Using the Rewarding Value of Food and Sensitivity to Reward to Improve the Snacking Behavior of Adolescents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Battery Life Test Results HUAWEI TOSHIBA INTEX PLUM
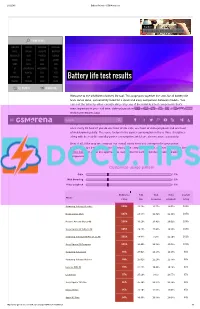
2/12/2015 Battery life tests GSMArena.com Starborn SAMSUNG GALAXY S6 EDGE+ REVIEW PHONE FINDER SAMSUNG LENOVO VODAFONE VERYKOOL APPLE XIAOMI GIGABYTE MAXWEST MICROSOFT ACER PANTECH CELKON NOKIA ASUS XOLO GIONEE SONY OPPO LAVA VIVO LG BLACKBERRY MICROMAX NIU HTC ALCATEL BLU YEZZ MOTOROLA ZTE SPICE PARLA Battery life test results HUAWEI TOSHIBA INTEX PLUM ALL BRANDS RUMOR MILL Welcome to the GSMArena battery life tool. This page puts together the stats for all battery life tests we've done, conveniently listed for a quick and easy comparison between models. You can sort the table by either overall rating or by any of the individual test components that's most important to you call time, video playback or web browsing.TIP US 828K 100K You can find all about our84K 137K RSS LOG IN SIGN UP testing procedures here. SearchOur overall rating gives you an idea of how much battery backup you can get on a single charge. An overall rating of 40h means that you'll need to fully charge the device in question once every 40 hours if you do one hour of 3G calls, one hour of video playback and one hour of web browsing daily. The score factors in the power consumption in these three disciplines along with the reallife standby power consumption, which we also measure separately. Best of all, if the way we compute our overall rating does not correspond to your usage pattern, you are free to adjust the different usage components to get a closer match. Use the sliders below to adjust the approximate usage time for each of the three battery draining components. -

Electronic 3D Models Catalogue (On July 26, 2019)
Electronic 3D models Catalogue (on July 26, 2019) Acer 001 Acer Iconia Tab A510 002 Acer Liquid Z5 003 Acer Liquid S2 Red 004 Acer Liquid S2 Black 005 Acer Iconia Tab A3 White 006 Acer Iconia Tab A1-810 White 007 Acer Iconia W4 008 Acer Liquid E3 Black 009 Acer Liquid E3 Silver 010 Acer Iconia B1-720 Iron Gray 011 Acer Iconia B1-720 Red 012 Acer Iconia B1-720 White 013 Acer Liquid Z3 Rock Black 014 Acer Liquid Z3 Classic White 015 Acer Iconia One 7 B1-730 Black 016 Acer Iconia One 7 B1-730 Red 017 Acer Iconia One 7 B1-730 Yellow 018 Acer Iconia One 7 B1-730 Green 019 Acer Iconia One 7 B1-730 Pink 020 Acer Iconia One 7 B1-730 Orange 021 Acer Iconia One 7 B1-730 Purple 022 Acer Iconia One 7 B1-730 White 023 Acer Iconia One 7 B1-730 Blue 024 Acer Iconia One 7 B1-730 Cyan 025 Acer Aspire Switch 10 026 Acer Iconia Tab A1-810 Red 027 Acer Iconia Tab A1-810 Black 028 Acer Iconia A1-830 White 029 Acer Liquid Z4 White 030 Acer Liquid Z4 Black 