Transforming Mental Health Services in Gwent
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1 a Meeting of the Aneurin Bevan University Health Board Quality and Patient Safety Committee Will Be Held on Thursday 5Th Decem
Agenda A meeting of the Aneurin Bevan University Health Board Quality and Patient Safety Committee will be held on Thursday 5th December 2019, commencing at 09:30am in Conference Rooms 1 & 2, Headquarters, St Cadoc’s Hospital, Caerleon AGENDA Preliminary Matters Attachment 09:30 1.1 Welcome and Introductions Verbal Chair 15 mins 1.2 Apologies for Absence Verbal Chair 1.3 Declarations of Interest Verbal Chair 1.4 Draft Minutes of the Committee Attachment Chair held on 16th October 2019 1.5 Action Sheet of the Committee Attachment Chair held on 16th October 2019 Governance 09:45 2.1 Revised Committee Terms of Attachment Chair 10 Reference mins Presentations 09:55 3.1 Patient Safety - Themes and Presentation Claire Bevan/ 30 Trends to Inform Improvements Dr Brendan Lloyd/ mins and Learning with WAST Darren Panniers, WAST 3.2 Safety and Patient Experience – Presentation Martine Price 20 Winter Plan mins 3.3 Quality & Safety in Presentation Chris Blyth/Jayne 30 Ophthalmology Roberts/Julie Poole mins Break (10 mins) 11.15 For Consideration 11.25 4.1 Quality, Safety and Performance Attachment Dr Paul Buss 15 Overview mins 4.2 Risk Assessment Overview Attachment Chair 10 mins Items for Quality Assurance 11.50 5.1 QPSOG Assurance Update from Verbal Peter Carr 10 Meeting held on 28th November mins 2019 1 Quality & Patient Safety Committee - Thursday 5th December 2019-05/12/19 1 of 259 Agenda 5.2 Clinical Audit Programme Attachment Kate Hooton 10 mins 5.3 Putting Things Right Progress Attachment Rhiannon Jones 10 Against Improvement mins Programme -

Doctors Process of Obtaining a Identification Badge
Identification Badges For Medical & Dental Doctors Please apply for your identification badge as soon as possible. Mail from the identification office can take up to 7 days. How to Apply Email a jpeg image of yourself (with a plain background) Along with your: Full name Email address & Telephone number Start date Hospital base Job title & Speciality GMC/GDC number to: [email protected] * If you have any difficulty in supplying an image to the identification office please email the above address and we will do our best to assist. Important Information It is vital that if your badge becomes lost or stolen that you report it to the identification office immediately via this email address [email protected] You may need to contact the Identification office at the end of each rotation for additional access. Please do this a day or two before your rotation to ensure you do not struggle with gaining access. All Doctors badges have the title “Dr” printed before their first name. If you are entitled and wish to use the alternative titles of Mr, Mrs, Ms, Miss, Prof or other appropriate titles, please highlight this in bold as part of your full name when applying. You will be contacted with a collection point, date & time if you have informed the identification office of your contact details. Please see collection points below. Collect Doctors based Royal Gwent/St Woolos Hospital Collection Point: Security Department, Level 2 B Block Royal Gwent Hospital. Opening hours - 24 hours a day 7 days a week. Doctors based Nevill Hall Hospital -

