Drug Utilisation Evaluation Study on Patients with Diabetes Mellitus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Exploring the Role of Malaysian Student's Intrapreneurial Self
sustainability Article Exploring the Role of Malaysian Student’s Intrapreneurial Self-Capital in the Relationship between Satisfaction with Life, Academic Performance, and Flourishing Chua Bee Seok 1, Pan Lee Ching 1 and Rosnah Ismail 2,* 1 Faculty of Psychology and Education, Universiti Malaysia Sabah, Kota Kinabalu 88400, Malaysia; [email protected] (C.B.S.); [email protected] (P.L.C.) 2 Department of Psychology, Faculty of Allied Health Sciences, University of Cyberjaya, Cyberjaya 63000, Malaysia * Correspondence: [email protected] Received: 21 November 2019; Accepted: 10 January 2020; Published: 13 January 2020 Abstract: Intrapreneurial self-capital is the construct coined by Di Fabio as a core of individual resources used to cope with career and life construction challenges. In this study, we used the model of Individual Differences in Evaluating Life Satisfaction (IDELS) to examine the mediating role of intrapreneurial self-capital in the relationship between life satisfaction and flourishing among Malaysian undergraduate students. The Intrapreneurial Self-Capital Scale (ISCS), Satisfaction with Life Scale (SWLS), and Flourishing Scale were administered to 665 undergraduate students from one of the public universities in Kota Kinabalu, Sabah, Malaysia. The results reported a significant direct effect of student satisfaction with life to flourishing. A significant path coefficient was also found from satisfaction with life and student academic performance to intrapreneurial self-concept providing the support that student satisfaction with life and academic performance has a positive effect on their intrapreneurial self-concept. The coefficients from intrapreneurial self-concept to flourishing was also significant. This provides initial support that an intrapreneurial self-concept may have a positive mediating effect on the relationship between satisfaction with life, academic performance, and flourishing. -

The Effects of Piper Sarmentosum Aqueous Extracts on Zebrafish
www.nature.com/scientificreports OPEN The efects of Piper sarmentosum aqueous extracts on zebrafsh (Danio rerio) embryos and caudal fn tissue regeneration Intan Zarina Zainol Abidin1*, Shazrul Fazry2, Nur Hidayah Jamar2, Herryawan Ryadi Ediwar Dyari3, Zaidah Zainal Arifn4, Anis Nabilah Johari5, Nur Suhanawati Ashaari6, Nor Azfa Johari6, Rohaya Megat Abdul Wahab7 & Shahrul Hisham Zainal Arifn5,6* In Malaysia, Piper sarmentosum or ‘kaduk’ is commonly used in traditional medicines. However, its biological efects including in vivo embryonic toxicity and tissue regenerative properties are relatively unknown. The purpose of this study was to determine zebrafsh (Danio rerio) embryo toxicities and caudal fn tissue regeneration in the presence of P. sarmentosum aqueous extracts. The phytochemical components and antioxidant activity of the extract were studied using GC–MS analysis and DPPH assay, respectively. Embryo toxicity tests involving survival, heartbeat, and morphological analyses were conducted to determine P. sarmentosum extract toxicity (0–60 µg/mL); concentrations of 0–400 µg/mL of the extract were used to study tissue regeneration in the zebrafsh caudal fn. The extract contained several phytochemicals with antioxidant activity and exhibited DPPH scavenging activity (IC50 = 50.56 mg/mL). Embryo toxicity assays showed that a concentration of 60 μg/mL showed the highest rates of lethality regardless of exposure time. Slower embryogenesis was observed at 40 µg/mL, with non-viable embryos frst detected at 50 µg/mL. Extracts showed signifcant diferences (p < 0.01) for tissue regeneration at all concentrations when compared to non-treated samples. In conclusion, Piper sarmentosum extracts accelerated tissue regeneration, and extract concentrations at 60 µg/mL showed the highest toxicity levels for embryo viability. -

Presentasi Lldikti VI 290321