031 Acer Liquid Z200 Essential White 032 Acer Liquid Z200 Titanium Black 033 Acer Liquid Z200 Fragrant Pink 034 Acer Liquid Z200 Sky Blue 035 Acer Liquid Z200 Sunshine Yellow 036 Acer Liquid Jade Black 037 Acer Liquid Jade Green 038 Acer Liquid Jade White 039 Acer Liquid Z500 Sandy Silver 040 Acer Liquid Z500 Aquamarine Green 041 Acer Liquid Z500 Titanium Black 042 Acer Iconia Tab 7 (A1-713) 043 Acer Iconia Tab 7 (A1-713HD) 044 Acer Liquid E700 Burgundy Red 045 Acer Liquid E700 Titan Black 046 Acer Iconia Tab 8 047 Acer Liquid X1 Graphite Black 048 Acer Liquid X1 Wine Red 049 Acer Iconia Tab 8 W 050 Acer -

HANDLEBAR MOUNTED SMARTPHONE/GPS HOLDER 8524 Handlebar Mounted Case for Various Smartphones
HANDLEBAR MOUNTED SMARTPHONE/GPS HOLDER 8524 Handlebar mounted case for various smartphones. • 360 degrees adjustable, quick release system. • Sunshade visor. No ITL • External water-resistant case and additional rain cover included. 076-S955B • Screen compatible with iPhone, GPS or other touch screens. • Security strip to prevent accidental falls. • Battery charger wire holder. No ITL No ITL 076-S953B 076-S954B No ITL No ITL No ITL 076-S956B 076-S957B 076-S952 076-S952B Application Inner size No ITL Universal, screens up to 3,5" 12,5 x 8,5cm 076-S952 Universal, screens up to 3,5" 12,5 x 8,5cm 076-S952B Universal, screens up to 4,3" 14,0 x 9,0cm 076-S953B Universal, screens up to 5,0" 16,0 x 10,5cm 076-S954B No ITL I-phone 5 13,0 x 7,0cm 076-S955B 076-S951KIT I-phone 6/Samsung S5 14,3 x 7,1cm 076-S956B Description No ITL I-phone 6+/Samsung Note 4 16,1 x 8,3cm 076-S957B Universal mounting kit 076-S951KIT2* Mounting kit 076-S951BKITR** * For models: S950, S952, S956B, S957B COMPATIBILITY CHART ** For models: S952B, S953B, S954B, S955B S953B S954B S954B S957B • Samsung Galaxy S5 mini • Motorola Moto X Force • Tom Tom Rider 40, • LG G5 • Samsung Galaxy A3 2016) • Motorola Moto X Play • Tom Tom Rider 400, • LG Ray S954B • Motorola Moto X Style • Tom Tom go 51, • LG K5 • Apple iPhone 6 • Motorola Moto G (version 2014, 2015) • Tom Tom go 510, • Nokia-Microsoft Lumia 535 • Apple iPhone 6s • Motorola Moto G Turbo Edition • Tom Tom go 5100, • Nokia-Microsoft Lumia 650 • Apple iPhone 6 Plus • Xiaomi Mi 4s • Coyote Nav, • Nokia-Microsoft Lumia 950 • Apple iPhone 6s Plus • Xiaomi Mi 5 Standard Edition/ • Parrot Asteroid Mini, • HTC One A9 • Samsung Galaxy S7 Exclusive Edition • Parrot Asteroid Tablet. -

Microsoft Lumia 435
