with their toileting skills. This consistent approach allows children to identify appropriate hygiene and toileting practices that will reduce the spread of infectious disease. Toileting facilities and practices that ensure ease of access, good supervision and support for children will enable children to develop toileting skills within a safe and secure environment. Routine and self-help activities enable educators to promote children’s learning, meet individual needs and develop strong trusting relationships with children. -
2015-2016 SHM Parent Handbook (10-15-15)
PARENT HANDBOOK 2015 – 2016 Academic Year Sunny Hollow Montessori 636 South Mississippi River Boulevard Saint Paul, MN 55116 Phone: 651-690-2307 Fax: 651-690-0684 sunnyhollow.org Revised 10/15/15 Parent Handbook WELCOME We are delighted that your family is a part of the Sunny Hollow Montessori community! This handbook provides you with the tools you need to be informed and connected at Sunny Hollow. Included are the guidelines, policies, and procedures for families. If you have any questions, please ask our administrative staff. Here’s to a strong year of partnership, joy, and learning at Sunny Hollow! CHANGES TO THIS HANDBOOK We have revised the 2015-2016 Parent Handbook to make it easier to use and to include our new Toddler Community. Please review and let us know if you have questions. For returning families, here are important changes to drop-off times: • All Casa and Elementary children are expected to be in the school by 8:30 am. • Casa staff will now greet children from 8:20 to 8:30 am. • Car drop-off is now from 8:20 to 8:30 am. 2 Parent Handbook TABLE OF CONTENTS WELCOME 2 OVERVIEW OF SUNNY HOLLOW MONTESSORI 5 Our Mission 5 Our Vision 5 Our Values 5 Our History 5 Accreditation, Licensing, and Associations 6 Non-Discrimination Policy 6 STAFF DIRECTORY 7 WHO TO CONTACT WITH QUESTIONS 9 BOARD OF TRUSTEES 10 THE MONTESSORI METHOD 11 MONTESSORI EDUCATION PROGRAMS 13 Toddler Community (16 to 33 Months) 13 Casa (33 Months to 6 years) 16 Elementary (Grades 1 to 6) 19 CASA AND ELEMENTARY EXTRA CURRICULAR PROGRAMS 22 Foreign Language -

TOILET TRAINING and ENCOPRESIS
ENCOPRESISENCOPRESIS Ricardo A. Caicedo, M.D. University of Florida Pediatric Gastroenterology Revised July 2005 ENCOPRESISENCOPRESIS • Introduction – Definition – Classification •Elements – Constipation – Stool Retention – Incontinence – Development and Behavior • Toilet training • Other potentiators • Evaluation • Management ENCOPRESIS1 • Repeated passage of feces into inappropriate places such as clothing or floor •Age >4 years – chronological or mental • Involuntary or intentional • Not due to an organic disorder or medication • At least once a month for > 3 months 1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 4th ed. (DSM-IV). Washington, DC: American Psychiatric Association; 1994:106-110. ENCOPRESIS • Affects 1-3 % of children • Boys > girls (estimated at 4-6:1)2 • Most accidents occur later in day (3-7 PM)2 • Primary (continuous): child has never completed toilet training for stool • Secondary (discontinuous): toilet trained child regresses to incontinence 2. Levine MD. Encopresis. In: Levine MD, Carey WB, Crocker AC, eds. Developmental-Behavioral Pediatrics. Philadelphia: Saunders; 1983: 586-95. ENCOPRESIS • Retentive (80-95%): involves – Constipation – Stool retention – Overflow incontinence • Nonretentive or “solitary”(5-20%)3: – No constipation or overflow incontinence – Stool toileting refusal/resistance/”phobia” – Often manifestation of emotional disturbance • Virtually all children with encopresis retain stools at least intermittently4 3. Kuhn BR et al. Am Family Physician 1999; 59(8): 312-17. 4. Levine MD. Pediatr Rev. 1981; 2:285. EPIDEMIOLOGY5 INCIDENCE Overall children 1.5 % • Incidence & prevalence decrease with age School children 1.5-7.5%13 aged 6-12 • More prevalent in boys 4 y/o 2.8 % • Prevalence reverses in 5 y/o 2.2 % elderly 6 y/o 1.9 % • 16% of affected 7 y/o 1.5 % children have one Gen Peds clinics 3.0 % affected parent Child Ψoutpts. -