Job Supporting Document This Will Open in a New Window
Job Description and Information Pack June 2021 DIVISION OF UNSCHEDULED CARE Appointment of Full Time (10 Sessions) Specialty Doctor in Care of the elderly Based at St Woolos, South East Wales http://www.wales.nhs.uk/sitesplus/866/page/40418 Job Reference: 040-SD208 Anticipated Start Date: IMMEDIATE DIVISIONAL CONTACT FOR ENQUIRIES ABOUT THIS POST Dr Ajit Verma, Tel 01633 234387 Links to Additional Information Aneurin Bevan Homepage Aneurin Bevan Values and Behaviours Framework Aneurin Bevan Demography Profile Medical Training/Careers in Wales Visit Wales Train Work Live Medical Resourcing Department, Ground Floor Portacabins, Llanfrechfa Grange, Cwmbran, NP44 8YN Email [email protected] Tel 01633623935 Job Description Title: Specialty Doctor in Care of the Elderly (Replacement Post) Professionally accountable to: Medical Director via Divisional Director Managerially accountable to: Chief Executive via Divisional Director Base: St Woolos Hospital and other sites as per requirements Other hospitals at which duties are performed: In view of the fact that the organisation is currently undertaking a review of its services and the locations at which they are undertaken, it is important to be aware that work patterns may change and the place(s) of duties modified. The Clinical Strategy of the Health Board is under constant development and the job holder may be required to undertake different duties agreed at the time of appointment. Purpose of the Post and General Responsibilities There has never been a more exciting time to join our clinical teams as we pioneer new ways of delivering health services across the Gwent area. Our innovative Clinical Futures programme bridges all aspects of primary, community and secondary care and you could be a part of its plans to deliver the best to our patients and communities. -
Hospitals in Wales Thank You for Your Request Which I Re
Ein cyf/Our ref: ATISN 12891 22 January 2019 Dear , ATISN 12891 – Hospitals in Wales Thank you for your request which I received on 14 January 2019. You asked for the following information: A list of Welsh Hospitals per trust. The information you requested is attached in annex A. If you are dissatisfied with the Welsh Government’s handling of your request, you can ask for an internal review within 40 working days of the date of this response. Requests for an internal review should be addressed to the Welsh Government’s Freedom of Information Officer at: Information Rights Unit, Welsh Government, Cathays Park, Cardiff, CF10 3NQ or Email: [email protected] Please remember to quote the ATISN reference number above. You also have the right to complain to the Information Commissioner. However, please note the Commissioner will not normally investigate a complaint until it has been through our own internal review process. The Information Commissioner can be contacted at: Grŵp Iechyd a Gwasanaethau Cymdeithasol Health and Social Services Group E-bost E-mail: Parc Cathays Cathays Park [email protected] Caerdydd Cardiff CF10 3NQ Rydym yn croesawu derbyn gohebiaeth yn Gymraeg. Byddwn yn ateb gohebiaeth a dderbynnir yn Gymraeg yn Gymraeg ac ni fydd gohebu yn Gymraeg yn arwain at oedi. We welcome receiving correspondence in Welsh. Any correspondence received in Welsh will be answered in Welsh and corresponding in Welsh will not lead to a delay in responding. Information Commissioner’s Office, Wycliffe House, Water Lane, Wilmslow, Cheshire, SK9 5AF The request you sent me contains personal information about you – for example, your name and address. -

Facilities 112 + Bleed Nov 12
2011/12 THE NHS ESTATE IN WALES Facilities Performance Report THE NHS ESTATE IN WALES Facilities Performance Report 2011/12 CONTENTS 1 INTRODUCTION 5 2 EXECUTIVE SUMMARY 6-8 2.1 Context of the report 2.2 Facilities performance 3 THE 2011/12 FACILITIES PERFORMANCE REPORT 9-10 3.1 Health Board/Trust-wide services 3.2 Hospital-specific information 3.3 General observations on data returns 4 ANALYSIS OF HEALTH BOARD/TRUST-WIDE SERVICES DATA 11-23 4.1 Expenditure on NHS facilities services 4.2 Telecommunications 4.3 Car parking 4.4 Cleaning services 4.5 Catering services 4.6 Laundry and linen services 4.7 Security services 4.8 Portering services 4.9 Postal services 5 ANALYSIS OF MAJOR ACUTE HOSPITAL DATA 24-31 5.1 Overall analysis 5.2 Car parking 5.3 Cleaning services 5.4 Catering services 5.5 Laundry and linen services 5.6 Security services 5.7 Portering services 6 APPENDICES 33-109 Appendices I – VIII Observations on FM-related operating costs for each Health Board/Trust 1 INTRODUCTION 1.1 The 2011/12 Facilities Performance Report is based on annual estate data returns for the 2011/12 financial year, submitted to the on-line Estates and Facilities Performance Management System (EFPMS) by seven Health Boards and Velindre NHS Trust with respect to their healthcare premises. Due to the uniqueness of the Welsh Ambulance Services NHS Trust estate, the system, by and large, does not include FM data relating to this Trust. The system was introduced by the Welsh Government in April 2002 and is managed by NHS Wales Shared Services Partnership - Facilities Services (NWSSP-FS). -

