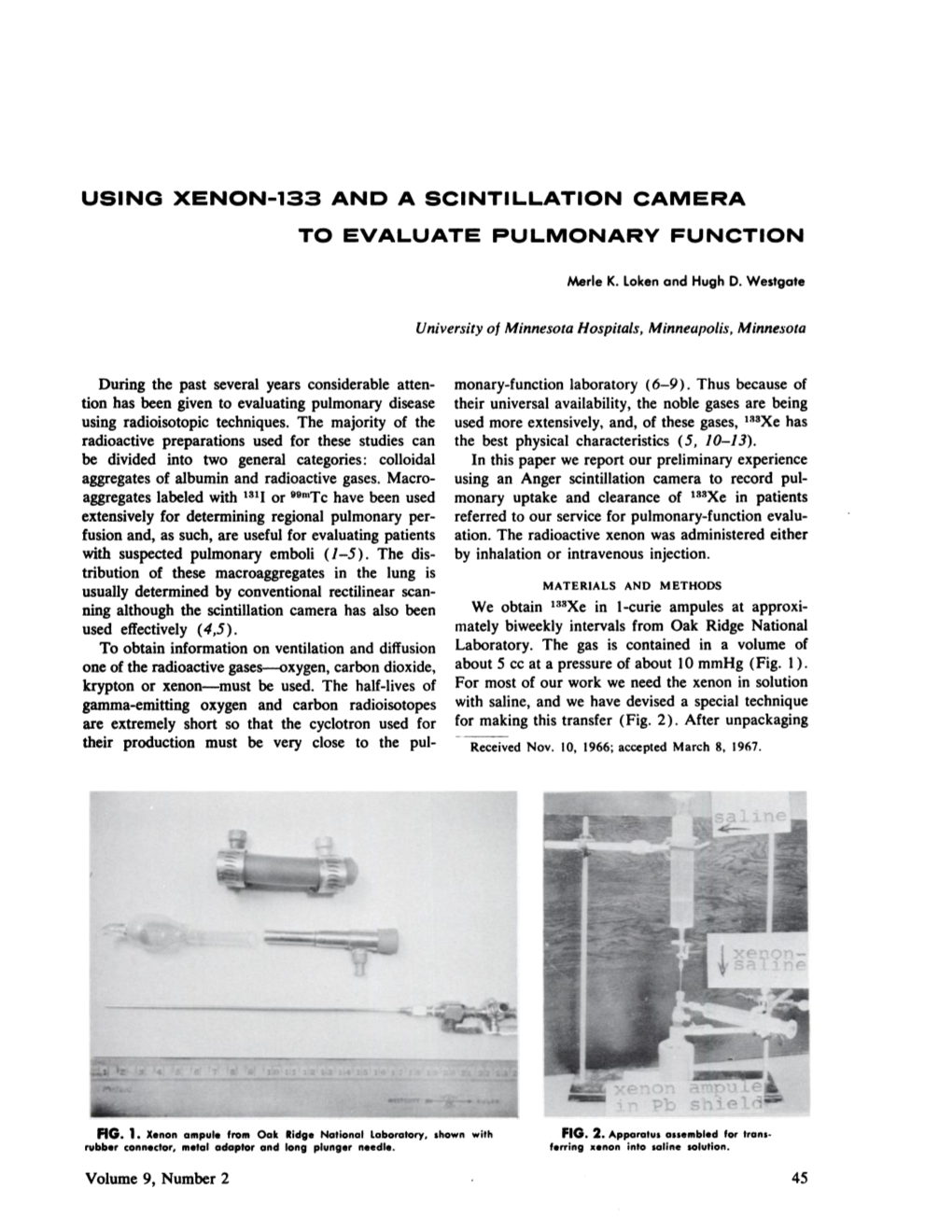
Using Xenon-133 and a Scintillation Camera to Evaluate Pulmonary Function
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Unique Properties of Water!