MICROSOFT LUMIA 435 Configurazione WAP Gli smartphone con sistema operativo Windows Phone si configurano all'accensione in maniera automatica sia per la navigazione, che per la messaggistica MMS, con i parametri del gestore della sim inserita. I parametri di queste configurazioni di default non sono modificabili. In caso di problemi, prevalentemente dovuti a cambi con sim di altro gestore, Windows Phone 8 presenta comunque già nelle impostazioni di fabbrica la possibilità di settare in maniera completamente manuale gli apn per la navigazione (wap.tim.it) e per gli MMS (unico.tim.it). Gli apn impostati manualmente sugli smartphone Lumia con Windows Phone 8, una volta attivati, ''prevalgono'' infatti su quelli che di default lo smartphone rileva dalla Rete secondo il gestore della sim. Per impostare manualmente un apn valido per la navigazione Internet, fai scorrere la schermata Home per accedere al menù delle applicazioni. 1 Scorri la schermata verso il basso. Premi la voce ''Impostazioni''. 2 Scorri anche questa schermata verso il basso. Scegli ora ''rete cellulare e SIM”. 3 Scorri di nuovo verso il basso. Seleziona la voce ''Impostazioni SIM''. 4 Fai scorrere il pulsantino per abilitare l'impostazione dell'APN Internet manuale. Ora puoi impostare i parametri dell'APN manuale. Nel campo ''Nome'' digita ''wap.tim.it', lascia vuoti i campi ''Nome utente'' e ''Password'', quindi scorri la schermata verso il basso. 5 Lascia il resto delle voci impostato come in figura, quindi salva le impostazioni premendo il simbolo in basso a sinistra. Ora le nuove impostazioni sono attive con priorità su quelle impostate di default dalla rete e lo smartphone le utilizzerà per la navigazione. -

Scegli Il Tuo Smartphone
Scegli il tuo Smartphone Per tutti i clienti ricaricabili Listino valido dal 07/09/2015 Descrizione Prodotto Fascia rateizzazione [Entry ticket] MICROSOFT LUMIA 435 3€ x 24 mesi 0€ TIM MODEM WI-FI 4G LTE 3€ x 24 mesi 0€ ZTE Blade G Lux 3€ x 24 mesi 0€ HUAWEI Ascend Y530 3€ x 24 mesi 29€ ZTE Blade A430 3€ x 24 mesi 29€ HUAWEI Ascend Y625 5€ x 24 mesi 0€ LG Leon 5€ x 24 mesi 0€ MICROSOFT LUMIA 535 5€ x 24 mesi 0€ MICROSOFT LUMIA 640 5€ x 24 mesi 0€ SAMSUNG GALAXY J1 5€ x 24 mesi 0€ ZTE Blade A450 5€ x 24 mesi 0€ SAMSUNG GALAXY Core Prime 5€ x 24 mesi 19€ DORO Liberto 820 Mini 5€ x 24 mesi 49€ LG Spirit 5€ x 24 mesi 49€ HUAWEI P8 LITE 5€ x 30 mesi 49€ NOKIA LUMIA 830 5€ x 30 mesi 49€ SAMSUNG GALAXY Grand Prime 5€ x 30 mesi 49€ SONY XPERIA™ M2 5€ x 30 mesi 49€ LG Wine Smart 5€ x 30 mesi 49€ LG G4C 10€ x 24 mesi 0€ HUAWEI Ascend G7 10€ x 24 mesi 49€ SAMSUNG GALAXY A3 10€ x 24 mesi 49€ SONY XPERIA™ M4 10€ x 24 mesi 49€ BlackBerry® Classic 10€ x 30 mesi 99€ HUAWEI P8 10€ x 30 mesi 99€ SAMSUNG GALAXY A5 10€ x 30 mesi 99€ SAMSUNG GALAXY Gear S 10€ x 30 mesi 99€ SAMSUNG GALAXY S5 10€ x 30 mesi 99€ SONY XPERIA™ Z3 15€ x 30 mesi 49€ SAMSUNG GALAXY S6 32GB 15€ x 30 mesi 49€ LG G4 15€ x 30 mesi 99€ SAMSUNG GALAXY S6 64GB 15€ x 30 mesi 99€ SAMSUNG GALAXY S6 Edge 32GB 15€ x 30 mesi 99€ SAMSUNG GALAXY S6 Edge Plus 32 GB 20€ x 30 mesi 99€ SAMSUNG GALAXY S6 Edge 64GB 20€ x 30 mesi 99€ ©2014 Telecom Italia - P.IVA 00488410010 1 Descrizione Prodotto Fascia rateizzazione [Entry ticket] SAMSUNG GALAXY S6 Edge Plus 64 GB 25€ x 30 mesi 99€ SAMSUNG GALAXY Note 4 25€ x 30 mesi 0€ TIM Ricorda: • Tutti i prezzi sono IVA inclusa. -