Mengelola Kemitraan di Perguruan Tinggi Pengalaman Universitas Islam Indonesia Disampaikan pada Wiryono Raharjo FGD Implementasi Kerjasama Kampus Merdeka Wakil Rektor Bidang Kemitraan dan Kewirausahaan Pada Perguruan Tinggi Swasta Universitas Islam Indonesia Politeknik ATMI, 29 Maret 2021 Universitas Islam Indonesia 1 Materi presentasi dan diskusi • Memaknai kemitraan • Profil kemitraan UII • Mobilitas internasional • Studi kasus UII dalam membangun dan merawat kemitraan: • Program ACICIS • Erasmus+ CBHE • Akreditasi dan sertifikasi internasional • Kurikulum yang "MBKM friendly" • KUI sebagai unit pendukung Universitas Islam Indonesia 2 Memaknai kemitraan Universitas Islam Indonesia 3 Prinsip kemitraan PARTICIPATION ACCEPTANCE COMMUNICATION TRUST SHARE P A C T S PUNCTUAL ACCOUNTABLE COLLABORATE TRANSPARENT SUBMIT Universitas Islam Indonesia 4 Alasan memilih mitra (kasus UII) ALASAN PEMILIHAN MITRA Outbound Mobility Inbound Mobility Grant Opportunity Universitas Islam Indonesia 5 Kelompok mitra (kasus UII) Industri Pemerintah UII Akademik LSM Universitas Islam Indonesia 6 Profil kemitraan UII Universitas Islam Indonesia 7 Numbers of Domestic Partners Domes&c partners 49 37 21 3 Academic Government Industry Society/NGO Domes:c partners Universitas Islam Indonesia 8 Numbers of Global Partners Global partners 66 3 3 Academic Industry Society Global partners Universitas Islam Indonesia 9 Partnership in 2020 New and renewed partnership 22 11 Domes:c partners Global partners New and renewed partnership Universitas Islam Indonesia 10 Domestic -
Ytp) Lepasan Spm 2020
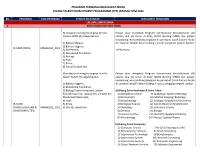
PROGRAM PEMBANGUNAN BAKAT MUDA YOUNG TALENT DEVELOPMENT PROGRAMME (YTP) LEPASAN SPM 2020 BIL. PROGRAM KOD PROGRAM SYARAT KELAYAKAN MAKLUMAT PENGAJIAN LALUAN LUAR NEGARA 1. KOLEJ MARA BANTING (KMB) Mendapat sekurang-kurangnya Gred A- Pelajar akan mengikuti Program International Baccalaureate (IB) dalam LAPAN (8) subjek berikut: selama dua (2) tahun di Kolej MARA Banting (KMB) dan pelajar berpeluang menyambung pengajian ke peringkat Ijazah Sarjana Muda 1) Bahasa Melayu; di universiti terpilih dalam bidang / kursus pengajian seperti berikut: 2) Bahasa Inggeris; IB SAINS HAYAT MARA0101_2021 3) Matematik; 1) Pharmacy 4) Matematik Tambahan; 5) Biologi; 6) Fizik; 7) Kimia; 8) Satu (1) subjek lain Mendapat sekurang-kurangnya Gred A- Pelajar akan mengikuti Program International Baccalaureate (IB) dalam TUJUH (7) subjek berikut: selama dua (2) tahun di Kolej MARA Banting (KMB) dan pelajar berpeluang menyambung pengajian ke peringkat Ijazah Sarjana Muda 1) Bahasa Inggeris; di universiti terpilih dalam bidang / kursus pengajian seperti berikut : 2) Matematik Tambahan; 3) Biologi/ Sains Komputer/ Lukisan a) Bidang Sains Kesihatan & Sains Tulen: Kejuruteraan/ Kej. Awam/ Kej. Elektrik/ Kej. 1) Biomedical Science 9) Audiology/ Speech Pathology Mekanikal/ Reka Cipta; 2) Biochemistry 10) Medical Imaging/ Radiology 4) Fizik; 3) Biotechnology 11) Geology/ Geophysics/Geoscience IB SAINS 5) Kimia; 4) Biological Science 12) Sports Medicine Rehabilitation (SAINS KESIHATAN & MARA0102_2021 6) Dua (2) subjek lain 5) Physiology 13) Veterinary Science SAINS KOMPUTER) -
ASEAN Federation of Endocrine Societies
Journal of the JournalASEAN of the Federation of ASEANEndocrine Federation Societies of EndocrineVolume No. 36 Special EditionSocieties | ISSN 2308-118x (Online) Event ID: CPDE25340 20 Points Vol. 32 No. 2 November 2017 | ISSN 0857-1074 | eISSN 2308-118x VIRTUAL 30th July to 1st August 2021 www.memsmac.org The Journal of the ASEAN Federation of Endocrine Societies (JAFES) is an open-access, peer-reviewed, English language, medical and health science journal that is published two times a year by the ASEAN Federation of Endocrine Societies (AFES). Its editorial policies are aligned with the policies of the International Committtee of Medical Journal Editors (www.icmje.org). JAFES welcomes manuscripts on all aspects of endocrinology and metabolism in the form of original articles, reviewU Narticles,RAVELLING case reports, feature articles T HE I NTRICACIES IN E NDOCRINOLOGY (clinical practice guidelines, clinical case seminars, clinical practice guidelines, book reviews, et cetera), editorials, letters to the Editor, brief communications and special announcements. Authors may include members and non-members of the AFES. Authors are required to accomplish, sign and submit scanned copies of the JAFES Author Form consisting of:Messages (1) Authorship Certification, that the manuscript has been read and approved by all authors, and that the requirements for authorship have been met by each Organisingauthor; (2) the Author Declaration & Scientific, that the article Committee represents original material that is not being considered for publication or has not been published or accepted for publication elsewhere; (3) the Statement of Copyright Transfer [accepted manuscripts become the permanent property of the JAFES and are licensed Listwith an ofAttribution Faculty-Share Alike-Non-Commercial Creative Commons License. -