Iowa Family Day Care Handbook
DOCUMENT RESUME ED 286 603 PS 016 794 AUTHOR Holt, Bess Gene; Karas, Shirley C. TITLE Iowa Family Day Care Handbook. 3rd Edition. INSTITUTION Iowa State Univ. of Science and Technology, Ames. Dept. of Child Development. SPONS AGENCY Iowa State Dept. of Human Services, Des Moines. PUB DATE 86 GRANT IDHS-PL-98-473 NOTE 215p. AVAILABLE FROM Child Development Training Program, Department of Child Development, Iowa State University, Ames, IL 50011 ($7.00). PUB TYPE Guides Non-Classroom Use (055) EMS PRICE MF01/PC09 Plus Postage. DESCRIPTORS Administrator Guides; *Business Skills; Community Resources; Discipline; Early Childhood Education; *Educational Planning; *Family Day Care; First Aid; Health; Nutrition; Safety; Scheduling; State Programs; Teacher Burnout IDENTIFIERS *Iowa ABSTRACT The purposes of this handbook are (1) to help individuals who are thinking about becoming family day care providers decide whether the profession is appropriate for themselves and their families, and (2) to present ideas for setting up and maintaining a family day care home that provides high quality service to families, 4 developmental learning environment to children, and business success to providers. Chapter 1 offers an introduction to family day care in Iowa. Chapter 2 focuses on starting and maintaining a family day care business. Chapter 3 discusses the home as a child care and learning environment. Chapter 4 explores aspects of the relationship between parent and cz.regiver. Chapter 5 discusses causes of behavior, individual differences, learning, development, and meeting children's special needs. Chapter 6 offers suggestions for guiding and disciplining children. Chapter 7 concerns scheduAing and planning learning and care activities. -
How to Clean and Sanitize a Bedside Commode
How to Clean and Sanitize a Bedside Commode Cleaning Keeping a bedside commode clean and odor free doesn't have to be a chore. Much like your toddler's old potty chair, bedside commodes are relatively easy to clean. All it takes is a pair of disposable gloves, Clorox wipes, and a can of Lysol aerosol spray. Step 1: Put on a pair of disposable gloves. Step 2: Place the lid on the waste container and carry with both hands to the bathroom. (For models with a carrying handle, it's a wise practice to support the bucket with one hand in case the handle detaches). Lift up the toilet seat and pour the contents into the toilet. Step 3: Rinse the bucket with some warm water and pour into the toilet. This will help to remove residual amount of waste. Step 4: Wipe down the inside of the bucket with Clorox wipes, disposing of the wipes in a separate container. For the frugally minded, a less expensive solution is to make your own cleaning agent by mixing up a pint of warm water with a tablespoons of bleach, which can then be decanted in a spray bottle. Spray the solution directly onto a paper towel which can then be used to wipe down the inside of the waste bucket and the underside of the lid. Take care not to spill any of the solution on your clothes or the bathroom rug! Step 5: Rinse the waste pail thoroughly with warm water and dry with a clean rag. Step 6: Spray the inside of the container with Lysol spray, and then place the bucket back under the commode. -