Fnac Reprise
FNAC REPRISE Liste des smartphones éligibles au programme de reprise au 19/08/2016 ACER LIQUID Z4 APPLE IPHONE 5 BLACK 64GB ACER INCORPORATED LIQUID Z530S APPLE IPHONE 5 WHITE 16GB ACER INCORPORATED LIQUID Z630S APPLE IPHONE 5 WHITE 32GB ALBA ALBA 4.5INCH 5MP 4G 8GB APPLE IPHONE 5 WHITE 64GB ALBA DUAL SIM APPLE IPHONE 5C ALCATEL IDOL 3 8GB APPLE IPHONE 5C BLUE 16GB ALCATEL ONE TOUCH 228 APPLE IPHONE 5C BLUE 32GB ALCATEL ONE TOUCH 903 APPLE IPHONE 5C BLUE 8GB ALCATEL ONE TOUCH 903X APPLE IPHONE 5C GREEN 16GB ALCATEL ONE TOUCH IDOL 2 MINI S APPLE IPHONE 5C GREEN 32GB ALCATEL ONE TOUCH TPOP APPLE IPHONE 5C GREEN 8GB ALCATEL ONETOUCH POP C3 APPLE IPHONE 5C PINK 16GB AMAZON FIRE PHONE APPLE IPHONE 5C PINK 32GB APPLE APPLE WATCH EDITION 42MM APPLE IPHONE 5C PINK 8GB APPLE IPHONE 3G APPLE IPHONE 5C WHITE 16GB APPLE IPHONE 3G BLACK 16GB APPLE IPHONE 5C WHITE 32GB APPLE IPHONE 3G BLACK 8GB APPLE IPHONE 5C WHITE 8GB APPLE IPHONE 3G WHITE 16GB APPLE IPHONE 5C YELLOW 16GB APPLE IPHONE 3GS APPLE IPHONE 5C YELLOW 32GB APPLE IPHONE 3GS 8GB APPLE IPHONE 5C YELLOW 8GB APPLE IPHONE 3GS BLACK 16GB APPLE IPHONE 5S APPLE IPHONE 3GS BLACK 32GB APPLE IPHONE 5S BLACK 16GB APPLE IPHONE 3GS WHITE 16GB APPLE IPHONE 5S BLACK 32GB APPLE IPHONE 3GS WHITE 32GB APPLE IPHONE 5S BLACK 64GB APPLE IPHONE 4 APPLE IPHONE 5S GOLD 16GB APPLE IPHONE 4 BLACK 16GB APPLE IPHONE 5S GOLD 32GB APPLE IPHONE 4 BLACK 32GB APPLE IPHONE 5S GOLD 64GB APPLE IPHONE 4 BLACK 8GB APPLE IPHONE 5S WHITE 16GB APPLE IPHONE 4 WHITE 16GB APPLE IPHONE 5S WHITE 32GB APPLE IPHONE 4 WHITE 32GB APPLE IPHONE -

Roaring Success
ONE-STOP MAG ALL ABOUT APPS... VOLUME 1 | ISSUE 09 | JUNE 2015 | ` 60 Mag Now INDIA’S BIGGEST ONLINE Shopping Site, FLIPKART, has a BEST APP TOO! UBER: A MUST-TRY App for All GMASA 2015 The BIGGEST APP EVENT is a ROARING SUCCESS JUNE 2015 | Volume 01 | Issue 09 BUZZ PLAY ZONE IGADGETS 04 Latest news from the 30 Games and other fun apps 41 world of mobile apps TECH-TALK APP-LY INSTALL 08 GMASA - 2015-Grand Success 32 A feature about apps 42 10 must-have apps used in daily life APP-RAISE SMARTPHONE 48 @EVENTS 18 Reviews of new apps 38 SHOPPING News, Reviews and more about the latest Smartphones Editorial Chief Editor: Venkatesh C R Senior Associate Editor: Padma Iyer Design Consultant: Shakthi Girish Design Head: Sankaran N Senior Designer: Umashankar R Writer: Deacon Joseph Suaiden Contributing Writers: Arun Pradeep, Editorial Coordinators: Raja T M, Ambili S, Maureen Fernando, Content Coordinators: Ratheesh K, Suganya Raj A, Bramakalai R, Vijay Prasanna R C, Preethi. I Advertising Team Leader Sales: Stephen Andrews Business Development