Amphetamine Use Among Workers with Severe Hyperthermia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(19) United States (12) Patent Application Publication (10) Pub
US 20130289061A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2013/0289061 A1 Bhide et al. (43) Pub. Date: Oct. 31, 2013 (54) METHODS AND COMPOSITIONS TO Publication Classi?cation PREVENT ADDICTION (51) Int. Cl. (71) Applicant: The General Hospital Corporation, A61K 31/485 (2006-01) Boston’ MA (Us) A61K 31/4458 (2006.01) (52) U.S. Cl. (72) Inventors: Pradeep G. Bhide; Peabody, MA (US); CPC """"" " A61K31/485 (201301); ‘4161223011? Jmm‘“ Zhu’ Ansm’ MA. (Us); USPC ......... .. 514/282; 514/317; 514/654; 514/618; Thomas J. Spencer; Carhsle; MA (US); 514/279 Joseph Biederman; Brookline; MA (Us) (57) ABSTRACT Disclosed herein is a method of reducing or preventing the development of aversion to a CNS stimulant in a subject (21) App1_ NO_; 13/924,815 comprising; administering a therapeutic amount of the neu rological stimulant and administering an antagonist of the kappa opioid receptor; to thereby reduce or prevent the devel - . opment of aversion to the CNS stimulant in the subject. Also (22) Flled' Jun‘ 24’ 2013 disclosed is a method of reducing or preventing the develop ment of addiction to a CNS stimulant in a subj ect; comprising; _ _ administering the CNS stimulant and administering a mu Related U‘s‘ Apphcatlon Data opioid receptor antagonist to thereby reduce or prevent the (63) Continuation of application NO 13/389,959, ?led on development of addiction to the CNS stimulant in the subject. Apt 27’ 2012’ ?led as application NO_ PCT/US2010/ Also disclosed are pharmaceutical compositions comprising 045486 on Aug' 13 2010' a central nervous system stimulant and an opioid receptor ’ antagonist. -

Toxicology Times
TOXICOLOGY (800) 677-7995 TIMES www.sdrl.com A FREE Monthly Newsletter for Substance Abuse and Opioid Treatment Volume 5, Issue 7 Programs from San Diego Reference Laboratory July, 2015 Amphetamines (Part 1) Dr. Joseph E. Graas, Scientific Director most often used in inhalers and does not tite, increased stamina and physical energy, Dr. Edward Moore, Medical Director have the central nervous system activity nor increased sexual response/drive, involuntary any addictive properties. All of the com- body movements, increased perspiration, The term “amphetamines” has come to mean pounds that have the structure of hyperactivity, nausea and increased heart rate. a class of endogenous neurotransmitters that phenylethylamine will have this mixture of d This drug is highly addictive and tolerance stimulate the sympathetic nervous system. and l molecules. In the production of these develops quickly. Withdrawal is an extremely This is a broad class of various substituted drugs they are usually noted as a racemic unpleasant experience. A few street names derivatives of phenylethylamine. This grow- mixture, or specifically, as the d or l com- for the drug are amp, speed, crank, dolls and ing class of structurally related molecules may pound. To properly evaluate this family of crystal. also stimulate the sympathetic nervous sys- compounds known as sympathomimetic tem in many different ways, such as affecting amines, amphetamines or phenylethylamine, Methamphetamine was developed by the the re-release of neurotransmitters or pre- it is best done by describing each member of Japanese in 1919 and used during World War venting the re-uptake of neurotransmitters, the class: amphetamine , methampheta- II to help soldiers stay alert and energize hallucinogens, anorectics, bronchodilators mine , phentermine , phenylpropanola- factory workers. -