Medicines Management in Acute Hospitals: Update on Progress – Aneurin Bevan University Health Board
Medicines Management in Acute Hospitals: Update on Progress – Aneurin Bevan University Health Board Audit year: 2018 Date issued: December 2019 Document reference: 1594A2019-20 This document has been prepared as part of work performed in accordance with statutory functions. In the event of receiving a request for information to which this document may be relevant, attention is drawn to the Code of Practice issued under section 45 of the Freedom of Information Act 2000. The section 45 code sets out the practice in the handling of requests that is expected of public authorities, including consultation with relevant third parties. In relation to this document, the Auditor General for Wales and the Wales Audit Office are relevant third parties. Any enquiries regarding disclosure or re-use of this document should be sent to the Wales Audit Office at [email protected]. We welcome correspondence and telephone calls in Welsh and English. Corresponding in Welsh will not lead to delay. Rydym yn croesawu gohebiaeth a galwadau ffôn yn Gymraeg a Saesneg. Ni fydd gohebu yn Gymraeg yn arwain at oedi. This work was delivered by Urvisha Perez. Contents The Health Board has made good progress in addressing our recommendations to improve aspects of medicines management within acute hospitals, but some high-risk recommendations remain outstanding. Summary report Introduction 4 Our findings 4 Appendices Appendix 1 – progress against our 2015 recommendations 7 Page 3 of 24 - Medicines Management in Acute Hospitals: Update on Progress – Aneurin Bevan University Health Board Summary report Introduction 1 Our 2015 report on Medicines Management in Acute Hospitals found that despite low staffing levels and high workload, there were good relationships with ward staff together with effective aspects of corporate arrangements and some medicines management processes. -

A Cardiff Capital Region Metro: Impact Study
Report to the Minister for Economy, Science and Transport Merthyr Ebbw Hirwaun Tydfil Rhymney Tredegar Vale Brynmawr Abergavenny Aberdare Treherbert Abertillery Pontypool Bargoed Blackwood Newbridge Abercynon Cwmbran Pontypridd Ystrad Mynach Cross Keys Porth Maesteg Talbot Green Taffs Well Caerphilly Caerleon Pontyclun Cardiff Gate North West Heath Bridgend Cardiff Severn Queen Tunnel Ely Mill Street Newport Junction Porthcawl St Llanwern Chepstow Mellons Culverhouse Cross Pill Cardiff Cardiff Bay Bristol Airport Sports Village Cardiff Central Barry Penarth Porth Teigr A Cardiff Capital Region Metro: Impact Study October 2013 Merthyr Ebbw Hirwaun Tydfil Rhymney Tredegar Vale Brynmawr Abergavenny Aberdare Treherbert Abertillery Pontypool Bargoed Blackwood Newbridge Abercynon Cwmbran Pontypridd Ystrad Mynach Cross Keys Porth Maesteg Talbot Green Taffs Well Caerphilly Caerleon Pontyclun Cardiff Gate North West Heath Bridgend Cardiff Severn Queen Tunnel Ely Mill Street Newport Junction Porthcawl St Llanwern Chepstow Mellons Culverhouse Cross Pill Cardiff Cardiff Bay Bristol Airport Sports Village Cardiff Central Barry Penarth Porth Teigr A Cardiff Capital Region Metro... “Connecting more people to more places” “Enabling development and regeneration” “Creating a more liveable and economically dynamic region” A Cardiff Capital Region Metro: Impact Study A Cardiff Capital Region Metro: Foreword Wales is changing; we are at last showing the confidence to embrace the biggest opportunities. Three years ago no-one really expected the valley lines to be electrified, let alone contemplation of a Metro in South East Wales. This is now a real prospect and I was delighted that the Minister for Economy, Science and Transport, Edwina Hart, asked me to lead this Metro study to help frame the development of what will be the most important project in Wales for a generation. -