Download Fair Directory
UTP-Sureworks-Directory-V5.pdf 1 13/11/2019 5:02:57 PM C M Y CM MY A CY CMY K 2019_ad_A-Levels_A5_Dec.indd 2 19/11/2019 3:09 PM Inside this fair directory MESSAGE CONTENTS ADVERTISERS in this directory 5 Welcome Message MESSAGE FROM 6-7 Which Pre-U Programme Should DATIN JERCY CHOO You Pursue? ACCA (The Association of Chartered Certified Accountants) 15 A Closer Look at Veterinary Science FROM SUREWORKS 12-13 AIMST University 14 Organiser of the Education & Further Studies Fair, Dec 2019 What is Automotive Engineering? Asia Pacific University 26 16-17 Curtin University 19 Skills to Prepare You for the Falcon Universal 10 20-21 Fourth Industrial Revolution HELP University IFC Kolej Yayasan UEM (KYUEM) 8 Welcome to the Education & Datin Jercy Choo 22-23 What are Green Jobs? Manipal International University CPS Further Studies Fair Series 50! Medic Ed Consultant Sdn Bhd IBC 28-29 Careers in Event Management Methodist College Kuala Lumpur OBC If you are currently searching for the next step to take in your education journey, you are in the Monash University Malaysia 18 right place! Find all the information you need right here at the fair over the weekend. As there are 32-33 Careers in Sports Science MyStudy Education Consulting so many education options available today, it is important to do as much research as possible to Sdn Bhd (Study Abroad) 35 ultimately choose the right course for you. 36-37 Jobs to Expect in 2020 New Era University College 27 Newcastle University The fair features leading universities, colleges, and skills-based institutions in Malaysia and abroad. -

Hands-On Training on Inhaled Devices to Boost Pharmacy Students
Pharmacy Education (2021) 21(1) 390 – 396 https://doi.org/10.46542/pe.2021.211.390396 RESEARCH ARTICLE Hands-on training on inhaled devices to boost pharmacy students’ performance during inhaler counselling Nurdiana Jamil1 , Wan Nur Syafiqa Wan Norhaidi1, Syahiera Farhana Zakaria2 1 Faculty of Pharmacy, University of Cyberjaya, Selangor, Malaysia 2 School of Pharmacy, International Medical University, Kuala Lumpur, Malaysia Keywords Abstract Inhaler technique OSCE Objective: The effective use of inhalers depends on completeness of information from healthcare Pharmacy curriculum providers. As pharmacists acquire foundational skills on inhalers from their undergraduate curriculum, the experience and performance of pharmacy students regarding inhaler counselling Correspondence should be explored. Methods: Pharmacy students who completed their final year of study Nurdiana Jamil answered an online questionnaire on their experience with teaching-learning activities on inhalers. Faculty of Pharmacy Students also underwent an objective structured clinical exam that included Turbuhaler device University of Cyberjaya counselling. Results: 84 students who completed the online questionnaire strongly agreed that Persiaran Bestari the curriculum increased their awareness of different types of inhalers (65.5%) and specific 63000 Cyberjaya techniques for use (64.3%). Students reported being able to counsel on metered-dose inhaler Selangor (98.8%) and dry-powder inhaler (92.8%) techniques. Students performed well (mean=9.4, SD=2.7) Malaysia at Turbuhaler counselling from a full score of 14. Conclusions: The current training on inhaler [email protected] devices was useful for the pharmacy students. Future training should emphasise supplementary advice on inhaler taste and gargling. Introduction Patients are not solely liable for their ability to use inhalers correctly. -

University of Cyberjaya