Stimulant and Related Medications: US Food and Drug
Stimulant and Related Medications: U.S. Food and Drug Administration-Approved Indications and Dosages for Use in Adults The therapeutic dosing recommendations for stimulant and related medications are based on U.S. Food and Drug Administration (FDA)-approved product labeling. Nevertheless, the dosing regimen is adjusted according to a patient’s individual response to pharmacotherapy. The FDA-approved dosages and indications for the use of stimulant and related medications in adults are provided in this table. All medication doses listed are for oral administration. Information on the generic availability of the stimulant and related medications can be found by searching the Electronic Orange Book at https://www.accessdata.fda.gov/scripts/cder/ob/default.cfm on the FDA website. Generic Medication Indication Dosing Information Other Information Availability amphetamine/dextroamphetamine ADHD Initial dose: May increase daily dose by 5 mg at Yes mixed salts[1] 5 mg once or twice a day; weekly intervals until optimal response Maximum dose: 40 mg per day is achieved. Only in rare cases will it be necessary to exceed a total of 40 mg per day. amphetamine/dextroamphetamine narcolepsy Initial dose: 10 mg per day; May increase daily dose by 10 mg at Yes mixed salts Usual dose: weekly intervals until optimal response 5 mg to 60 mg per day is achieved. Take first dose in divided doses upon awakening. amphetamine/dextroamphetamine ADHD Recommended dose: Patients switching from regular-release Yes mixed salts ER*[2] 20 mg once a day amphetamine/dextroamphetamine mixed salts may take the same total daily dose once a day. armodafinil[3] narcolepsy Recommended dose: Take as a single dose in the morning. -

Monoamine Reuptake Inhibitors in Parkinson's Disease
Hindawi Publishing Corporation Parkinson’s Disease Volume 2015, Article ID 609428, 71 pages http://dx.doi.org/10.1155/2015/609428 Review Article Monoamine Reuptake Inhibitors in Parkinson’s Disease Philippe Huot,1,2,3 Susan H. Fox,1,2 and Jonathan M. Brotchie1 1 Toronto Western Research Institute, Toronto Western Hospital, University Health Network, 399 Bathurst Street, Toronto, ON, Canada M5T 2S8 2Division of Neurology, Movement Disorder Clinic, Toronto Western Hospital, University Health Network, University of Toronto, 399BathurstStreet,Toronto,ON,CanadaM5T2S8 3Department of Pharmacology and Division of Neurology, Faculty of Medicine, UniversitedeMontr´ eal´ and Centre Hospitalier de l’UniversitedeMontr´ eal,´ Montreal,´ QC, Canada Correspondence should be addressed to Jonathan M. Brotchie; [email protected] Received 19 September 2014; Accepted 26 December 2014 Academic Editor: Maral M. Mouradian Copyright © 2015 Philippe Huot et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. The motor manifestations of Parkinson’s disease (PD) are secondary to a dopamine deficiency in the striatum. However, the degenerative process in PD is not limited to the dopaminergic system and also affects serotonergic and noradrenergic neurons. Because they can increase monoamine levels throughout the brain, monoamine reuptake inhibitors (MAUIs) represent potential therapeutic agents in PD. However, they are seldom used in clinical practice other than as antidepressants and wake-promoting agents. This review article summarises all of the available literature on use of 50 MAUIs in PD. The compounds are divided according to their relative potency for each of the monoamine transporters. -

Established Aggregate Production Quotas for Schedule I and II
59980 Federal Register / Vol. 77, No. 190 / Monday, October 1, 2012 / Notices DEPARTMENT OF JUSTICE for Schedule I and II Controlled information, DEA has determined that Substances and Proposed Assessment of adjustments to the proposed aggregate Drug Enforcement Administration Annual Needs for the List I Chemicals production quotas and assessment of [Docket No. DEA–365] Ephedrine, Pseudoephedrine, and annual needs for 3,4-methylenedioxy-N- Phenylpropanolamine for 2013,’’ was methylcathinone (methylone), Established Aggregate Production published in the Federal Register (77 3,4,methylenedioxypyrovalerone Quotas for Schedule I and II Controlled FR 46519). That notice proposed the (MDPV), 4-methyl-N-methylcathinone Substances and Established 2013 aggregate production quotas for (mephedrone), N-benzylpiperazine, Assessment of Annual Needs for the each basic class of controlled substance amphetamine (for conversion), List I Chemicals Ephedrine, listed in schedules I and II and the 2013 amphetamine (for sale), hydrocodone Pseudoephedrine, and assessment of annual needs for the list (for sale), hydromorphone, Phenylpropanolamine for 2013 I chemicals ephedrine, lisdexamfetamine, methylphenidate, pseudoephedrine, and morphine (for sale), oxycodone (for AGENCY: Drug Enforcement phenylpropanolamine. All interested sale), oxymorphone (for conversion), Administration (DEA), Department of persons were invited to comment on or remifentanil, sufentanil, tapentadol, Justice. object to the proposed aggregate ephedrine (for conversion), ephedrine ACTION: -