Name: _______ANSWER KEY_______________ Class: _____ Date: _______________ Unique Properties of Water! Word Bank: Adhesion Evaporation Polar Surface tension Cohesion Freezing Positive Universal solvent Condensation Melting Sublimation Dissolve Negative 1. The electrons are not shared equally between the hydrogen and oxygen atoms of water creating a Polar molecule. 2. The polarity of water allows it to dissolve most substances. Because of this it is referred to as the universal solvent 3. Water molecules stick to other water molecules. This property is called cohesion. 4. Hydrogen bonds form between adjacent water molecules because the positive charged hydrogen end of one water molecule attracts the negative charged oxygen end of another water molecule. 5. Water molecules stick to other materials due to its polar nature. This property is called adhesion. 6. Hydrogen bonds hold water molecules closely together which causes water to have high surface tension. This is why water tends to clump together to form drops rather than spread out into a thin film. 7. Condensation is when water changes from a gas to a liquid. 8. Sublimation is when water changes from a solid directly to a gas. 9. Freezing is when water changes from a liquid to a solid. 10. Melting is when water changes from a solid to a liquid. 11. Evaporation is when water changes from a liquid to a gas. 12. Why does ice float? Water expands as it freezes, so it is LESS DENSE AS A SOLID. 13. What property refers to water molecules resembling magnets? How are these alike? Polar bonds create positive and negative ends of the molecule. -

Periodic Table of the Elements Notes
Periodic Table of the Elements Notes Arrangement of the known elements based on atomic number and chemical and physical properties. Divided into three basic categories: Metals (left side of the table) Nonmetals (right side of the table) Metalloids (touching the zig zag line) Basic Organization by: Atomic structure Atomic number Chemical and Physical Properties Uses of the Periodic Table Useful in predicting: chemical behavior of the elements trends properties of the elements Atomic Structure Review: Atoms are made of protons, electrons, and neutrons. Elements are atoms of only one type. Elements are identified by the atomic number (# of protons in nucleus). Energy Levels Review: Electrons are arranged in a region around the nucleus called an electron cloud. Energy levels are located within the cloud. At least 1 energy level and as many as 7 energy levels exist in atoms Energy Levels & Valence Electrons Energy levels hold a specific amount of electrons: 1st level = up to 2 2nd level = up to 8 3rd level = up to 8 (first 18 elements only) The electrons in the outermost level are called valence electrons. Determine reactivity - how elements will react with others to form compounds Outermost level does not usually fill completely with electrons Using the Table to Identify Valence Electrons Elements are grouped into vertical columns because they have similar properties. These are called groups or families. Groups are numbered 1-18. Group numbers can help you determine the number of valence electrons: Group 1 has 1 valence electron. Group 2 has 2 valence electrons. Groups 3–12 are transition metals and have 1 or 2 valence electrons. -

The Oxygen and Carbon Dioxide Compensation Points of C3
Proc. Natl. Acad. Sci. USA Vol. 92, pp. 11230-11233, November 1995 Plant Biology The oxygen and carbon dioxide compensation points of C3 plants: Possible role in regulating atmospheric oxygen (photosynthetic carbon/02 inhibition/photorespiration/Nicotiana tobacum/Spinacea oleracea) N. E. TOLBERT*, C. BENKERt, AND E. BECKt *Department of Biochemistry, Michigan State University, East Lansing, MI 48824; and tLehrstuhl Fur Pflanzenphysiologie, Universitat Bayreuth, 95440 Bayreuth, Germany Contributed by N. E. Tolbert, August 15, 1995 ABSTRACT The 02 and CO2 compensation points (02 F bisphosphate to sustain the C2 cycle. Refixation of CO2 and C02 F) of plants in a closed system depend on the ratio of generates the same amount of 02 as taken up during the C2 CO2 and 02 concentrations in air and in the chloroplast and cycle. There is no net CO2 and 02 gas exchange during the