Omnibus Codes (For Nebraska Only)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Geomorphic and Hydraulic Assessment of the Bear River in and Near Evanston, Wyoming
GEOMORPHIC AND HYDRAULIC ASSESSMENT OF THE BEAR RIVER IN AND NEAR EVANSTON, WYOMING By M.E. SMITH anc/M.L. MADERAK____________________ U.S. GEOLOGICAL SURVEY Water-Resources Investigations Report 93-4032 Prepared in cooperation with the CITY OF EVANSTON and UINTA COUNTY Cheyenne, Wyoming 1993 U.S. DEPARTMENT OF THE INTERIOR BRUCE BABBITT, Secretary U.S. GEOLOGICAL SURVEY ROBERT M. HIRSCH, Acting Director For additional information Copies of this report may be write to: purchased from: U.S. Geological Survey Earth Science Information Center District Chief Open-File Reports Section U.S. Geological Survey Box 25286, MS 517 2617 E. Lincolnway, Suite B Denver Federal Center Cheyenne, Wyoming 82001 Denver, Colorado 80225 CONTENTS Abstract..................................................................................................................................................................... 1 Introduction................................................................................._^ 2 Purpose and scope....................................................................................................................................... 2 Acknowledgments...................................................................................................................................... 2 Approach................................................................................................................................................................... 4 Methods of analysis................................................................................................................................... -
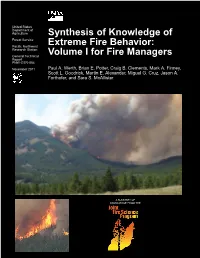
Synthesis of Knowledge of Extreme Fire Behavior: Volume I for Fire Managers
United States Department of Agriculture Synthesis of Knowledge of Forest Service Pacific Northwest Extreme Fire Behavior: Research Station General Technical Volume I for Fire Managers Report PNW-GTR-854 November 2011 Paul A. Werth, Brian E. Potter, Craig B. Clements, Mark A. Finney, Scott L. Goodrick, Martin E. Alexander, Miguel G. Cruz, Jason A. Forthofer, and Sara S. McAllister A SUMMARY OF KNOWLEDGE FROM THE The Forest Service of the U.S. Department of Agriculture is dedicated to the principle of multiple use management of the Nation’s forest resources for sustained yields of wood, water, forage, wildlife, and recreation. Through forestry research, cooperation with the States and private forest owners, and management of the national forests and national grasslands, it strives—as directed by Congress—to provide increasingly greater service to a growing Nation. The U.S. Department of Agriculture (USDA) prohibits discrimination in all its programs and activities on the basis of race, color, national origin, age, disability, and where applicable, sex, marital status, familial status, parental status, religion, sexual orientation, genetic information, political beliefs, reprisal, or because all or part of an individual’s income is derived from any public assistance program. (Not all prohibited bases apply to all programs.) Persons with disabilities who require alternative means for communication of program information (Braille, large print, audiotape, etc.) should contact USDA’s TARGET Center at (202) 720-2600 (voice and TDD). To file a complaint of discrimination, write USDA, Director, Office of Civil Rights, Room 1400 Independence Avenue, SW, Washington, DC 20250-9410 or call (800) 795-3272 (voice) or (202) 720-6382 (TDD). -

Morphology, Grain Size Characteristics, and Fluvial Processes of Two Bars, Colville River Delta, Alaska