A Dose-Escalating, Phase-2 Study of Oral Lisdexamfetamine
Ezard et al. BMC Psychiatry (2016) 16:428 DOI 10.1186/s12888-016-1141-x STUDY PROTOCOL Open Access Study protocol: a dose-escalating, phase-2 study of oral lisdexamfetamine in adults with methamphetamine dependence Nadine Ezard1,2, Adrian Dunlop3, Brendan Clifford1* , Raimondo Bruno4, Andrew Carr5, Alexandra Bissaker1 and Nicholas Lintzeris6,7 Abstract Background: The treatment of methamphetamine dependence is a continuing global health problem. Agonist type pharmacotherapies have been used successfully to treat opioid and nicotine dependence and are being studied for the treatment of methamphetamine dependence. One potential candidate is lisdexamfetamine, a pro-drug for dexamphetamine, which has a longer lasting therapeutic action with a lowered abuse potential. The purpose of this study is to determine the safety of lisdexamfetamine in this population at doses higher than those currently approved for attention deficit hyperactivity disorder or binge eating disorder. Methods/design: This is a phase 2 dose escalation study of lisdexamfetamine for the treatment of methamphetamine dependence. Twenty individuals seeking treatment for methamphetamine dependence will be recruited at two Australian drug and alcohol services. All participants will undergo a single-blinded ascending-descending dose regime of 100 to 250 mg lisdexamfetamine, dispensed daily on site, over an 8-week period. Participants will be offered counselling as standard care. For the primary objectives the outcome variables will be adverse events monitoring, drug tolerability and regimen completion. Secondary outcomes will be changes in methamphetamine use, craving, withdrawal, severity of dependence, risk behaviour and other substance use. Medication acceptability, potential for non-prescription use, adherence and changes in neurocognition will also be measured. -

Product Monograph
PRODUCT MONOGRAPH VYVANSE®* lisdexamfetamine dimesylate Capsules: 10 mg, 20 mg, 30 mg, 40 mg, 50 mg, 60 mg and 70 mg Chewable Tablets: 10 mg, 20 mg, 30 mg, 40 mg, 50 mg and 60 mg Central Nervous System Stimulant Takeda Canada Inc. Date of Preparation: 22 Adelaide Street West, Suite 3800 19 February 2009 Toronto, Ontario M5H 4E3 Date of Revision: July 21, 2020 Submission Control No.: 240669 *VYVANSE® and the VYVANSE Logo are registered trademarks of Shire LLC, a Takeda company. Takeda and the Takeda Logo are trademarks of Takeda Pharmaceutical Company Limited, used under license. © 2020 Takeda Pharmaceutical Company Limited. All rights reserved. Pa ge 1 of 60 TABLE OF CONTENTS PART I: HEALTH PROFESSIONAL INFORMATION .................................................... 3 SUMMARY PRODUCT INFORMATION ................................................................... 3 INDICATIONS AND CLINICAL USE ........................................................................ 3 CONTRAINDICATIONS ............................................................................................ 5 WARNINGS AND PRECAUTIONS ............................................................................ 6 ADVERSE REACTIONS........................................................................................... 12 DRUG INTERACTIONS ........................................................................................... 23 DOSAGE AND ADMINISTRATION ........................................................................ 25 OVERDOSAGE ....................................................................................................... -

Pharmacy Prior Authorization Guideline 1. Criteria
Harvard Pilgrim Health Care – Pharmacy Prior Authorization Guideline Guideline Name ADHD Medications: Adderall (amphetamine-dextroamphetamine mixed salts), Adderall XR (amphetamine-dextroamphetamine mixed salts extended-release), Adzenys ER (amphetamine), Adzenys XR-ODT (amphetamine), Aptensio XR (methylphenidate), amphetamine, amphetamine-dextroamphetamine mixed salts, amphetamine-dextroamphetamine mixed salts extended-release, Concerta (methylphenidate), Cotempla-XR ODT (methylphenidate), Daytrana (methylphenidate), Desoxyn (methamphetamine), Dexedrine (dextroamphetamine), dexmethylphenidate, dexmethylphenidate extended- release, dextroamphetamine, dextroamphetamine extended-release, dextroamphetamine oral solution, Dyanavel XR (amphetamine), Evekeo (amphetamine), Focalin (dexmethylphenidate), Focalin XR (dexmethylphenidate), Jornay PM (methylphenidate), Metadate ER (methylphenidate), methamphetamine, Methylin oral solution (methylphenidate), methylphenidate, methylphenidate chewable tablets, methylphenidate extended-release, methylphenidate extended-release (CD), methylphenidate extended-release (LA), methylphenidate extended- release OSM, methylphenidate oral solution, Mydayis (amphetamine- dextroamphetamine), Procentra (dextroamphetamine), Quillivant XR (methylphenidate), Quillichew ER (methylphenidate), Relexxii (methylphenidate), Ritalin (methylphenidate), Ritalin LA (methylphenidate), Vyvanse (lisdexamfetamine), and Zenzedi (dextroamphetamine) 1. Criteria Product Name: Brand Adderall, Generic amphetamine-dextroamphetamine mixed -

