RASEF Expression Correlates with Hormone Receptor Status in Breast Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chromosomal Aberrations in Head and Neck Squamous Cell Carcinomas in Norwegian and Sudanese Populations by Array Comparative Genomic Hybridization
825-843 12/9/08 15:31 Page 825 ONCOLOGY REPORTS 20: 825-843, 2008 825 Chromosomal aberrations in head and neck squamous cell carcinomas in Norwegian and Sudanese populations by array comparative genomic hybridization ERIC ROMAN1,2, LEONARDO A. MEZA-ZEPEDA3, STINE H. KRESSE3, OLA MYKLEBOST3,4, ENDRE N. VASSTRAND2 and SALAH O. IBRAHIM1,2 1Department of Biomedicine, Faculty of Medicine and Dentistry, University of Bergen, Jonas Lies vei 91; 2Department of Oral Sciences - Periodontology, Faculty of Medicine and Dentistry, University of Bergen, Årstadveien 17, 5009 Bergen; 3Department of Tumor Biology, Institute for Cancer Research, Rikshospitalet-Radiumhospitalet Medical Center, Montebello, 0310 Oslo; 4Department of Molecular Biosciences, University of Oslo, Blindernveien 31, 0371 Oslo, Norway Received January 30, 2008; Accepted April 29, 2008 DOI: 10.3892/or_00000080 Abstract. We used microarray-based comparative genomic logical parameters showed little correlation, suggesting an hybridization to explore genome-wide profiles of chromosomal occurrence of gains/losses regardless of ethnic differences and aberrations in 26 samples of head and neck cancers compared clinicopathological status between the patients from the two to their pair-wise normal controls. The samples were obtained countries. Our findings indicate the existence of common from Sudanese (n=11) and Norwegian (n=15) patients. The gene-specific amplifications/deletions in these tumors, findings were correlated with clinicopathological variables. regardless of the source of the samples or attributed We identified the amplification of 41 common chromosomal carcinogenic risk factors. regions (harboring 149 candidate genes) and the deletion of 22 (28 candidate genes). Predominant chromosomal alterations Introduction that were observed included high-level amplification at 1q21 (harboring the S100A gene family) and 11q22 (including Head and neck squamous cell carcinoma (HNSCC), including several MMP family members). -

Genomic and Transcriptome Analysis Revealing an Oncogenic Functional Module in Meningiomas
Neurosurg Focus 35 (6):E3, 2013 ©AANS, 2013 Genomic and transcriptome analysis revealing an oncogenic functional module in meningiomas XIAO CHANG, PH.D.,1 LINGLING SHI, PH.D.,2 FAN GAO, PH.D.,1 JONATHAN RUssIN, M.D.,3 LIYUN ZENG, PH.D.,1 SHUHAN HE, B.S.,3 THOMAS C. CHEN, M.D.,3 STEVEN L. GIANNOTTA, M.D.,3 DANIEL J. WEISENBERGER, PH.D.,4 GAbrIEL ZADA, M.D.,3 KAI WANG, PH.D.,1,5,6 AND WIllIAM J. MAck, M.D.1,3 1Zilkha Neurogenetic Institute, Keck School of Medicine, University of Southern California, Los Angeles, California; 2GHM Institute of CNS Regeneration, Jinan University, Guangzhou, China; 3Department of Neurosurgery, Keck School of Medicine, University of Southern California, Los Angeles, California; 4USC Epigenome Center, Keck School of Medicine, University of Southern California, Los Angeles, California; 5Department of Psychiatry, Keck School of Medicine, University of Southern California, Los Angeles, California; and 6Division of Bioinformatics, Department of Preventive Medicine, Keck School of Medicine, University of Southern California, Los Angeles, California Object. Meningiomas are among the most common primary adult brain tumors. Although typically benign, roughly 2%–5% display malignant pathological features. The key molecular pathways involved in malignant trans- formation remain to be determined. Methods. Illumina expression microarrays were used to assess gene expression levels, and Illumina single- nucleotide polymorphism arrays were used to identify copy number variants in benign, atypical, and malignant me- ningiomas (19 tumors, including 4 malignant ones). The authors also reanalyzed 2 expression data sets generated on Affymetrix microarrays (n = 68, including 6 malignant ones; n = 56, including 3 malignant ones). -
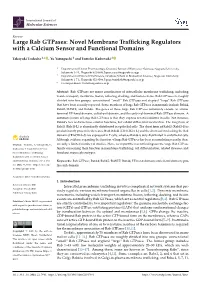
Large Rab Gtpases: Novel Membrane Trafficking Regulators with a Calcium Sensor and Functional Domains
International Journal of Molecular Sciences Review Large Rab GTPases: Novel Membrane Trafficking Regulators with a Calcium Sensor and Functional Domains Takayuki Tsukuba 1,* , Yu Yamaguchi 1 and Tomoko Kadowaki 2 1 Department of Dental Pharmacology, Graduate School of Biomedical Sciences, Nagasaki University, Sakamoto 1-7-1, Nagasaki 852-8588, Japan; [email protected] 2 Department of Frontier Oral Science, Graduate School of Biomedical Sciences, Nagasaki University, Sakamoto 1-7-1, Nagasaki 852-8588, Japan; [email protected] * Correspondence: [email protected] Abstract: Rab GTPases are major coordinators of intracellular membrane trafficking, including vesicle transport, membrane fission, tethering, docking, and fusion events. Rab GTPases are roughly divided into two groups: conventional “small” Rab GTPases and atypical “large” Rab GTPases that have been recently reported. Some members of large Rab GTPases in mammals include Rab44, Rab45/RASEF, and Rab46. The genes of these large Rab GTPases commonly encode an amino- terminal EF-hand domain, coiled-coil domain, and the carboxyl-terminal Rab GTPase domain. A common feature of large Rab GTPases is that they express several isoforms in cells. For instance, Rab44’s two isoforms have similar functions, but exhibit differential localization. The long form of Rab45 (Rab45-L) is abundantly distributed in epithelial cells. The short form of Rab45 (Rab45-S) is predominantly present in the testes. Both Rab46 (CRACR2A-L) and the short isoform lacking the Rab domain (CRACR2A-S) are expressed in T cells, whereas Rab46 is only distributed in endothelial cells. Although evidence regarding the function of large Rab GTPases has been accumulating recently, there Citation: Tsukuba, T.; Yamaguchi, Y.; are only a limited number of studies. -