specificities of ribulose bisphosphate carboxylase/oxyge- photorespiration (11) unless the complete C2 cycle is blocked nase (Rubisco). The photosynthetic 02 F is defined as the or metabolically interrupted by accumulation or removal of atmospheric 02 level, with a given CO2 level and temperature, products such as glycine or serine. Photorespiration dissipates at which net 02 exchange is zero. In experiments with C3 excess photosynthetic capacity (ATP and NADPH) without plants, the 02 F with 220 ppm CO2 is 23% 02; 02 F increases CO2 reduction or net 02 change. Photosynthetic carbon me- to 27% with 350 ppm CO2 and to 35% 02 with 700 ppm CO2. tabolism is a competition between CO2 and 02 for the dual At 02 levels below the 02 F, C02 uptake and reduction are activities of Rubisco, based on the ratio of CO2 and 02 accompanied by net 02 evolution. -

Liquid Densities of Oxygen, Nitrogen, Argon and Parahydrogen 6
NATL INST OF STAND & TECH A111D7 231A72 NBS TECHNICAL NOTE 361(Revised) *+ •«, - *EAU O* Metric Supplement May 1974 U.S. DEPARTMENT OF COMMERCE /National Bureau of Standards Liquid Densities of Oxygen, Nitrogen, Argon and Parahydrogen NATIONAL BUREAU OF STANDARDS The National Bureau of Standards ' was established by an act of Congress March 3, 1901. The Bureau's overall goal is to strengthen and advance the Nation's science and technology and facilitate their effective application for public benefit. To this end, the Bureau conducts research and provides: (1) a basis for the Nation's physical measurement system, (2) scientific and technological services for industry and government, (3) a technical basis for equity in trade, and (4) technical services to promote public safety. The Bureau consists of the Institute for Basic Standards, the Institute for Materials Research, the Institute for Applied Technology, the Institute for Computer Sciences and Technology, and the Office for Information Programs. THE INSTITUTE FOR BASIC STANDARDS provides the central basis within the United States of a complete and consistent system of physical measurement; coordinates that system with measurement systems of other nations; and furnishes essential services leading to accurate and uniform physical measurements throughout the Nation's scientific community, industry, and commerce. The Institute consists of a Center for Radiation Research, an Office of Meas- urement Services and the following divisions: Applied Mathematics — Electricity — Mechanics — Heat -

Coordination Chemistry of Xenon
Coordination Chemistry of Xenon Paul Griffin Literature Seminar 11/14/19 Situated on the far side of the periodic table, the chemical inertness of the noble gases has led to their widespread applications ranging from gas-discharge lamps and ion engines for space travel to medical applications including as MRI contrast agents and radiotherapy.1 Though all practical applications of the noble gases center around Xe (0), understanding the reactivity and bonding of xenon in higher oxidation states is fundamental to investigating chemistry at the far end of the periodic table. The reactivity of the noble gases, in particular xenon, was first uncovered when Bartlett, who had previously prepared dioxygenyl hexafluoroplatinate (V) (O2PtF6), noted similar ionization energies for molecular oxygen and atomic xenon (a difference of 0.1 eV).2 Mixing of xenon with PtF6 vapor led to the formation of an orange-yellow solid led to the synthesis of the first noble gas compound, xenon hexafluoroplatinate (V) (XePtF6). The chemistry of xenon has evolved significantly since its’ discovery to include an assortment of xenon fluorides, oxides, oxylfluorides, organoxenon3, and metalloxenon compounds such as the tetraxenoaurate (II) cation (Figure 1).4 These species have weak covalent bonding between Xe and the oxygen/fluorine moieties.5 The chemistry of xenon is dominated by the 2+, 4+, and 6+ oxidation states, though Xe (VIII) compounds are known in the form of perxenates and xenon tetroxide. These primarily ionic species, particularly the oxides, oxylfluorides, and fluorides, serve as precursors to noncovalent adducts of xenon. Figure 1. Organoxenon and metalloxenon species Recent work has led to the preparation of xenon adducts with noncovalently interacting ligands such as acetonitrile6a, 6b, ketones6c, sulfoxides6c, and crown ethers6d (Figure 2) capable of weakly coordinating to xenon salts to afford stable species at room temperature. -