Executive: Meenalochini M. Manager Circulation: Vivek Anandan Social Media Coordinator: Mercy Livingstone Website Coordinator: Mangalam Krishna App Coordinator: Senthil Nayagam Printing Press: Safire Offset Printers Special Thanks to... Mr. C. N. Ramdas IAS (R), Chairman, GNG Group of Companies, Greetings readers! Mrs. Nirmala Ramdas, Director, GNG Group of Companies With great pleasure & excitement, here we are with yet Mr. C. R. Rajendran & Mrs. Kamalam another edition of Apps World Mag. As always, this issue comes Rajendran, Directors, Pandian Textiles to you packed with updates on the latest smartphones, gadgets, Mr. -

Arkusz1 Strona 1 MODEL TEL. ALCATEL 3040G
Arkusz1 QTY PRICE NET/ MODEL AVAILABLE UNIT TEL. ALCATEL 3040G- GRADE B (SL) 1 10 EUR TEL. ALCATEL ONE TOUCH 2007D - GRADE B 1 12 EUR TEL. ALCATEL ONE TOUCH 7041X - GRADE C 1 13 EUR TEL. ALCATEL ONETOUCH 2045X - GRADE B 1 10 EUR TEL. ALCATEL ONETOUCH 2045X - GRADE B* 1 8 EUR TEL. ALCATEL ONETOUCH 6030X-GRADE B 1 20 EUR TEL. ALCATEL OT-E221 - GRADE D (SL) 1 3 EUR TEL. ALCATEL PIXI 4 - GRADE D 1 10 EUR TEL. ALCATEL VLE5 - GRADE A (SL) 1 4 EUR TEL. ASUS_T00I ZENFONE 4 - GRADE C 1 40 EUR TEL. ASUS_T00J ZENFONE 5 - GRADE B* 1 55 EUR TEL. BLACKBERRY Classic Q20 - GRADE B*. 1 30 EUR TEL. BLACKBERRY Q10 - GRADE B 1 25 EUR TEL. BLACKBERRY Q5 - GRADE C 2 15 EUR TEL. BLACKBERRY Z10 STL100-1 - GRADE B 1 26 EUR TEL. CAT B25 - GRADE C 1 14 EUR TEL. CAT B25 - GRADE D 1 8 EUR TEL. CAT B30 - GRADE D 1 10 EUR TEL. DISCOVERY V8 - Grade B 1 30 EUR TEL. HTC DESIRE 310 (0PA2110) - GRADE B* 1 16 EUR TEL. HTC DESIRE 310 (0PA2110) - GRADE C 1 14 EUR TEL. HTC Desire 500 - GRADE B 1 16 EUR TEL. HTC G1 - GRADE A 1 20 EUR TEL. HTC HERM300 - GRADE A 1 45 EUR TEL. HTC WILDFIRE S (PG76100) - GRADE B* 1 12 EUR TEL. HTC WILDFIRE S (PG76100) - GRADE D 1 8 EUR TEL. HUAWEI ASCEND G 300 - GRADE C 1 25 EUR TEL. HUAWEI Ascend Y300 - GRADE C 1 16 EUR TEL. -

Microsoft Lumia
Microsoft Lumia 435 The Power to Never Compromise Key Features Operating System: Windows Phone 8.1 with Lumia • Always the latest generation Windows Phone 8.1 Denim experiences including Cortana*, OneDrive and Lumia 435 Office –built in and free Networks: GSM/EDGE: 850/900/1800/1900 MHz • Make memorable Skype video calls and seamlessly WCDMA: Band 1 (2100 MHz), Band 2 (1900 MHz), switch between voice and video with built-in Skype Band 5 (850 MHz), Band 8 (900 MHz) Never Compromise integration and a front facing camera. • All the apps you love – alive on the most personal Processor: Qualcomm Snapdragon 200 MSM 8210, home screen 1.2 GHz dual-core Accessories Memory: 1GB RAM, 8 GB internal mass memory + up • Comfort Headset to 128 GB MicroSD and up to 30 GB of free OneDrive • Bang by Coloud (speaker) cloud storage** • Cover for Lumia 435 / 532 (exchangeable back cover) Display: 