Climate Change and Health in West Africa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
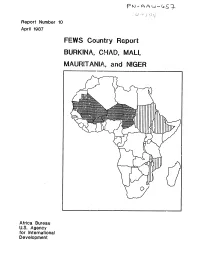
FEWS Country Report BURKINA, CHAD, MALI, MAURITANIA, and NIGER
Report Number 10 April 1987 FEWS Country Report BURKINA, CHAD, MALI, MAURITANIA, and NIGER Africa Bureau U.S. Agency for International Development Summary Map __ Chad lMurltanl fL People displaced by fighting High percentage of population have bothL.J in B.E.T. un~tfood needsa nd no source of income - High crop oss cobied with WESTERN Definite increases in retes of malnutrition at CRS centers :rom scarce mrket and low SAHARA .ct 1985 through Nov 196 ,cash income Areas with high percentage MA RTAI of vulnerable LIBYA MAU~lAN~A/populations / ,,NIGER SENEGAL %.t'"S-"X UIDA Areas at-risk I/TGI IEI BurkinaCAMEROON Areas where grasshoppers r Less than 50z of food needs met combined / CENTRAL AFRICAN would have worst impact Fi with absence of government stocks REPLTL IC if expected irdestat ions occur W Less than r59 of food needs met combined ith absence of government stocks FEYIS/PWA. April 1987 Famine Early Warning System Country Report BURKINA CHAD MALI MAURITANIA NIGER Populations Under Duress Prepared for the Africa Bureau of the U.S. Agency for International Development Prepared by Price, Williams & Associates, Inc. April 1987 Contents Page i Introduction 1 Summary 2 Burkina 6 Chad 9 Mali 12 Mauritania 18 Niger 2f FiAures 3 Map 2 Burkina, Grain Supply and OFNACER Stocks 4 Table I Burkina, Production and OFNACER Stocks 6 Figure I Chad, Prices of Staple Grains in N'Djamcna 7 Map 3 Chad, Populations At-Risk 10 Table 2 Mali, Free Food Distribution Plan for 1987 II Map 4 Mali, Population to Receive Food Aid 12 Figure 2 Mauritania, Decreasing -

Phase 2 Environmental Impact Assessment On-Site Mine Process
Tasiast Mauritanie Limited SA Tasiast Gold Mine Expansion Project Phase 2: On-Site Mine, Process and Infrastructure Environmental Impact Assessment Final 30 March 2012 Prepared for Prepared for Tasiast Mauritanie Limited SA Tasiast Gold Mine Expansion Project Revision Schedule Phase 2 Environmental Impact Assessment 30 March 2012 Final Rev Date Details Prepared by Reviewed by Approved by 01 21/12/2011 Draft for review Reine Loader Julie Raynor Russell Foxwell Environmental Consultant Associate Associate Fraser Paterson Associate 02 01/03/2012 Draft for Reine Loader Julie Raynor Russell Foxwell translation Environmental Consultant Associate Associate Fraser Paterson Associate 03 30/03/2012 FINAL Reine Loader Fraser Paterson Russell Foxwell Environmental Consultant Associate Associate URS Infrastructure & Environment UK Limited 6-8 Greencoat Place London SW1P 1PL United Kingdom Tel +44 (0) 20 7798 5000 Fax +44 (0) 20 7798 5001 www.ursglobal.com Tasiast Mauritanie Limited SA Tasiast Gold Mine Expansion Project Limitations URS Infrastructure & Environment UK Limited (“URS”) (formerly URS Scott Wilson Ltd) has prepared this Report for the use of Tasiast Mauritanie Limited SA (“Client”) in accordance with the Agreement under which our services were performed. No other warranty, expressed or implied, is made as to the professional advice included in this Report or any other services provided by URS. Notwithstanding anything to the contrary, URS acknowledge that the Report may be disclosed by the Client to any third party, including members of the public for the specific purposes which have been advised to URS. URS shall not have any liability to any third parties for the unauthorised copying and any subsequent reliance on this Report. -