HOME OXYGEN FIRE SAFETY a Fact Sheet for Home Oxygen Users
New York State Office of Fire Prevention and Control HOME OXYGEN FIRE SAFETY A Fact Sheet for Home Oxygen Users This bulletin provides general safety information for oxygen equipment used for medical purposes in private homes, apartments and condominiums. Oxygen Liquid oxygen @Do not use liquid oxygen vessels that exceed 10 gallons. Oxygen is not flammable, but it can Oxygen is stored as a very cold cause other materials that burn to liquid in a vessel very similar to a Safety thermos. When released, the liquid ignite more easily and to burn far @Never smoke while using oxygen. more rapidly. The result is that a converts to a gas and you breathe it fire involving oxygen can appear in just like compressed gas. This @Warn visitors not to smoke near storage method takes up less space you when you are using oxygen. explosive-like. Oxygen is of great benefit to those in need of than the compressed gas cylinder, @Post at least one NO SMOKING respiratory therapy but it should and you can transfer the liquid to a sign in a prominent place at the always be handled with caution and small, portable vessel at home. entrance to your home. Liquid oxygen is more expensive awareness of the potential hazards. @ than the compressed gas and the When you go to a restaurant with The Equipment vessel vents when it is not in use. your portable oxygen source, sit There are three common ways of An oxygen-conserving device may in the nonsmoking section and providing oxygen therapy. Oxygen be built into the vessel to conserve away from any open flame such can be delivered to your home in as candles or warming burners. -
Nitrogen Oxides (Nox), Why and How They Are Controlled
United States Office of Air Quality EPA 456/F-99-006R Environmental Protection Planning and Standards November 1999 Agency Research Triangle Park, NC 27711 Air EPA-456/F-99-006R November 1999 Nitrogen Oxides (NOx), Why and How They Are Controlled Prepared by Clean Air Technology Center (MD-12) Information Transfer and Program Integration Division Office of Air Quality Planning and Standards U.S. Environmental Protection Agency Research Triangle Park, North Carolina 27711 DISCLAIMER This report has been reviewed by the Information Transfer and Program Integration Division of the Office of Air Quality Planning and Standards, U.S. Environmental Protection Agency and approved for publication. Approval does not signify that the contents of this report reflect the views and policies of the U.S. Environmental Protection Agency. Mention of trade names or commercial products is not intended to constitute endorsement or recommendation for use. Copies of this report are available form the National Technical Information Service, U.S. Department of Commerce, 5285 Port Royal Road, Springfield, Virginia 22161, telephone number (800) 553-6847. CORRECTION NOTICE This document, EPA-456/F-99-006a, corrects errors found in the original document, EPA-456/F-99-006. These corrections are: Page 8, fourth paragraph: “Destruction or Recovery Efficiency” has been changed to “Destruction or Removal Efficiency;” Page 10, Method 2. Reducing Residence Time: This section has been rewritten to correct for an ambiguity in the original text. Page 20, Table 4. Added Selective Non-Catalytic Reduction (SNCR) to the table and added acronyms for other technologies. Page 29, last paragraph: This paragraph has been rewritten to correct an error in stating the configuration of a typical cogeneration facility. -

The Elements.Pdf