4” WVGA LCD, capacitive multipoint-touch, 800 x 480 pixels, no Glance UI Size: 118.1/64.7/11.7 (volumetric) mm Primary Camera: 2 MP Fixed Focus, Flash: no Weight: 134.1 g Secondary Camera: VGA Colors: Connectivity: A-GPS/GLONASS, WIFI (2.4 GHz) b/g/n, Talk time and Standby time (Estimates) microUSB, BT 4.0/Micro SIM • Talk time GSM up to 20.9 hours • Talk time 3G up to 11.7 hours Sensors: Accelerometer, Ambient light sensor, Optical • Video playback up to 6.6 hours proximity sensor • Music playback up to 64 hours • Standby time up to 21 days Audio: 3.5 mm AV connector (AHJ), FM Radio, Music player Sales Package • Lumia 435 Battery: Removable 1560 mAh battery, no wireless -

Ghid Rapid Γρήγορη Έναρξη Lumia 435 Lumia 435 Dual
Ghid rapid Γρήγορη έναρξη Lumia 435 Lumia 435 Dual SIM RM-1069 9264389 RO EL RM-1071 Află mai multe... Microsoft Lumia 435 Microsoft Lumia 435 Dual SIM 9264389 Ediția 1.1 RO Tastele și componentele Important: Pentru informații importante despre utilizarea în siguranță a dispozitivului și a bateriei, citiți secțiunile „Pentru siguranța dvs.” și „Informații despre produs și siguranță” de la www.microsoft.com/mobile/support/ înainte de a începe să utilizați dispozitivul. Aceleași informații sunt disponibile pe telefon, în ghidul utilizatorului. Selectați Lumia: Ajutor+Sfaturi. 1 Receptorul 2 Conectorul audio (3,5 mm) 3 Camera foto de pe față 4 Tastele de volum 5 Tasta de pornire/oprire/blocare 6Tasta de căutare 7Microfon 8 Conectorul micro-USB 9 Tasta înapoi 10 Tasta de pornire 11 Ecranul tactil 12 Camera foto de pe spate 13 Zona antenei 14 Difuzorul Unele dintre accesoriile menționate în acest ghid al utilizatorului, cum ar fi încărcătorul, setul de căști cu microfon sau cablul de date, ar putea fi vândute separat. Evitați atingerea inutilă a zonei antenei în timp ce aceasta este în uz. Contactul cu antenele afectează calitatea comunicării și poate reduce durata de funcționare a bateriei din cauza creșterii nivelului de consum în timpul funcționării. Pregătirea pentru utilizare Înainte de a începe să utilizați telefonul, scoateți capacul din spate pentru a introduce cartelele micro-SIM (cunoscute și sub numele de cartele mini-UICC). Scoaterea capacului din spate Asigurați-vă că telefonul este oprit. 1. Țineți cu o mână telefonul de colțurile de sus și, cu degetul mare al celeilalte mâini, apăsați și scoateți capacul din spate. -

HEM Pricelist 09 MARS 2016.Pdf