Genomic Anatomy of the Tyrp1 (Brown) Deletion Complex
Genomic anatomy of the Tyrp1 (brown) deletion complex Ian M. Smyth*, Laurens Wilming†, Angela W. Lee*, Martin S. Taylor*, Phillipe Gautier*, Karen Barlow†, Justine Wallis†, Sancha Martin†, Rebecca Glithero†, Ben Phillimore†, Sarah Pelan†, Rob Andrew†, Karen Holt†, Ruth Taylor†, Stuart McLaren†, John Burton†, Jonathon Bailey†, Sarah Sims†, Jan Squares†, Bob Plumb†, Ann Joy†, Richard Gibson†, James Gilbert†, Elizabeth Hart†, Gavin Laird†, Jane Loveland†, Jonathan Mudge†, Charlie Steward†, David Swarbreck†, Jennifer Harrow†, Philip North‡, Nicholas Leaves‡, John Greystrong‡, Maria Coppola‡, Shilpa Manjunath‡, Mark Campbell‡, Mark Smith‡, Gregory Strachan‡, Calli Tofts‡, Esther Boal‡, Victoria Cobley‡, Giselle Hunter‡, Christopher Kimberley‡, Daniel Thomas‡, Lee Cave-Berry‡, Paul Weston‡, Marc R. M. Botcherby‡, Sharon White*, Ruth Edgar*, Sally H. Cross*, Marjan Irvani¶, Holger Hummerich¶, Eleanor H. Simpson*, Dabney Johnson§, Patricia R. Hunsicker§, Peter F. R. Little¶, Tim Hubbard†, R. Duncan Campbell‡, Jane Rogers†, and Ian J. Jackson*ʈ *Medical Research Council Human Genetics Unit, Edinburgh EH4 2XU, United Kingdom; †Wellcome Trust Sanger Institute, and ‡Medical Research Council Rosalind Franklin Centre for Genome Research, Hinxton CB10 1SA, United Kingdom; §Life Sciences Division, Oak Ridge National Laboratory, Oak Ridge, TN 37831; and ¶Department of Biochemistry, Imperial College, London SW7 2AZ, United Kingdom Communicated by Liane B. Russell, Oak Ridge National Laboratory, Oak Ridge, TN, January 9, 2006 (received for review September 15, 2005) Chromosome deletions in the mouse have proven invaluable in the deletions also provided the means to produce physical maps of dissection of gene function. The brown deletion complex com- genetic markers. Studies of this kind have been published for prises >28 independent genome rearrangements, which have several loci, including albino (Tyr), piebald (Ednrb), pink-eyed been used to identify several functional loci on chromosome 4 dilution (p), and the brown deletion complex (2–6). -