Louisiana State University LSU Digital Commons LSU Historical Dissertations and Theses Graduate School 1977 Morphology, Grain Size Characteristics, and Fluvial Processes of Two Bars, Colville River Delta, Alaska. Donald Franklin Nemeth Louisiana State University and Agricultural & Mechanical College Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_disstheses Recommended Citation Nemeth, Donald Franklin, "Morphology, Grain Size Characteristics, and Fluvial Processes of Two Bars, Colville River Delta, Alaska." (1977). LSU Historical Dissertations and Theses. 3075. https://digitalcommons.lsu.edu/gradschool_disstheses/3075 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Historical Dissertations and Theses by an authorized administrator of LSU Digital Commons. For more information, please contact [email protected]. INFORMATION TO USERS This material was produced from a microfilm copy of the original document. While the most advanced technological means to photograph and reproduce this document have been used, the quality is heavily dependent upon the quality of the original submitted. The following explanation of techniques is provided to help you understand markings or patterns which may appear on this reproduction. 1. The sign or "target" for pages apparently lacking from the document photographed is "Missing Page(s)". If it was possible to obtain the missing page(s) or section, they are spliced into the film along with adjacent pages. This may have necessitated cutting thru an image and duplicating adjacent pages to insure you complete continuity. 2. When an image on the film is obliterated with a large round black mark, it is an indication that the photographer suspected that the copy may have moved during exposure and thus cause a blurred image. -
Analysis of Runoff from Small Drainage Basins in Wyoming
Analysis of Runoff from Small Drainage Basins in Wyoming GEOLOGICAL SURVEY WATER-SUPPLY PAPER 2056 Prepared In cooperation with the Wyoming Highway Department and the U.S. Department of Transportation, Federal Highway Administration Analysis of Runoff from Small Drainage Basins in Wyoming By GORDON S. CRAIG, JR., and JAMES G. RANKL GEOLOGICAL SURVEY WATER-SUPPLY PAPER 2056 Prepared in cooperation with the Wyoming Highway Department and the U.S. Department of Transportation, Federal Highway Administration UNITED STATES GOVERNMENT PRINTING OFFICE, WASHINGTON : 1978 UNITED STATES DEPARTMENT OF THE INTERIOR CECIL D. ANDRUS, Secretary GEOLOGICAL SURVEY H. William Menard, Director Library of Congress Catalog-card Number 78-600090 For sale by the Superintendent of Documents, U. S. Government Printing OfEce Washington, D. C. 20402 Stock Number 024-001-03106-0 CONTENTS Page Symbols_________________________________________ V Abstract_________________________________________ 1 Introduction ________________________________________ 1 Purpose and scope _______ ____________________________ 1 Limitations of study _______________________________ 5 Acknowledgments ________________________________________ 5 Use of metric units of measurement ________________________ 6 Data collection ____________________________________ 6 Description of area __________________________________ 6 Instrumentation __________________________________ 7 Types of records _________________________________________ 7 Station frequency analysis _________________________________ 9 Runoff -

Geologic and Physiographic Controls on Bed-Material Yield, Transport, and Channel Morphology for Alluvial and Bedrock Rivers, Western Oregon
Geologic and physiographic controls on bed-material yield, transport, and channel morphology for alluvial and bedrock rivers, western Oregon Jim E. O’Connor1,†, Joseph F. Mangano1,2, Scott W. Anderson1,3, J. Rose Wallick1, Krista L. Jones1, and Mackenzie K. Keith1 1U.S. Geological Survey, Oregon Water Science Center, 2130 SW 5th Avenue, Portland, Oregon 97201, USA 2Department of Geosciences, Colorado State University, Fort Collins, Colorado 80523, USA 3Department of Geography, University of Colorado–Boulder, Boulder, Colorado 80309, USA ABSTRACT geometry and sediment supply. At the scale (Stanford and Ward, 1993; Yarnell et al., 2006). of western Oregon, the physiographic and Most fundamentally, the distinction relates to the The rivers of western Oregon have di- lithologic controls on the balance between balance between bed-material supply and river verse forms and characteristics, with channel bed-material supply and transport capacity transport capacity (Gilbert, 1877, 1914; Howard, substrates ranging from continuous alluvial exert far-reaching infl uence on the distribu- 1980; Whipple, 2004). Rivers in which the long- gravel to bare bedrock. Analysis of several tion of alluvial and nonalluvial channels and term channel transport capacity exceeds bed- measurable morphologic attributes of 24 val- their