En Téléchargeant Ce Document, Vous Souscrivez Aux Conditions D’Utilisation Du Fonds Gregory-Piché
En téléchargeant ce document, vous souscrivez aux conditions d’utilisation du Fonds Gregory-Piché. Les fichiers disponibles au Fonds Gregory-Piché ont été numérisés à partir de documents imprimés et de microfiches dont la qualité d’impression et l’état de conservation sont très variables. Les fichiers sont fournis à l’état brut et aucune garantie quant à la validité ou la complétude des informations qu’ils contiennent n’est offerte. En diffusant gratuitement ces documents, dont la grande majorité sont quasi introuvables dans une forme autre que le format numérique suggéré ici, le Fonds Gregory-Piché souhaite rendre service à la communauté des scientifiques intéressés aux questions démographiques des pays de la Francophonie, principalement des pays africains et ce, en évitant, autant que possible, de porter préjudice aux droits patrimoniaux des auteurs. Nous recommandons fortement aux usagers de citer adéquatement les ouvrages diffusés via le fonds documentaire numérique Gregory- Piché, en rendant crédit, en tout premier lieu, aux auteurs des documents. Pour référencer ce document, veuillez simplement utiliser la notice bibliographique standard du document original. Les opinions exprimées par les auteurs n’engagent que ceux-ci et ne représentent pas nécessairement les opinions de l’ODSEF. La liste des pays, ainsi que les intitulés retenus pour chacun d'eux, n'implique l'expression d'aucune opinion de la part de l’ODSEF quant au statut de ces pays et territoires ni quant à leurs frontières. Ce fichier a été produit par l’équipe des projets numériques de la Bibliothèque de l’Université Laval. Le contenu des documents, l’organisation du mode de diffusion et les conditions d’utilisation du Fonds Gregory-Piché peuvent être modifiés sans préavis. -

Monographie Des Communes Des Départements De L'atlantique Et Du Li
Spatialisation des cibles prioritaires des ODD au Bénin : Monographie des communes des départements de l’Atlantique et du Littoral Note synthèse sur l’actualisation du diagnostic et la priorisation des cibles des communes Monographie départementale _ Mission de spatialisation des cibles prioritaires des ODD au Bénin _ 2019 1 Une initiative de : Direction Générale de la Coordination et du Suivi des Objectifs de Développement Durable (DGCS-ODD) Avec l’appui financier de : Programme d’appui à la Décentralisation et Projet d’Appui aux Stratégies de Développement au Développement Communal (PDDC / GIZ) (PASD / PNUD) Fonds des Nations unies pour l'enfance Fonds des Nations unies pour la population (UNICEF) (UNFPA) Et l’appui technique du Cabinet Cosinus Conseils Monographie départementale _ Mission de spatialisation des cibles prioritaires des ODD au Bénin _ 2019 2 Tables des matières LISTE DES CARTES ..................................................................................................................................................... 4 SIGLES ET ABREVIATIONS ......................................................................................................................................... 5 1.1. BREF APERÇU SUR LES DEPARTEMENTS DE L’ATLANTIQUE ET DU LITTORAL ................................................ 7 1.1.1. INFORMATIONS SUR LE DEPARTEMENT DE L’ATLANTIQUE ........................................................................................ 7 1.1.1.1. Présentation du Département de l’Atlantique ...................................................................................... -

PIF) Entry – Full Sized Project – GEF - 7 Development of an Integrated System to Promote the Natural Capital in the Drylands of Mauritania
5/5/2020 WbgGefportal Project Identification Form (PIF) entry – Full Sized Project – GEF - 7 Development of an integrated system to promote the natural capital in the drylands of Mauritania Part I: Project Information GEF ID 10444 Project Type FSP Type of Trust Fund GET CBIT/NGI CBIT NGI Project Title Development of an integrated system to promote the natural capital in the drylands of Mauritania Countries Mauritania Agency(ies) IUCN Other Executing Partner(s) Executing Partner Type CNEOZA, Ministère de l'Environnement et du Développement Durable Government https://gefportal2.worldbank.org 1/51 5/5/2020 WbgGefportal GEF Focal Area Land Degradation Taxonomy Climate Change Adaptation, Climate Change, Focal Areas, Climate resilience, Livelihoods, Disaster risk management, Land Degradation, Sustainable Land Management, Drought Mitigation, Integrated and Cross-sectoral approach, Improved Soil and Water Management Techniques, Sustainable Livelihoods, Sustainable Pasture Management, Ecosystem Approach, Restoration and Rehabilitation of Degraded Lands, Community-Based Natural Resource Management, Sustainable Agriculture, Income Generating Activities, Food Security, Land Degradation Neutrality, Land Productivity, Influencing models, Transform policy and regulatory environments, Strengthen institutional capacity and decision-making, Convene multi-stakeholder alliances, Private Sector, Stakeholders, Individuals/Entrepreneurs, Large corporations, SMEs, Beneficiaries, Non-Governmental Organization, Civil Society, Community Based Organization, Participation, -