Identification of Expression Qtls Targeting Candidate Genes For
ISSN: 2378-3648 Salleh et al. J Genet Genome Res 2018, 5:035 DOI: 10.23937/2378-3648/1410035 Volume 5 | Issue 1 Journal of Open Access Genetics and Genome Research RESEARCH ARTICLE Identification of Expression QTLs Targeting Candidate Genes for Residual Feed Intake in Dairy Cattle Using Systems Genomics Salleh MS1,2, Mazzoni G2, Nielsen MO1, Løvendahl P3 and Kadarmideen HN2,4* 1Department of Veterinary and Animal Sciences, Faculty of Health and Medical Sciences, University of Copenhagen, Denmark Check for 2Department of Bio and Health Informatics, Technical University of Denmark, Lyngby, Denmark updates 3Department of Molecular Biology and Genetics-Center for Quantitative Genetics and Genomics, Aarhus University, AU Foulum, Tjele, Denmark 4Department of Applied Mathematics and Computer Science, Technical University of Denmark, Lyngby, Denmark *Corresponding author: Kadarmideen HN, Department of Applied Mathematics and Computer Science, Technical University of Denmark, DK-2800, Kgs. Lyngby, Denmark, E-mail: [email protected] Abstract body weight gain and net merit). The eQTLs and biological pathways identified in this study improve our understanding Background: Residual feed intake (RFI) is the difference of the complex biological and genetic mechanisms that de- between actual and predicted feed intake and an important termine FE traits in dairy cattle. The identified eQTLs/genet- factor determining feed efficiency (FE). Recently, 170 can- ic variants can potentially be used in new genomic selection didate genes were associated with RFI, but no expression methods that include biological/functional information on quantitative trait loci (eQTL) mapping has hitherto been per- SNPs. formed on FE related genes in dairy cows. In this study, an integrative systems genetics approach was applied to map Keywords eQTLs in Holstein and Jersey cows fed two different diets to eQTL, RNA-seq, Genotype, Data integration, Systems improve identification of candidate genes for FE. -

Matrix Metalloproteinases As Target Genes for Gene Regulatory Networks
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by DSpace at Belgorod State University Received: 30 November 2018 | Revised: 30 March 2019 | Accepted: 8 April 2019 DOI: 10.1002/jcb.28815 RESEARCH ARTICLE Matrix metalloproteinases as target genes for gene regulatory networks driving molecular and cellular pathways related to a multistep pathogenesis of cerebrovascular disease Alexey Polonikov1,2 | Larisa Rymarova2 | Elena Klyosova3 | Anastasia Volkova1 | Iuliia Azarova3,4 | Olga Bushueva1,5 | Marina Bykanova1,5 | Iuliia Bocharova1 | Sergey Zhabin6 | Mikhail Churnosov7 | Vitaliy Laskov8 | Maria Solodilova1 1Department of Biology, Medical Genetics and Ecology, Kursk State Medical University, Kursk, Russian Federation 2Laboratory of Statistical Genetics and Bioinformatics, Research Institute for Genetic and Molecular Epidemiology, Kursk State Medical University, Kursk, Russian Federation 3Laboratory of Biochemical Genetics and Metabolomics, Research Institute for Genetic and Molecular Epidemiology, Kursk State Medical University, Kursk, Russian Federation 4Department of Biological Chemistry, Kursk State Medical University, Kursk, Russian Federation 5Laboratory of Genomic Research, Research Institute for Genetic and Molecular Epidemiology, Kursk State Medical University, Kursk, Russian Federation 6Department of Surgical Diseases, Kursk State Medical University, Kursk, Russian Federation 7Department of Medical Biological Disciplines, Belgorod State University, Belgorod, Russian Federation 8Department of Neurology and Neurosurgery, Kursk State Medical University, Kursk, Russian Federation Correspondence Alexey Polonikov, MD, PhD, Department Abstract of Biology, Medical Genetics and Ecology, The present study investigated a joint contribution of matrix metalloproteinases Kursk State Medical University, 3 Karl (MMPs) genes to ischemic stroke (IS) development and analyzed interactions Marx St., Kursk 305041, Russian ‐ Federation. between MMP genes and genome wide associated loci for IS. -