Your NHS Services in Gwent Have Changed
Your NHS services in Gwent have changed Please read this booklet to find out how you can access services. Cut out and keep NHS SERVICES IN GWENT HAVE CHANGED now The Grange University Hospital is open CALL 999 OR GO TO THE GRANGE UNIVERSITY HOSPITAL A&E if you have a LIFE-THREATENING ILLNESS or SERIOUS INJURY GO TO A MINOR INJURY UNIT at Nevill Hall, the Royal Gwent, Ysbyty Ystrad Fawr or Ysbyty Aneurin Bevan Hospitals, if you have a minor injury (Children under 1 year will need to go to The Grange University Hospital). CALL NHS 111 if you are unwell, unsure what to do and need help. You can also call 111 for urgent GP care when your own Surgery is closed. CONTACT YOUR GP if you have an illness or concern that is not immediately life-threatening. TREAT AT HOME or CONTACT YOUR PHARMACIST if you have a minor illness or ailment such as a sore throat, cough, skin irritation or common mild illness. For more information, visit abuhb.nhs.wales. Keep up to date and ask us questions by following us: @AneurinBevanUHB AneurinBevanHealthBoard Changes to Emergency Hospital Services The Grange University Hospital opened on 17th November 2020 to provide Critical and Specialist Care to every resident living in Gwent and South Powys. The new hospital provides a centre of excellence to treat our most seriously ill patients, or those with significant injuries, and is now the only Emergency Department for the communities of Gwent. The hospital opened ahead of schedule in November 2020 to help us respond to winter pressures and the COVID-19 pandemic. -
Trust Name Hospital Name
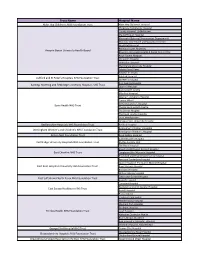
Trust Name Hospital Name Alder Hey Children's NHS Foundation Trust Alder Hey Children's Hospital Chepstow Community Hospital County Hospital, Griffithstown Maindiff Court Hospital Mamhalid (External Procurement Department) Monnow Vale Health and Social Care Centre Nevill Hall Hospital Redwood Suite, Rhymney Aneurin Bevan University Health Board Rhymney Integrated Health & Social Care Centre Royal Gwent Hospital St Cadoc's Hospital St Woolos Hospital The Grange University Hospital Ysbyty Ystrad Fawr Ysbyty'r tri Chwm Ashford Hospital Ashford and St Peter's Hospitals NHS Foundation Trust St Peter's Hospital King George Hospital Barking, Havering and Redbridge University Hospitals NHS Trust Queen's Hospital Barking Birth Centre Mile End Hospital Newham University Hospital Canary Wharf St Bartholomew's Hospital Barts Health NHS Trust The Barkantine Birth Centre The Dental Hospital The Royal London Hospital Trust Headquarters Whipps Cross University Hospital Bedfordshire Hospitals NHS Foundation Trust Bedford Hospital Birmingham Children's Hospital Birmingham Women's and Children's NHS Foundation Trust Birmingham Women's Hospital Bolton NHS Foundation Trust Royal Bolton Hospital Addenbrooke's Hospital Cambridge University Hospitals NHS Foundation Trust Ely Day Surgery Unit The Rosie Hospital Macclesfield District General Hospital East Cheshire NHS Trust Congleton War Memorial Hospital Knutsford and District Community Hospital Kent and Canterbury Hospital Queen Elizabeth The Queen Mother Hospital East Kent Hospitals University NHS Foundation -

Job Description and Information Pack Month 2011
Job Description and Information Pack Month 2011 Job Description and Information Pack January 2021 DIVISION OF Family and Therapies Appointment of Full Time International Training Fellow in Neonatology Based at the Grange University Hospital, South East Wales http://www.wales.nhs.uk/sitesplus/866/page/40418 Job Reference: 040-MTI-Neonates-2021 Anticipated Start Date: Required for an immediate start for a period of 24 months DIVISIONAL CONTACT FOR ENQUIRIES ABOUT THIS POST Dr Sue Papworth, Consultant Neonatologist and Clinical Director Tel 01633-234615 Dr Gautam Bagga, Consultant Neonatologist, Tel 01633-234615 Dr Tanoj Kollamparambil, Consultant Neonatologist, Tel 01633-234615 Links to Additional Information Aneurin Bevan Homepage Aneurin Bevan Values and Behaviours Framework Aneurin Bevan Demography Profile Medical Training/Careers in Wales Visit Wales Train Work Live Medical Resourcing Department, Ground Floor Portacabins, Llanfrechfa Grange, Cwmbran, NP44 8YN Email [email protected] Tel 01633623935 JOB DESCRIPTION The Job Itself Title: International Training Fellow in Neonatology (MTI) Professionally accountable to: Medical Director via Clinical and Divisional Directors Managerially accountable to: Supervising Consultant Base: Grange University Hospital, Cwmbran, South East Wales Other hospitals at which duties are performed: In view of the fact that the organisation is currently undertaking a review of its services and the locations at which they are undertaken, it is important to be aware that work patterns may -