consequently distinctive morphologies material supply (termed supply- or detachment- ley reaches on 17 rivers provides a basis for and behaviors—differences germane for un- limited rivers) will typically fl ow over bedrock comparing nonalluvial and alluvial channels. derstanding river response to tectonics and beds for part or much of their courses. Where Key differences are that alluvial reaches have environmental perturbations, as well as for supply meets or exceeds transport capacity greater bar area, greater migration rates, and implementing effective restoration and moni- (transport-limited rivers), channel beds are typi- show systematic correlation among variables toring strategies. -
2021 Hunting and Trapping Regulations
Effective July through2021 June 30, 2022 Updated 9.10.21 MINNESOTA HUNTING & TRAPPING REGULATIONS SHARE THE PASSION mndnr.gov/hunting #huntmn Paid Advertisement FIREWOOD ALERT! You have the power to protect forests and trees! Pests like the invasive Buy locally harvested firewood at emerald ash borer can or near your destination. hitchhike in your firewood. Buy certified heat-treated firewood You can prevent the spread ahead of time, if available. of these damaging insects and diseases by following Gather firewood on site when these firewood tips: permitted. What might be in your firewood? GYPSY MOTH is a devastati ng pest SPOTTED LANTERNFLY sucks sap from of oaks and other trees. Female dozens of tree and plant species. This pest moths lay tan patches of eggs on loves tree-of-heaven but will feed on black fi rewood, campers, vehicles, pati o walnut, white oak, sycamore, and grape. furniture — anything outside! When Like the gypsy moth, this pest lays clusters these items are moved to new areas, of eggs on just about any dry surface, from this pest gets a free ride. landscaping stone to fi rewood! ASIAN LONGHORNED BEETLE will EMERALD ASH BORER — the infamous tunnel through, and destroy, over killer of ash trees — is found in forests 20 species of trees — especially and city trees across much of the eastern maple trees. The larvae of this and central United States. This insect is beetle bore into tree branches and notoriously good at hitching rides in infested trunks, making it an easy pest to fi rewood. Don’t give this tree-killing bug a accidentally transport in fi rewood. -

PADDLING TRAIL River Thames: Putney to Old Isleworth
PADDLING TRAIL River Thames: Putney to Old Isleworth Key Information Start: Putney Slipway, Putney Portages: 0 For more Embankment, Putney, Time: 2-4 hours information scan SW15 1JW Distance: 8 miles the QR code or Finish: Isleworth Draw Dock, OS Map: Explorer 161 https://bit.ly/2Lyh5 Church St, Old Isleworth, London South k1 TW7 6BG & 173 London North This is a busy and tidal part of the River Thames. You must visit boatingonthethames.co.uk to check tide times and safety advice before undertaking this trail. The trail covers the Upper Tideway in south west London, with sweeping aspects of the river. The course of the annual University Boat Race forms part of the trail. 1. We recommend you paddle with the assistance of the tidal flow, departing from Putney in the first 2 hours of the flood tide. Closely timing the tides can allow a return trip. Put in at the public slipway, crossing to the Football Stadium side of the river and turning left, for correct rules of travel. 2. Approaching Hammersmith Bridge the London Wetland Centre is behind the tree line on the opposite bank. Beware of the tide pushing you into Dove Pier after the b ridge. 3. Between Hammersmith and Chiswick Ait the river is flanked by elegant houses. At Chiswick Ait an option is to take the inside channel; usually passable after an hour or so of a flood tide. 4. Chiswick Pier signals a crossing point for a change in navigation rules. Keep the green marker buoys on your right on this sweeping bend of the river to Chiswick Bridge. -

Application of Remote Sensing and GIS Technology for Monitoring Coastal Changes in Estuary Area of the Red River System, Vietnam