A Periodic Table of the Elements at Los Alamos National Laboratory Los Alamos National Laboratory's Chemistry Division Presents Periodic Table of the Elements A Resource for Elementary, Middle School, and High School Students Click an element for more information: Group** Period 1 18 IA VIIIA 1A 8A 1 2 13 14 15 16 17 2 1 H IIA IIIA IVA VA VIAVIIA He 1.008 2A 3A 4A 5A 6A 7A 4.003 3 4 5 6 7 8 9 10 2 Li Be B C N O F Ne 6.941 9.012 10.81 12.01 14.01 16.00 19.00 20.18 11 12 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 3 Na Mg IIIB IVB VB VIB VIIB ------- VIII IB IIB Al Si P S Cl Ar 22.99 24.31 3B 4B 5B 6B 7B ------- 1B 2B 26.98 28.09 30.97 32.07 35.45 39.95 ------- 8 ------- 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 4 K Ca Sc Ti V Cr Mn Fe Co Ni Cu Zn Ga Ge As Se Br Kr 39.10 40.08 44.96 47.88 50.94 52.00 54.94 55.85 58.47 58.69 63.55 65.39 69.72 72.59 74.92 78.96 79.90 83.80 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 5 Rb Sr Y Zr NbMo Tc Ru Rh PdAgCd In Sn Sb Te I Xe 85.47 87.62 88.91 91.22 92.91 95.94 (98) 101.1 102.9 106.4 107.9 112.4 114.8 118.7 121.8 127.6 126.9 131.3 55 56 57 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 6 Cs Ba La* Hf Ta W Re Os Ir Pt AuHg Tl Pb Bi Po At Rn 132.9 137.3 138.9 178.5 180.9 183.9 186.2 190.2 190.2 195.1 197.0 200.5 204.4 207.2 209.0 (210) (210) (222) 87 88 89 104 105 106 107 108 109 110 111 112 114 116 118 7 Fr Ra Ac~RfDb Sg Bh Hs Mt --- --- --- --- --- --- (223) (226) (227) (257) (260) (263) (262) (265) (266) () () () () () () http://pearl1.lanl.gov/periodic/ (1 of 3) [5/17/2001 4:06:20 PM] A Periodic Table of the Elements at Los Alamos National Laboratory 58 59 60 61 62 63 64 65 66 67 68 69 70 71 Lanthanide Series* Ce Pr NdPmSm Eu Gd TbDyHo Er TmYbLu 140.1 140.9 144.2 (147) 150.4 152.0 157.3 158.9 162.5 164.9 167.3 168.9 173.0 175.0 90 91 92 93 94 95 96 97 98 99 100 101 102 103 Actinide Series~ Th Pa U Np Pu AmCmBk Cf Es FmMdNo Lr 232.0 (231) (238) (237) (242) (243) (247) (247) (249) (254) (253) (256) (254) (257) ** Groups are noted by 3 notation conventions. -

SDS # : 002074 Supplier's Details : Airgas USA, LLC and Its Affiliates 259 North Radnor-Chester Road Suite 100 Radnor, PA 19087-5283 1-610-687-5253
SAFETY DATA SHEET Oxidizing Gas Mixture: Nitrogen 1ppm-76.5% / Oxygen 23.5-99.9999% Section 1. Identification GHS product identifier : Oxidizing Gas Mixture: Nitrogen 1ppm-76.5% / Oxygen 23.5-99.9999% Other means of : Not available. identification Product type : Gas. Product use : Synthetic/Analytical chemistry. SDS # : 002074 Supplier's details : Airgas USA, LLC and its affiliates 259 North Radnor-Chester Road Suite 100 Radnor, PA 19087-5283 1-610-687-5253 24-hour telephone : 1-866-734-3438 Section 2. Hazards identification OSHA/HCS status : This material is considered hazardous by the OSHA Hazard Communication Standard (29 CFR 1910.1200). Classification of the : OXIDIZING GASES - Category 1 substance or mixture GASES UNDER PRESSURE - Compressed gas GHS label elements Hazard pictograms : Signal word : Danger Hazard statements : May cause or intensify fire; oxidizer. Contains gas under pressure; may explode if heated. Precautionary statements General : Read and follow all Safety Data Sheets (SDS’S) before use. Read label before use. Keep out of reach of children. If medical advice is needed, have product container or label at hand. Close valve after each use and when empty. Use equipment rated for cylinder pressure. Do not open valve until connected to equipment prepared for use. Use a back flow preventative device in the piping. Use only equipment of compatible materials of construction. Open valve slowly. Use only with equipment cleaned for Oxygen service. Prevention : Keep away from clothing, incompatible materials and combustible materials. Keep reduction valves, valves and fittings free from oil and grease. Response : In case of fire: Stop leak if safe to do so. -
The Role of Oxygen and Hydrogen in Refining
Strategic links: The role of oxygen and hydrogen in refining. Authors M. Marquez and X. Tian Date October 2016 First published in Hydrocarbon Engineering Magazine APPLicaTION TecHNOLOGieS → O₂ enrichment Emission reduction Water treatment Industrial services Complementary offering 02 Strategic links: The role of oxygen and hydrogen in refining. The commoditised refining industry finds itself subject to ever increasing competitive pressures. In mature markets small and mid-sized refineries have to compete with large, integrated complexes recently built in emerging markets which enjoy the benefits of easier access to feedstock and lower labour costs, a situation exacerbated by the costs of creating low sulfur fuels from heavier, more sour crude, as the world’s crude oil