Poverty and the Struggle to Survive in the Fuuta Tooro Region Of
What Development? Poverty and the Struggle to Survive in the Fuuta Tooro Region of Southern Mauritania Dissertation Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Christopher Hemmig, M.A. Graduate Program in Near Eastern Languages and Cultures. The Ohio State University 2015 Dissertation Committee: Sabra Webber, Advisor Morgan Liu Katey Borland Copyright by Christopher T. Hemmig 2015 Abstract Like much of Subsaharan Africa, development has been an ever-present aspect to postcolonial life for the Halpulaar populations of the Fuuta Tooro region of southern Mauritania. With the collapse of locally historical modes of production by which the population formerly sustained itself, Fuuta communities recognize the need for change and adaptation to the different political, economic, social, and ecological circumstances in which they find themselves. Development has taken on a particular urgency as people look for effective strategies to adjust to new realities while maintaining their sense of cultural identity. Unfortunately, the initiatives, projects, and partnerships that have come to fruition through development have not been enough to bring improvements to the quality of life in the region. Fuuta communities find their capacity to develop hindered by three macro challenges: climate change, their marginalized status within the Mauritanian national community, and the region's unfavorable integration into the global economy by which the local markets act as backwaters that accumulate the detritus of global trade. Any headway that communities can make against any of these challenges tends to be swallowed up by the forces associated with the other challenges. -

Project for the Establishment and Management of Marine Protected
Distr. Restricted UNITED NATIONS INDUSTRIAL DEVELOPMENT ORGANIZATION Original Version: French PROJECT / PROGRAMME TO COMBAT THE LOSS OF LIVING RESOURCES AND THE DEGRADATION OF THE COASTAL AREA IN THE GUINEA CURRENT LAEGE MARINE ECOSYSTEM AREA Contract N° GP/RAF/04/004/11-B2 PROJECT FOR THE ESTABLISHEMENT AND MANAGEMENT OF MARINE PROTECTED AREAS IN BENIN (Pilot Project in the 16 Guinea Current Large Marine Ecosystem countries) Prepared for the Governments of Angola, Benin, Cameroon, Congo, Cote d’Ivoire, Gabon, Ghana, Guinea, Equatorial Guinea, Guinea Bissau, Liberia, Nigeria, the Democratic Republic of Congo, Sao Tome & Principe, Sierra Leone, and Togo by the United Nations Industrial Development Organization (UNIDO) with the cooperation of the United Nations Environmental Programme (UNEP). FINAL REPORT By CEDED-ONG Project Director: Christian Susan, Environmental Management Branch, Program Development and Technical Cooperation Division This document has not yet been officially edited List of acronyms and abbreviations ABE Agence Béninoise pour l’Environnement (Benin Environmental Agency) MPA Marine Protected Area CA Chef d’Arrondissement CBRST Centre Béninois de Recherche Scientifique et Technique (Benin Scientific and Technical Research Center) CEDED Centre pour l’Environnement et le Développement Durable (Environment and Sustainable Development Research Center) CRHOB Centre de Recherche Halieutique et Océanologiques du Bénin (Benin Halieutic and Oceanographic Research Center) CV Chef de Village (Village Chief) DDEPN Direction Départementale -

Sdlao Uemoa Uicn
0° 1° E 2° E Kouffo Sakété Adjohoun ! ! Mono Lokossa Allada ! ! Haho Athiémè Tagbligbo ! Dangbo ! Bopa ! ! Akpro-MissérétéAvrankou ! ! Adjara ! Zio BENIN Foret d'Eto Sè Tori-Bossito ! ! Porto-Novo Lac Ahémé Lac ! ! Ganvié Akodéha.! Abomey-Calavi! .! ! ! Aguégué Kpomasse ! ! Tohouè Vo Ativé Zooti Lac Nokoué Djérèbé! Tsevie ! ! Kétonou ! Kevé ! Atitogon ! ! ! Comé Agatogbo! ! ! Agbanto Ekpé Kpodji-Agué TOGO Akoumapé ! Vo Afouinmé ! ! ! ! Kraké !Sèmè-Kpodji! Hahatoé Vo Koutimé Ouidah ! ! Gbéhoué ! ! Avlékété Aklakou ! ·[ Vogan Anfoin ! ! ! Djégbadji ! COTONOU k Ganavé Djondji h Sevagan ! ! ! Wogba Avlo ! ! Zones Humides du Littoral du Togo Noépé ! ! Djablé .! Akoda ! Agoué Aképé ! ! Grand-Popo Dzodze ! ! Togoville ! ! ! Volta Lebe ! Gbodjomé ! Aného ! ! h Agbodrafo Kpong ·[ ! h k LOME ! Denu Aflao Akatsi ! ! Adiome ! Sogakope Tsiame ! ! Anyako Dabala ! 7° N ! 7° N Atiavi Keta Lagoon ! GHANA Kasseh .! [ ! ! Keta k Songaw Lagoon ! Oyibi .! ! Lekpoguno Lolonya ! ! Palm Point Anloga ! ! ! Dzita ! Old Ningo ! Ada-Foah Strogboe New Ningo ! k ! k ! Prampram ! Grove Point Tema k Bontrase h ! ·[ Asafo ! Oduponkpehé Swedru ! k ! Accra Point Afranse Bortianor .! k ! ! Densu ACCRA k delta ! Nyanyano Buduburam ! Feté ! Awutu Senya k Beraku Point ! Winneba ! Muni .! Winneba Point Lagoon k Apam Apam Point ! k REGIONAL SHORELINE MONITORING STUDY AND ! Mumford DRAWING UP A MANAGEMENT SCHEME FOR Babli Point ! !Akra THE WEST AFRICAN COASTAL AREA Tantum Country borders TYPOLOGY OF HUMAN LAND-USE SYSTEMS LESS THAN 1KM FROM SHORE ROAD NETWORK West African Major -