(12) Patent Application Publication (10) Pub. No.: US 2015/0202317 A1 Rau Et Al
US 20150202317A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2015/0202317 A1 Rau et al. (43) Pub. Date: Jul. 23, 2015 (54) DIPEPTDE-BASED PRODRUG LINKERS Publication Classification FOR ALPHATIC AMNE-CONTAINING DRUGS (51) Int. Cl. A647/48 (2006.01) (71) Applicant: Ascendis Pharma A/S, Hellerup (DK) A638/26 (2006.01) A6M5/9 (2006.01) (72) Inventors: Harald Rau, Heidelberg (DE); Torben A 6LX3/553 (2006.01) Le?mann, Neustadt an der Weinstrasse (52) U.S. Cl. (DE) CPC ......... A61K 47/48338 (2013.01); A61 K3I/553 (2013.01); A61 K38/26 (2013.01); A61 K (21) Appl. No.: 14/674,928 47/48215 (2013.01); A61M 5/19 (2013.01) (22) Filed: Mar. 31, 2015 (57) ABSTRACT The present invention relates to a prodrug or a pharmaceuti Related U.S. Application Data cally acceptable salt thereof, comprising a drug linker conju (63) Continuation of application No. 13/574,092, filed on gate D-L, wherein D being a biologically active moiety con Oct. 15, 2012, filed as application No. PCT/EP2011/ taining an aliphatic amine group is conjugated to one or more 050821 on Jan. 21, 2011. polymeric carriers via dipeptide-containing linkers L. Such carrier-linked prodrugs achieve drug releases with therapeu (30) Foreign Application Priority Data tically useful half-lives. The invention also relates to pharma ceutical compositions comprising said prodrugs and their use Jan. 22, 2010 (EP) ................................ 10 151564.1 as medicaments. US 2015/0202317 A1 Jul. 23, 2015 DIPEPTDE-BASED PRODRUG LINKERS 0007 Alternatively, the drugs may be conjugated to a car FOR ALPHATIC AMNE-CONTAINING rier through permanent covalent bonds. -