YEARS OF EXCELLENCE GENERAL INQUIRY University of Cyberjaya (DU053(B)) www.cyberjaya.edu.my Persiaran Bestari, Cyber 11, 63000, Cyberjaya, Selangor, Malaysia facebook.com/unicyberjaya instagram.com/unicyberjaya Tel : +603 8313 7000 twitter.com/unicyberjaya MALAYSIAN RECRUITMENT INTERNATIONAL RECRUITMENT +6011 1112 3344 +6011 1112 3390 [email protected] [email protected] University Registration No: DU053(B) Copyright © 2020, University of Cyberjaya. This prospectus is intended to be a general statement of information. All information is correct at time of printing, but subject to change without prior notice. For more detailed and recent information, please consult the Student Recruitment Department. The University shall not be held liable for any errors or omissions. BK/PROSPECTUS/07042020 cyberjaya.edu.my Contents 1 Vice Chancellor’s Message 2 Our University 3 International Recognitions 4 World Class Campus 6 Student Life 8 University Township 10 Faculties 12 International Culture 13 Scholarships 14 Employable Graduates 15 Research Advantage 16 Research Clusters 17 Library Research Resources Specialised Laboratories & 18 Facilities --------------------------------- Our Programmes 19 Foundation Programmes 23 Medicine 25 Pharmacy 30 Psychology 35 Physiotherapy 36 Biomedical Engineering 37 Medical Assistant 38 Homeopathy 39 Occupational Safety and Health 43 Business Administration 48 Accounting 50 Information Technology 52 Postgraduate Programmes --------------------------------- 54 Entry Requirements 64 Our Location Vice Chancellor’s Message Welcome and thank you for your interest in University of Cyberjaya. Making a career choice or deciding on a place of study can be a very exciting and important decision for a young person and we are here to provide you with all the information you may require. -

University Students' Attitude Towards Amyotrophic Lateral Sclerosis
Journal of Pharmaceutical Research International 32(36): 89-98, 2020; Article no.JPRI.63911 ISSN: 2456-9119 (Past name: British Journal of Pharmaceutical Research, Past ISSN: 2231-2919, NLM ID: 101631759) University Students’ Attitude towards Amyotrophic Lateral Sclerosis Muhammad Shahid Iqbal1*, Salah-Ud-Din Khan2 Eldowaik Mohamed Salah Saad3 and Muhammad Zahid Iqbal4 1Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam bin Abdulaziz University, Al- kharj, 11942, Saudi Arabia. 2Department of Biochemistry, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia. 3Department of Hospital and Clinical Pharmacy, Faculty of Pharmacy, University of Cyberjaya, Cyberjaya, Malaysia. 4Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, AIMST University, 08100, Bedong, Kedah Darul Aman, Malaysia. Authors’ contributions This work was carried out in collaboration among all authors. Authors MSI and MZI designed the study, performed the initial statistical analyses and wrote the protocol. Authors SDK, EMS and MZI wrote the first draft of the manuscript. Authors MSI, EMS and MZI managed refined analyses. Authors SDK and MSI revised the manuscript. All authors read and approved the final manuscript. Article Information DOI: 10.9734/JPRI/2020/v32i3631001 Editor(s): (1) Dr. Giuseppe Murdaca, University of Genoa, Italy. (2) Dr. Rafik Karaman, Al-Quds University, Palestine. Reviewers: (1) Marcos Vinicio Chein Feres, Universidade Federal de Juiz de Fora, Brasil. (2) H. K. Shreedhar, India. Complete Peer review History: http://www.sdiarticle4.com/review-history/63911 Received 14 August 2020 Original Research Article Accepted 25 December 2020 Published 26 December 2020 ABSTRACT Objective: The objective of the study was to evaluate the attitude of university students towards Amyotrophic Lateral Sclerosis (ALS) in a medical university. -
Conference Programme & Book of Abstracts
4TH INTERNATIONAL CONFERENCE ON MEDICAL EDUCATION INFORMATICS MEI 2021 | 12-15 July | Nottingham| UK Conference Programme & Book of Abstracts Editors Stathis Th. Konstantinidis, Heather Wharrad, NG Chirk Jenn 4th International Conference on Medical Education Informatics 2 4th International Conference on Medical Education Informatics M E I 2 0 21| 12- 15 JULY | NOTTINGHAM | UK Conference Programme & Book of Abstracts of 4th International Conference on Medical Education Informatics July 12-15, 2021 University of Nottingham, Nottingham, UK Editors: Stathis Th. Konstantinidis, Heather Wharrad, NG Chirk Jenn Technical Assistance: Matthew Pears, Daniyar Sapargaliyev Publisher: University of Nottingham ISBN: [will be added in the final version] 4th International Conference on Medical Education Informatics Cover Message We welcome you to Nottingham and the 4th International Conference on Medical Education Informatics – MEI 2021. 4 4th International Conference on Medical Education Informatics Organising Committee Stathis Th. Konstantinidis, University of Nottingham, UK Heather Wharrad, University of Nottingham, UK NG Chirk Jenn, University of Malaya, MY Matthew Pears, University of Nottingham, UK Chin Hai Teo, University of Malaya, MY Hooi Min Lim, University of Malaya, MY International Steering Committee Chair: Panagiotis Bamidis, Aristotle University of Thessaloniki, GR & Leeds Institute of Medical Education, UK Daniela Giordano, Universita degli studi di Catania, IT Stathis Th. Konstantinidis, University of Nottingham, UK Costas Pattichis, -