resources dwindle. The sulfur content of the world’s diminishing crude oil resources is Effective from 1 January 2015, the SCAQMD’s Rule 1146 limits NOx higher than ever before as oil companies are forced to tap into a releases from industrial and commercial boilers, steam generators and cheaper but lower quality of crude that requires more refining to process heaters to less than 9 parts per million (ppm). By 2016, the meet tightening environmental standards and while maximising threshold for NOx emissions will fall to 5 ppm or lower. Looking ahead, margins. To be competitive in this challenging landscape, modern other geographies are bound to follow suit with tighter NOx controls refineries must operate efficiently, ensure adequate capacity, and that are more in line with the Californian example. control emission levels. Operators are therefore keen to maximise profitability factors, often by optimising the efficiency of their assets. -

WATER MOLECULES FORM HYDROGEN BONDS Water Is a Fundamental Requirement for Life, So It Is Important to Understand the Structural and Chemical Properties of Water
Water H2O Liquid, solid, and vapor coexist in the same environment WATER MOLECULES FORM HYDROGEN BONDS Water is a fundamental requirement for life, so it is important to understand the structural and chemical properties of water. Most biological molecules are surrounded by water, and even their molecular structure is in part governed by how their component groups interact with water. Water plays a role in how biological molecules assemble to form larger structures or undergo chemical transformation. In fact, water itself—or its H+ and OH- constituents—participates directly in many biochemical processes. The central O atom forms covalent bonds with two H atoms, leaving two unshared pairs of electrons. The molecule has approximately tetrahedral geometry, with the O atom at the center of the tetrahedron, the H atoms at two of the four corners, and electrons at the other two corners. The electrical charge is therefore polarized: Water is a highly polar molecule. Water: Hydrogen-bonding network Hydrogen bonds are found between molecules of water and molecules of ammonia. They are defined as the attractive interaction between a hydrogen atom bonded to a very electronegative atom (O, N, or F) and an unshared electron pair on another electronegative atom. Liquid water contains a vast three-dimensional network of hydrogen bonds resulting from the attraction between positively polarized hydrogens and electron pairs on negatively polarized oxygens. Each oxygen can form two hydrogen bonds, represented by dotted lines. Hydrogen bonding cont’d As a result of this electronic arrangement, the water molecule is polar; that is, it has an uneven distribution of charge. -

Medical Oxygen Safety
Medical Oxygen Safety Portable medical oxygen in the home has grown over the past decade. Medical oxygen adds a higher percentage of oxygen to the air a patient uses to breathe. Fire needs oxygen to burn. If a fire should start in an oxygen-enriched area, the material burning will burn more quickly. Homes where medical oxygen is used need specific fire safety rules to keep people safe from fire and burns. FACTS SAFETY TIPS ! Oxygen saturates fabric • covered furniture, clothing, KKK There is no safe way to smoke in the home when oxygen is in use. A patient on oxygen hair and bedding, making it easier for a fire to start and should not smoke. spread. KKK Candles, matches, wood stoves and even ! Smoking materials is the sparking toys, can be ignition sources and • leading heat source resulting should not be used in the home. in medical oxygen related fires, injuries and deaths. KKK Keep oxygen cylinders at least five feet from a heat source, open flames or electrical devices. KKK Body oil, hand lotion and items containing oil and grease can easily ignite. Keep oil and grease away where oxygen is in use. Post No Smoking and No Open Flames signs KKK Never use aerosol sprays containing in and outside the home to combustible materials near the oxygen. remind people not to smoke. Your Source for SAFETY Information NFPA Public Education Division • 1 Batterymarch Park, Quincy, MA 02169 www.nfpa.org/education ©NFPA 2016.