04 84 255 960 / 9h30 - 19h NON STOP Webshop sur www.hemfrance.com Grille tarifaire Téléphonie, Tablettes et pièces détachées Tarifs valables à partir du 9 mars 2016 Yoni HADDAD [0972 500 626 / 06 06 64 38 67 - Mail: [email protected] - Skype: yoni.hem] Eddy MYARA [0972 500 631 / 0761 631 731 - Mail: [email protected] - Skype: eddy.hem] Hector PEREIRA (Terrain) [06 35 02 77 48 - Mail: [email protected]] Livraison 24h – Franco de Port de 600€HT, 750€ en contre remboursement. En dessous, 20€ de participation Hem France – 27 Boulevard d’Arras, 13004 Marseille – Tél : 04 84 255 960, Fax : 0972 520 592 Ice Phone Forever Samsung Galaxy J5 Alcatel 2004 Samsung a510 Galaxy A5 (2016) 39€ 149€ 32€ 305€ KONROW Information Référence Modèle Prix (€HT) CHIP2_WHI Konrow Chipo 2 Blanc 11.90 € CHIP2_BRA Konrow Chipo 2 Brasil 11.90 € CHIP2_FRE Konrow Chipo 2 French 11.90 € CHIP2_BLK Konrow Chipo 2 Noir 11.90 € CHIP2_ORA Konrow Chipo 2 Orange 11.90 € CHIP2_RED Konrow Chipo 2 Rouge 11.90 € KCF_DB Konrow Coolfive Bleu Nuit + Coque de protection 59.00 € KCF_GLD Konrow Coolfive Gold + Coque de protection 59.00 € KCF_BLK Konrow Coolfive Noir + Coque de protection 59.00 € KCF_RED Konrow Coolfive Rouge + Coque de protection 59.00 € KCF_SIL Konrow Coolfive Silver + Coque de protection 59.00 € KCS_WHI Konrow Coolsmart Blanc Nacré 49.00 € KCS_BLU Konrow Coolsmart Bleu Cyan 49.00 € KCS_GLD Konrow Coolsmart Gold 49.00 € KCS_BLK Konrow Coolsmart Noir 49.00 € KCS_ORA Konrow Coolsmart Orange 49.00 € KCS_PNK Konrow Coolsmart Rose 49.00 € KCS_RED Konrow Coolsmart Rouge -

Ceny Urządzeń Telekomunikacyjnych I Innych Towarów Na Warunkach Ogólnych (Poza Promocją)
Ceny urządzeń telekomunikacyjnych i innych towarów na warunkach ogólnych (poza promocją) Wersja z dnia 23/08/2016 r. obowiązująca do odwołania lub do wyczerpania stanów magazynowych Polkomtel sp. z o.o. Cena w zł Cena w zł Nazwa urządzenia telekomunikacyjnego/innego towaru netto brutto (Z)Sony Xperia M4 Aqua + Power Bank Sony CP-V5 817,07 zł 1 005,00 zł Apple iPhone 6 PLUS 64GB LTE 3 418,70 zł 4 205,00 zł Apple iPhone 6s 64GB LTE 3 012,20 zł 3 705,00 zł Apple iPhone SE 2 158,54 zł 2 655,00 zł HONOR 5X LTE by Huawei 898,37 zł 1 105,00 zł Honor 7 lite by Huawei 902,44 zł 1 110,00 zł HONOR 7 LTE by Huawei 1 223,58 zł 1 505,00 zł Honor 8 by Huawei 1 630,08 zł 2 005,00 zł HTC 10 LTE 2 686,99 zł 3 305,00 zł HTC Desire 530 LTE 808,94 zł 995,00 zł HTC One M9 LTE 1 926,83 zł 2 370,00 zł Huawei CarFi LTE 199,19 zł 245,00 zł Huawei Mate 8 2 036,59 zł 2 505,00 zł HUAWEI Mate S LTE 1 833,33 zł 2 255,00 zł Huawei MediaPad T1 8.0 LTE 589,43 zł 725,00 zł HUAWEI P8 Lite LTE Dual SIM 678,86 zł 835,00 zł Huawei P9 1 955,28 zł 2 405,00 zł Huawei P9 Lite 1 056,91 zł 1 300,00 zł Huawei Y3 II 386,18 zł 475,00 zł Huawei Y5 II 451,22 zł 555,00 zł HUAWEI Y5 LTE 325,20 zł 400,00 zł Huawei Y6 II LTE 691,06 zł 850,00 zł Huawei Y6 Lte 491,87 zł 605,00 zł HUAWEI Y635 LTE 369,92 zł 455,00 zł Kazam TV 4.5 394,31 zł 485,00 zł Lenovo K5 735,77 zł 905,00 zł Lenovo Moto X Force 2 280,49 zł 2 805,00 zł Lenovo Moto X Style 1 410,57 zł 1 735,00 zł Lenovo S8 - 50L 8.0 LTE 589,43 zł 725,00 zł LG G Pad 8.0 4G 589,43 zł 725,00 zł LG G4 1 711,38 zł 2 105,00 zł LG G4 dual SIM 1 711,38