Garis Panduan Permohonan Application Guideline
APPLICATION GUIDELINE/REQUIREMENT GARIS PANDUAN PERMOHONAN TERTIARY EDUCATION SPONSORSHIP PROGRAMME (TESP 2020) Open to all full-time student who are currently pursuing First Degree Programme at selected field and selected Local Higher Learning Institution. APPLICATIONS REQUIREMENTS • Application must be made online thru MARA Portal via: www.mara.gov.my starting 13th April 2020 (Monday) 10.00am until 4th May 2020 (Monday) 12.00pm. • Applicant must meet the general requirements and academic requirements. • If false information given by the applicant, MARA reserves the right to terminate or withdraw the loan offer. GENERAL REQUIREMENTS • Malaysian. • Applicant and either one parents is Bumipuera. • Meet the family Sosio Economy Status (SES) eligibility requirements set by MARA. • Parents total taxable income is not more than RM180,000 a year. If parents are self- employed or work at oversea, their average gross income must be less than RM 15,000 per month • Parents/Guardians and applicant are not blacklisted by MARA. • Applicant do not receive any financial support/sponsorship from any agency for current study programme (double sponsor). • Sponsorship is not given to applicant taking same programme level. • Free from any chronic/ contagious disease/ disease that require follow-up treatment. • Applicant age limit should not exceed 40 years old at the time of application. ACADEMIC REQUIREMENTS New Student • Obtain CGPA > 3.0 in Asasi/ Matriculation/ Persediaan/ STPM and equivalent. Existing Student • Obtain CGPA > 3.0 in previous semester; AND • Their balance study is not less than a year. Others • Pass SPM with credit Bahasa Melayu. • Academic requirement for medicine, dentistry and pharmacy programme must be meet the criteria set by professional board. -

Dr Yong Rafidah Abdul Rahman
RESUME Dr Yong Rafidah Abdul Rahman MBBS (Malaya), MAFP (M’sia) FRACGP (Australia), FAFP (M’sia) Fellow of Higher Education Academy (UK) PG Diploma Reproductive Medicine (UPM) PG Diploma Medical Education (Dundee) ISO 9001 QMS Lead Auditor May 2018 Summary Dr Yong Rafidah bt Abdul Rahman Current position: Professor (Family Medicine) and Deputy Vice Chancellor (Student Experience & Learning Support) Asia Metropolitan University Professor Dr Hjh Yong Rafidah Abdul Rahman, MBBS(Malaya), FAFP(M’sia), FRACGP(Australia), FHEA(UK), PG Dip. Reproductive Medicine(UPM), PG Dip.Med. Education(Dundee); is a family medicine specialist, medical teacher and medical educationist with passion in quality assurance in higher education. She worked in active clinical medicine for fourteen years before embarking on academic career and has served three universities, before joining the Asia Metropolitan University in March 2017, as the Deputy Vice Chancellor (Academic). She was re-designated as the Deputy Vice Chancellor for Student Experience and Learning Support from April 2018. Having been in various leadership positions in academic and various training programs, she has extensive experience in curriculum development, academic management, quality assurance in higher education as well as student development. Her past administrative appointments include being the Director, Quality Management and Enhancement Centre of Cyberjaya University College of Medical Sciences (CUCMS), where she has overseen the quality management system of the university (including ISO 9001 certification), university enhancement initiatives, accreditation of academic programs and related training for university staff. Prior to this appointment, she was the Deputy Dean (Academic / Clinical) for the Faculty of Medicine, CUCMS. Apart from being a qualified ISO 9001 Quality Management System Lead Auditor; she is also an assessor for accreditation of Malaysian medical programs.