Compendium of Sanitation Technologies in Emergencies
Compendium 1st Edition of Sanitation Technologies in Emergencies Compendium 1st Edition of Sanitation Technologies in Emergencies Robert Gensch (GTO), Amy Jennings (BORDA), Samuel Renggli (Eawag), Philippe Reymond (Eawag) We would like to thank the following individuals and their organisations/institutions for their invaluable contributions to this publication: Djilali Abdelghafour, Nienke Andriessen, Leonellha Barreto-Dillon, Andy Bastable, Magdalena Bäuerl, Benjamin Bernan- dino, Damian Blanc, Franck Bouvet, Patrick Bracken, Chris Buckley, Marc-Andre Bünzli, Chris Canaday, Daniel Clauss, Benjamin Dard, Malcolm Dickson, Paul Donahue, Georg Ecker, Miriam Englund, Marta Fernández Cortés, Suzanne Ferron, Claire Furlong, Sergio Gelli, Feline Gerstenberg, Moritz Gold, Celia González Otálora, Peter Harvey, Oliver Hoffmann, Tineke Hooijmans, Andrews Jacobs, Heidi Johnston, Christopher Kellner, Anthony Kilbride, Sasha Kramer, Jenny Lamb, Günther Langergraber, Anne Lloyd, Andreas Ludwig, Christoph Lüthi, Saskia Machel, Grover Mamani, Adeline Mertenat, Mona Mijthab, Alexander Miller, Patrice Moix, Paolo Monaco, Bella Monse, Hans-Joachim Mosler, Burt Murray, Arne Pane sar, Thilo Panzerbieter, Jonathan Parkinson, Dominique Porteaud, Nick Preneta, Torsten Reckerzügl, Bob Reed, Stefan Reuter, Romain Revol, Nina Röttgers, Johannes Rück, Vasco Schelbert, Jan-Christoph Schlenk, Jan-Hendrik Schmidt, Stephanie Schramm, Jan Spit, Haakon Spriewald, Steve Sugden, Annkatrin Tempel, Elisabeth Tilley, Erika Trabucco, Tobias Ulbrich, Lukas Ulrich, Claudio Valsangiacomo, -

Sustainability Report 2007-2008 Absorbent Hygiene Products
Sustainability Report 2007-2008 Absorbent Hygiene Products Prepared by: The Absorbent Hygiene Products Manufacturers Committee of EDANA Foreword from the Chairman In 2007, the year of Europe’s 50th birthday, we are delighted to present EDANA’s second Sustainability Report, an initiative of our Absorbent Hygiene Products Manufacturers Committee’s (HAPCO) Sustainability and Environmental Working Group. In the same year that the Treaty of Rome was signed, a Swedish firm, building on the first disposable diaper developments of the 1940s, developed a 2-piece diaper, which consisted of a disposable wad of shredded paper pulp covered with gauze which was inserted into reusable plastic pants. Heralded by mothers at the time as one of the greatest inventions of the 20th century, parents today can now enjoy the benefits of fifty years of research & development and innovation of this life-changing product, which has brought huge benefits to society in terms of hygiene, health, comfort and convenience. This edition of the Sustainability Report is an update of the 2005 Report rather than a completely new report. We have sought to extend the amount of information available within the public domain about our industry and its impact on social, environmental and economic aspects of life in modern society. Our ongoing commitment means that we are continuously improving our sustainability performance and we are able to update the information contained in the 2005 Report with data from 2005 and 2006. We have also extended this report to contain data on the feminine care category of absorbent hygiene products; that is sanitary pads, pantyliners and tampons. -

Early Childhood Visits 1 Through 4 Years
Early Childhood Visits 1 Through 4 Years BFG 4TH ED.indb 501 1/20/17 2:47 PM BFG 4TH ED.indb 502 1/20/17 2:47 PM Early Childhood 12 Month Visit Context The 12-month-old stands proudly, somewhat bow- parents’ ability to let go, permit independence, and legged, belly protruding. Walking, one of the most enjoy aspects of his behavior that are out of their exciting developmental milestones, occurs around direct control. The toddler’s messy attempts to feed the toddler’s first birthday, bringing with it increas- himself can be difficult for his parents as they sort EARLY CHILDHOOD EARLY ing independence. During the first year of life, the out their own desire for order and neatness with 12 MONTH VISIT infant was rarely in conflict with his environment. his need for self-care. He might have been demanding when he cried, Fortunately, the toddler is endowed with a social he required considerable care, and he changed the feedback loop to recognize both pleasure and dis- balance in the family. However, he spent most of pleasure from significant caregivers. Adults build his first year getting to know and trust his parents on this characteristic by providing appropriate and his environment. As a toddler, he becomes responses to a toddler’s actions. Adult laughter increasingly competent in acting upon the world during a well-played game of peekaboo holds around him, all on his own. His world broadens, the key to future good times in other interactive bringing both excitement and challenge. games, and turning away, ignoring, or expressing Autonomy and independent mobility are develop- displeasure at a plate of food thrown on the floor, mental achievements of which the parents and which sends a message that this behavior is not toddler are justifiably proud, but the toddler acceptable, helps prevent later disruptive behaviors.