Aneurin Bevan University Health Board Job Blurb the Area Gwent Is Between Newport in the South, Abergavenny in the North, Rhymn
Aneurin Bevan University Health Board Job blurb The Area Gwent is between Newport in the south, Abergavenny in the north, Rhymney in the west and Monmouth in the East. There is easy access to the Brecon Beacons if you enjoy the outdoors, and Cardiff if city life is more up your street. There is no need to speak Welsh! The toll for the Severn Bridge will be abolished in December 2018 making it possible to commute to Bristol. This post is a replacement for a current CSRH trainee expected to complete in September or October 2018. There is another senior trainee in Cardiff and Vale the neighbouring health board. There are established links with Gynaecology, Public Health, Forensic medicine, so that the vast majority of training can be acquired in Gwent or Cardiff. The first 18 months are based in Royal Gwent or Ysbyty Ystrad Fawr hospitals with Mrs Makiya Ashraf the supervisor. She is an experienced College Tutor. Dr Louise Massey is the Training Programme Director and Education Supervisor. There are many other trainers in the department. 1.1 Names of Senior and Consultant Members of the Department Clare Lipetz, Clinical Director, consultant in Sexual & Reproductive Health Humphrey Birley, Consultant GUM/HIV Charlotte Fleming, Consultant in Sexual and Reproductive health Carys Knapper, Consultant GUM/HIV Louise Massey, Consultant in Sexual and Reproductive health Hayley Easen/Janine Jones, Senior Nurse, Sexual and Reproductive Health 1.2 Other relevant Staff (e.g. Scientific, Technical, Nursing) 8 part time SAS doctors 1 part time subspecialty trainee 40 part time nurses 6 outreach workers 20 administration, secretarial & clerical support Biomedical science support 2. -

Aneurin Bevan University Health Board – Housing and Mental Health Support Analysis April 2019
Aneurin Bevan University Health Board – Housing and Mental Health Support Analysis Final Report April 2019 Housing and Mental Health Mapping Analysis Contents 1. Introduction 3 2. Context 3 3. Executive summary 5 4. Methodology 7 5. Current services, good practice and innovation in Gwent – the base line 8 6. Findings – key issues for stakeholders 29 7. Examples of good practice and innovation in housing and mental health – national 58 8. Recommendations for a strategic programme 65 Appendix 1 – Project Steering Group membership 69 Appendix 2 – Stakeholders and contributors to the research 70 Appendix 3 – Documents reviewed 73 Appendix 4 – Service mapping 75 Appendix 5: Horizon Scan of innovative and good practice services 88 Aneurin Bevan University Health Board April 2019 2 of 111 Housing and Mental Health Mapping Analysis 1. INTRODUCTION 1.1 This housing and mental health support analysis was commissioned by the Aneurin Bevan University Health Board (ABUHB) in January 2019. The Board and its partners in Housing, Public Health, Supporting People formed a steering group (membership listed as Appendix 1) to oversee the project, meeting fortnightly with Campbell Tickell throughout the project’s duration. 1.2 The analysis has set out to provide a baseline assessment of Housing and Housing Related Support Services for adults with mental health issues, aged 18+ across the Gwent area (Blaenau Gwent, Caerphilly, Monmouthshire, Newport and Torfaen). The key objectives of this study are: 1) To identify the key issues for all stakeholders and describe possible solutions; 2) To map all current housing related mental health support available within health, social care, housing (statutory, registered social landlords and Supporting People) and the third sector; 3) To identify examples of good practice and innovation locally and across the UK that could inform possible solutions; 4) To organise and facilitate an event with key stakeholders to develop a strategic programme of work to take forward the findings of this study.