Partner Country Coverage
IMaD’s Lessons Learned Luis Benavente MD, MS CORE’s webinar August 29, 2012 Insert title here Country Number of health Health workers trained in topics related to malaria diagnosis as of June 2012 total N facility visits trained Baseline Outreach How to TOT and On-the- job Database National External Malaria all assesmt. of training & perform supervi- training data entry, Malaria competency micros- Diagnostic support laboratory sors during mainte- Slide sets, assess- copy and capabilities supervision assessments OTSS OTSS nance NAMS ments RDTs Angola 5 6 2 18 12 0 0 12 26 70 Benin 11 409 2 30 1671 9 0 0 40 1,752 Burundi 18 0 0 0 0 0 0 0 0 0 DR Congo 0 0 0 23 0 0 0 0 74 97 Ethiopia 4 0 4 0 0 0 13 17 0 34 Ghana 37 1109 37 46 3704 10 10 6 40 3,853 Guinea Con. 11 0 11 0 0 0 0 0 20 31 Kenya 1192 52 1192 66 312 0 0 37 67 1,674 Liberia 8 200 8 35 975 11 0 7 141 1,177 Madagascar 50 31 50 18 18 0 0 0 23 109 Malawi 14 521 14 75 1132 3 0 0 64 1,288 Mali 5 172 5 24 1188 4 0 0 40 1,261 Nigeria 40 0 0 0 0 0 0 26 0 26 Zambia 6 278 6 12 1733 5 0 9 92 1,857 Total 1,401 2,778 1,331 347 10,745 42 23 114 627 13,229 Proportion of febrile episodes caused by Plasmodium falciparum Source: d’Acremont V, Malaria Journal, 2010 Better testing is needed to assess the impact of malaria control interventions Parasitemia prevalence after IRS, countries with at least biennial monitoring 80% Namibia-C Zimbabwe Moz-Maputo 70% 60% 50% 40% 30% 20% 10% 0% 1948 1950 1952 1954 1956 1958 1960 1962 1964 1966 1968 CORE’s Surviving Malaria Pathway ITNs - Bednet use Caretaker recognizes -
A Sociolinguistic Survey of the Gbe Language Communities of Benin and Togo Volume 4 Xwela Language Area
DigitalResources Electronic Survey Report 2011-016 ® A sociolinguistic survey of the Gbe language communities of Benin and Togo Volume 4 Xwela language area Bonnie J. Henson Eric C. Johnson Angela Kluge A sociolinguistic survey of the Gbe language communities of Benin and Togo Volume 4 Xwela language area Bonnie J. Henson Eric C. Johnson Angela Kluge SIL International® 2011 SIL Electronic Survey Report 2011-016, March 2011 Copyright © 2011 Bonnie J. Henson, Eric C. Johnson, Angela Kluge and SIL International® All rights reserved A SOCIOLINGUISTIC SURVEY OF THE GBE LANGUAGE COMMUNITIES OF BENIN AND TOGO Series editor: Angela Kluge Gbe language family overview (by Angela Kluge) Volume 1: Kpési language area (by Evelin I. K. Durieux-Boon, Jude A. Durieux, Deborah H. Hatfield, and Bonnie J. Henson) Volume 2: Ayizo language area (by Deborah H. Hatfield and Michael M. McHenry) Volume 3: Kotafon language area (by Deborah H. Hatfield, Bonnie J. Henson, and Michael M. McHenry) Volume 4: Xwela language area (by Bonnie J. Henson, Eric C. Johnson, Angela Kluge) Volume 5: Xwla language area (by Bonnie J. Henson and Angela Kluge) Volume 6: Ci language area (by Bonnie J. Henson) Volume 7: Defi language area (by Eric C. Johnson) Volume 8: Saxwe, Daxe and Se language area (by Eric C. Johnson) Volume 9: Tofin language area (by Gabi Schoch) Volume 10: Gbesi language area (by Gabi Schoch) ii Contents Abstract 1. Introduction 2. Background 2.1. Language name and classification 2.2. Language area 2.3. Population 2.4. History of migration 2.5. Presence of other ethnic groups 2.6. -