Journal of the Korean Society of Surveying, Geodesy, Photogrammetry and Cartography, Vol. 31, No. 6-2, 529-538, 2013 http://dx.doi.org/10.7848/ksgpc.2013.31.6-2.529 Application of Remote Sensing and GIS technology for monitoring coastal changes in estuary area of the Red river system, Vietnam Pham Thi Lan1) · Tong Si Son2) · Kavinda Gunasekara3) · Nguyen Thi Nhan4)· La Phu Hien5) Abstract Coastline is the most dynamic part of seascape since its shape is affected by various factors. Coastal zone is an area with immense geological, geomorphological and ecological interest. Monitoring coastal change is very important for safe navigation, coastal resource management. This paper shows a result of monitoring coastal morphological changes using Remote Sensing and GIS. Study was carried out to obtain intensity of erosion, deposition and sand bar movement in the Red River Delta. Satellite images of ALOS/AVNIR-2 and Landsat were used for the monitoring of coastal morphological changes over the period of 1975 to 2009. Band rationing and threshold technique was used for the coastline extraction. Tidal levels at the time of image acquisition varied from -0.89m to 2.87m. Therefore, coastline from another image at a different tidal level in the same year was considered to get the corrected coastline by interpolation technique. A series of points were generated along the coastal line from 1975 image and were established as reference points to see the change in later periods. The changes were measured in Euclidean distances from these reference points. Positive values represented deposition to the sea and negative values are erosion. -

Record of Decision Canyon Mine Proposal
DOCUMENT #f, / RECORD OF DECISION USDA Forest Service Kaibab National Forest CANYON MINE PROPOSAL Final Environmental Impact Statement Coconino County, Arizona r - . t __ .. 915 RECORD OF DECISION / J USDA Forest Service Kaibab National Forest CANYON MINE PROPOSAL Final Environmental Impact Statement Coconino County, Arizona I. Introduction This Recor't:l of Decision docl.lllents my approval of a modified Plan of Operations for the Canyon Uranium ~ine on the Kaibab National Forest. The alternatives considered and my rationale for selecting the preferred alternative are described in this Record of Decision. The environmentally preferred alternative is also identified. In October, 1984, Energy Fuels Nuclear, Inc. (EFN), submitted to the USDA Forest Service, Kaibab National Forest, a proposed Plan of Operations to mine uranium on unpatented mining claims on the Tusayan Ranger District. The proposed mine is located in Coconino County, Arizona, approximately six miles south of the community of Tusayan. A detailed description of the proposed mine operations can be found in the Environmental Impact Statement (EIS). In brief, the proposed Canyon Mine would involve underground mining of a breccia pipe uranium deposit and would require disturbance of approximately 17 acres for the mine shaft and surface facilities. Ore from the rrJine ~ will be trucked to t.he licensed mill near Blanding, Utah. When the Plan of Operations was submitted, the Forest Service sought public review and COlTInent on tbe proposal to assist in determining the appropriate levei of analysis and documentation required under the ~ational Environmental Policy Act (NEPA). The Forest Service decided the preparation of an EIS was "'erranted and c notice to prepare an EIS was published in the Federal Register on April 30, 1985. -

Specification of Sediment Maintenance Flows for a Large Gravel-Bed River
WATER RESOURCES RESEARCH, VOL. 32, NO. 9, PAGES 2911-2921, SEPTEMBER 1996 Specification of sediment maintenance flows for a large gravel-bed river Peter R. Wilcock Departmentof Geographyand EnvironmentalEngineering, The JohnsHopkins University, Baltimore, Maryland G. Mathias Kondolf, and W. V. Graham Matthews Center for EnvironmentalDesign Research, University of California,Berkeley Alan F. Barta Intermountain Research Station, U.S. Forest Service, Boise, Idaho Abstract. Reservoirreleases may be specifiedto flushinterstitial fine sedimentfrom gravelbeds in the river downstream.Choice of an effectiveflow dependson trade-offs amongdischarge, flow duration,and pool dredgingas they determinerates of bed mobilization,sand removal, and gravel loss.A basisfor evaluatingthese trade-offs is developedwith an approximatemethod appropriateto the sparsedata typicallyavailable. Sand and graveltransport are representedwith rating curves.Approximate methods are introducedfor estimatingeffective gravel entrainment,subsurface sand supply,and pool sedimenttrapping. These are combinedin a sandrouting algorithmto evaluateflushing alternativesfor the Trinity River, California. A sedimentmaintenance flow of moderate size,just sufficientto entrainthe bed surfaceover the durationof the release,limits gravel lossand maximizessand trapping by pools.Larger dischargesproduce more finesremoval but at the costof greater gravelloss and reducedselective transport of fines.Dredged poolsincrease sand removal efficiency by providingmultiple exitsfrom the channeland minimizegravel -