Chiral Separation of Methamphetamine and Amphetamine on an Agilent Infinitylab Poroshell 120 Chiral-V Column with Detection by LC/MS
Application Note Clinical Research Chiral separation of methamphetamine and amphetamine on an Agilent InfinityLab Poroshell 120 Chiral-V column with detection by LC/MS Authors Abstract Carl Griffin and William Long An Agilent InfinityLab Poroshell 120 Chiral-V 2.1 × 150 mm, 2.7 μm column Agilent Technologies, Inc. (p/n 683775-604) was used to analyze methamphetamine and amphetamine Wilmington, DE, USA by LC/MS, using a mobile phase of methanol with 0.1 % acetic acid and 0.02 % ammonium hydroxide. The analysis was accomplished in 5 minutes, with a resolution Rs of 1.9 or better for racemic amphetamine and methamphetamine. Introduction H NH Experimental N 2 Superficially porous particle columns are An Agilent 1290 Infinity LC system CH3 a popular tool in liquid chromatography. with an Agilent 6460 triple quadrupole Superficially porous particle columns (S)-(+)-Methamphetamine (S)-(+)-Amphetamine LC/MS was used in this experiment. The generate high efficiency at lower Dextromethamphetamine Dextroamphetamine system was modified from its standard pressure relative to their totally porous configuration to have low system volume 1 particle column counterparts . This is H NH and dispersion. Table 1 shows the primarily due to a shorter mass transfer N 2 instrument configuration details. Table 1 distance and substantially narrower CH lists the Agilent InfinityLab Poroshell 120 particle size distribution of the particles 3 Chiral-V 2.1 × 150 mm, 2.7 μm column in the column2. The current trend with (R)-(–)-Methamphetamine (R)-(–)-Amphetamine used in this work. Table 2 shows the LC superficially porous particles is reducing Levomethamphetamine Levoamphetamine and MS parameters. -
Testing for Amphetamine and Methamphetamine Abuse Using
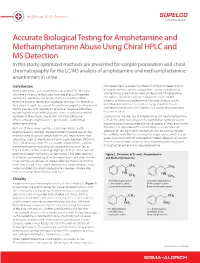
Healthcare & Life Sciences Accurate Biological Testing for Amphetamine and Methamphetamine Abuse Using Chiral HPLC and MS Detection In this study, optimized methods are presented for sample preparation and chiral chromatography for the LC/MS analysis of amphetamine and methamphetamine enantiomers in urine. Introduction from several tens to several hundreds of milligrams, depending on Methamphetamine and amphetamine, powerful CNS stimulants the purity and the isomeric composition, and will metabolize to 3 that have a variety of ethical uses, have side effects of increased amphetamine and 4-hydroxymethamphetamine. Amphetamine confidence, sociability, and energy that have resulted in their metabolizes mainly to 1-phenyl-2-propanone, with smaller extensive abuse as recreational psychoactive drugs. This extends to amounts of 4-hydroxyamphetamine. However, since up to 54% their abuse in sports because of the additional properties of increased of methamphetamine is excreted unchanged and 10-23% as mental alertness and suppression of fatigue.1 Negative side effects amphetamine following oral ingestion, it is usually the parent drug 1 include hypertension and tachycardia. In the usually uncontrolled that is monitored. situations of drug abuse, they exhibit similar psychoactive Culpability for the illicit use of amphetamine and methamphetamine effects, although amphetamine is generally less potent than rests on the ability to distinguish the contribution to the measured methamphetamine. abused product from possible alternative sources of the L-enantiomer. Illicit use of these drugs continues to be high. Public Health Therefore, the separation of the enantiomers is a more accurate England recently reported that the number of people stating their approach for testing. A chiral method can also be used to indicate main injecting drug to be amphetamines and amphetamine-type the synthetic route that was used by the illegal source, which can be substances (such as mephedrone) nearly tripled between 2002 and useful as part of a criminal investigation. -
ATC) Codes and Drug Identification Numbers (Dins
Anatomical Therapeutic Chemical (ATC) Codes and Drug Identification Numbers (DINs) of Drugs in the Drug Program Information Network (DPIN) Used to Define Attention Deficit Hyperactivity Disorder (ADHD) in Manitoba Children from 2000/01 to 2009/10 DIN ATC Code Equivalent Generic Product Name Product Description Ingredients AMPHETAMINE ASPARTATE MONOHYDRATE (1.25 MG)/AMPHETAMINE SULFATE (1.25 MG)/DEXTROAMPHETAMINE SACCHARATE (1.25 MG)/DEXTROAMPHETAMINE SULFATE 2248808 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR (1.25 MG) AMPHETAMINE ASPARTATE MONOHYDRATE (2.5 MG)/AMPHETAMINE SULFATE (2.5 MG)/DEXTROAMPHETAMINE SACCHARATE (2.5 MG)/DEXTROAMPHETAMINE SULFATE (2.5 2248809 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR MG) AMPHETAMINE ASPARTATE MONOHYDRATE (3.75 MG)/AMPHETAMINE SULFATE (3.75 MG)/DEXTROAMPHETAMINE SACCHARATE (3.75 MG)/DEXTROAMPHETAMINE SULFATE 2248810 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR (3.75 MG) AMPHETAMINE ASPARTATE MONOHYDRATE (5 MG)/AMPHETAMINE SULFATE (5 2248811 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR MG)/DEXTROAMPHETAMINE SACCHARATE (5 MG)/DEXTROAMPHETAMINE SULFATE (5 MG) AMPHETAMINE ASPARTATE MONOHYDRATE (6.25 MG)/AMPHETAMINE SULFATE (6.25 MG)/DEXTROAMPHETAMINE SACCHARATE (6.25 MG)/DEXTROAMPHETAMINE SULFATE 2248812 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR (6.25 MG) AMPHETAMINE ASPARTATE MONOHYDRATE (7.5 MG)/AMPHETAMINE SULFATE (7.5 MG)/DEXTROAMPHETAMINE SACCHARATE (7.5 MG)/DEXTROAMPHETAMINE SULFATE (7.5 2248813 N06BA01 MIXED SALT AMPHETAMINE ADDERALL XR MG) 1924516 N06BA02 DEXTROAMPHETAMINE SULFATE DEXEDRINE DEXTROAMPHETAMINE