Villages Et Quartiers De Ville (Cartes De Districts)
REPUBLIQUE POPULAIRE DU BENIN BUREAU CENTRAL DU RECENSEMENT PRESIDENCE DE LA REPUBLIQUE UNITE D'ANALYSE ET DE MINISTERE DU PLAN ET DE LA STATISTIQUE FORMATION DEMOGRAPHIQUES INSTITUT NATIONAL DE LA STATISTIQUE ET DE L'ANALYSE ECONOMIQUE LA POPULATION de L'ATLANTIQUE Villages et Quartiers de Ville (Cartes de Districts) Novembre 1988 REPUBLIQUE POPULAIRE DU BENIN BUREAU CENTRAL DU RECENSEMENT PRESIDENCE DE LA REPUBLIQUE UNITE D'ANALYSE ET DE MINISTERE DU PLAN ET DE LA STATISTIQUE FORMATION DEMOGRAPHIQUES INSTITUT NATIONAL DE LA STATISTIQUE ET DE L'ANALYSE ECONOMIQUE RECENSEMENT GENERAL DE LA POPULATION ET DE L'HABITATION (MARS 1979) LA POPULATION de L'ATLANTIQUE Villages et Quartiers de Ville (Cartes de Districts) Novembre 1988 DIm D)':"/) A T l B R B S Papa PRESENTATION GEOGRAPHIQUE i à iv II. LISTE DES TABLEAUX NOMBRE DE MENAGES ET LEUR POPULATION SELON LES DISTRICTS, LES COMMUNES ET LES VILLAGES POUR LA PROVINCE DE L'ATLANTIQUE Papa TABLEAU 1. District rural d'Abomey-Calavi 1 TABLEAU 2. District rural d'Allada 4 TABLEAU 3. District urbain de Cotonou l 7 TABLEAU 4. District urbain de Cotonou 2 8 TABLEAU 5. District urbain de Cotonou 3 9 TABLEAU 6. District urbain de Cotonou 4 10 TABLEAU 7. District urbain de Cotonou 5 11 TABLEAU 8. District urbain de Cotonou 6 12 TABLEAU 9. District rural de Kpomassè 13 TABLEAU 10. District rural de Ouidah 16 TABLEAU 11. District rural lacustre de So-Ava 18 TABLEAU 12. District rural de Torro 20 TABLEAU IJ. District rural de Torri-BossUo 22 "- \~ TABLEAU 14. District rural de Zè 24 III. -

Climate Change Adaptation and Livelihoods in Three Arid Regions of Mauritania
GEF Portal Climate change adaptation and livelihoods in three arid regions of Mauritania Part I: Project Information GEF ID 10103 Project Type FSP Type of Trust Fund LDCF Project Title Climate change adaptation and livelihoods in three arid regions of Mauritania Countries Mauritania, Agency(ies) UNEP, Other Executing Partner(s): Executing Partner Type Government GEF Focal Area Climate Change Taxonomy Focal Areas, Climate Change, Climate Change Adaptation, Adaptation Tech Transfer, National Adaptation Programme of Action, Complementarity, Sea- level rise, Livelihoods, Climate resilience, National Adaptation Plan, Small Island Developing States, Disaster risk management, Least Developed Countries, Innovation, Private sector, Ecosystem-based Adaptation, Community-based adaptation, Climate finance, Climate information, Influencing models, Strengthen institutional capacity and decision-making, Stakeholders, Beneficiaries, Local Communities, Gender Equality, Gender Mainstreaming, Sex-disaggregated indicators, Gender-sensitive indicators, Gender results areas, Capacity Development, Access and control over natural resources, Capacity, Knowledge and Research, Knowledge Generation, Workshop, Seminar, Master Classes, Training, Course, Professional Development, Climate Finance (Rio Markers), Climate Change Adaptation 2, Climate Change Mitigation 0, Mainstreaming adaptation, Participation and leadership Duration 48 In Months Agency Fee($) 419,540 Submission Date 10/4/2018 A. Indicative Focal/Non-Focal Area Elements Programming Directions Trust Fund