The Chi-Mun River Basin: Introducing the Study Area
Water Traps: The Elusive Quest for Water Storage in the Chi- Mun River Basin, Thailand Philippe Floch, François Molle WORKING PAPER Mekong Program on Water, Environment and Resilience For quotation: Floch P. and Molle F. (2009). Water Traps: The Elusive Quest for Water Storage in the Chi-Mun Basin, Thailand. Working Paper. Mekong Program on Water, Environment and Resilience (M- POWER). University of Natural Resources and Applied Life Sciences, Institut de Recherche pour le Développement, Chiang Mai, Thailand. Acknowledgement: This research was supported by Mekong Program on Water, Environment and Resilience (MPOWER), as part of its contribution to the CGIAR Challenge Programme on Water and Food ii Table of Content Table of Content .................................................................................................................................................................iii Figures.....................................................................................................................................................................................iv Tables.......................................................................................................................................................................................iv Abstract.....................................................................................................................................................................................v INTRODUCTION.................................................................................................................................... -

Selective Transport and Armoured Layer Development in NonUniform Bed Materials Part 1: Numerical Model Development
SELECTIVE TRANSPORT AND ARMOURED LAYER DEVELOPMENT IN NONUNIFORM BED MATERIALS PART 1: NUMERICAL MODEL DEVELOPMENT Arie Setiadi Moerwanto Pusat Penelitian dan Pengembangan Sumber Daya Air Jl. H. Juanda no. 193, Bandung E‐Mail: [email protected] Diterima: 30 Maret 2011; Disetujui: 10 Agustus 2011 ABSTRAK Pada sungai dengan material dasar sungai tidak seragam, ukuran butir, rapat massa dan keberadaan butir butir material terhadap aliran sungai akan sangat mempengaruhi gerak mula masingmasing butir material dasar sungai. Aliran sungai akan terlebih dahulu mengangkut material dasar sungai dengan ukuran butir yang relatif kecil dan tidak terlindungi, sementara butirbutir dengan ukuran yang lebih besar dan stabil akan membentuk lapisan perisai di permukaan dasar sungai. Karena angkutan sedimen terpilah, pembentukan lapisan perisai dan pembentukan corak dasar sungai sangat terkait erat dengan laju angkutan sedimen, maka kecermatan penyimulasian fenomenafenomena tersebut akan sangat mempengaruhi ketelitian analisis kedalaman aliran, laju muatan sedimen dasar, laju angkutan sedimen layang dan pada akhirnya juga akan mempengaruhi kecermatan analisis perubahan morfologi sungai. Dalam tulisan bagian pertama ini dibahas dengan detail studi pustaka dan landasan teori untuk pengembangan model numerik angkutan material sedimen terpilah, prediksi ketebalan lapisan aktif, mekanisme pertukaran antara material dasar sungai, angkutan sedimen dasar dan angkutan sedimen layang, pembentukan corak dasar sungai dan pembentukan lapisan perisai pada sungai dengan material dasar sungai tidak seragam. Verifikasi dan penilaian unjuk kerja model numerik yang didesain diulas dalam tulisan bagian kedua. Kata Kunci: Material tidak seragam dasar sungai, angkutan sedimen terpilah, corak dasar sungai, lapisan perisai, morfologi sungai. ABSTRACT For rivers with nonuniform bed materials, particle size, shape, density and exposure to the flow determine the resistance to movement of an individual particle.