2P5s Lichtarge Lab 2006
Pages 1–8 2p5s Evolutionary trace report by report maker May 11, 2010 4.3.1 Alistat 7 4.3.2 CE 7 4.3.3 DSSP 7 4.3.4 HSSP 7 4.3.5 LaTex 8 4.3.6 Muscle 8 4.3.7 Pymol 8 4.4 Note about ET Viewer 8 4.5 Citing this work 8 4.6 About report maker 8 4.7 Attachments 8 1 INTRODUCTION From the original Protein Data Bank entry (PDB id 2p5s): Title: Rab domain of human rasef in complex with gdp Compound: Mol id: 1; molecule: ras and ef-hand domain contai- CONTENTS ning; chain: a, b; fragment: residues 533-712; engineered: yes Organism, scientific name: Homo Sapiens; 1 Introduction 1 2p5s contains a single unique chain 2p5sA (157 residues long) and its homologue 2p5sB. 2 Chain 2p5sA 1 2.1 Q8IZ41 overview 1 2.2 Multiple sequence alignment for 2p5sA 1 2.3 Residue ranking in 2p5sA 1 2.4 Top ranking residues in 2p5sA and their position on 2 CHAIN 2P5SA the structure 1 2.1 Q8IZ41 overview 2.4.1 Clustering of residues at 25% coverage. 1 2.4.2 Overlap with known functional surfaces at From SwissProt, id Q8IZ41, 92% identical to 2p5sA: 25% coverage. 2 Description: RAS and EF hand domain containing (OTT- 2.4.3 Possible novel functional surfaces at 25% HUMP00000021538). coverage. 5 Organism, scientific name: Homo sapiens (Human). Taxonomy: Eukaryota; Metazoa; Chordata; Craniata; Vertebrata; 3 Notes on using trace results 6 Euteleostomi; Mammalia; Eutheria; Euarchontoglires; Primates; 3.1 Coverage 6 Catarrhini; Hominidae; Homo. -

P42.3 Gene Expression in Gastric Cancer Cell and Its Protein
Zhang et al. Theoretical Biology and Medical Modelling 2012, 9:53 http://www.tbiomed.com/content/9/1/53 RESEARCH Open Access p42.3 gene expression in gastric cancer cell and its protein regulatory network analysis Jianhua Zhang1†, Chunlei Lu2†, Zhigang Shang1, Rui Xing3, Li Shi1* and Youyong Lv3* * Correspondence: [email protected]; [email protected] Abstract †Equal contributors 1Department of Biomedical Background: To analyze the p42.3 gene expression in gastric cancer (GC) cell, find the Engineering, School of Electrical relationship between protein structure and function, establish the regulatory network of Engineering, Zhengzhou University, p42.3 protein molecule and then to obtain the optimal regulatory pathway. Zhengzhou, Henan Province 450001, China Methods: The expression of p42.3 gene was analyzed by RT-PCR, Western Blot and 3Laboratory of Molecular Oncology, other biotechnologies. The relationship between the spatial conformation of p42.3 Beijing Institute for Cancer Research, School of Oncology, Peking protein molecule and its function was analyzed using bioinformatics, MATLAB and University, Beijing, Hai-Dian District related knowledge about protein structure and function. Furthermore, based on 100080, China similarity algorithm of spatial layered spherical coordinate, we compared p42.3 Full list of author information is available at the end of the article molecule with several similar structured proteins which are known for the function, screened the characteristic nodes related to tumorigenesis and development, and established the multi variable relational model between p42.3 protein expression, cell cycle regulation and biological characteristics in the level of molecular regulatory networks. Finally, the optimal regulatory network was found by using Bayesian network. -

Supplementary Table 1-All DNM.Xlsx
Pathogenicity Patient ID Origin Semen analysis Gene Chromosome coordinates (GRCh37) Refseq ID HGVS Expressed in testis prediction* Proband_005 Netherlands Azoospermia CDK5RAP2 chr9:123215805 NM_018249:c.2722C>T p.Arg908Trp SP Yes, not enhanced ATP1A1 chr1:116930014 NM_000701:c.291del p.Phe97LeufsTer44 N/A Yes, not enhanced TLN2 chr15:63029134 NM_015059:c.3416G>A p.Gly1139Glu MP Yes, not enhanced Proband_006 Netherlands Azoospermia HUWE1 chrX:53589090 NM_031407:c.7314_7319del p.Glu2439_Glu2440del N/A Yes, not enhanced ABCC10 chr6:43417749 NM_001198934:c.4399C>T p.Arg1467Cys - Yes, not enhanced Proband_008 Netherlands Azoospermia CP chr3:148927135 NM_000096c.644G>A p.Arg215Gln - Not expressed FUS chr16:31196402 NM_004960:c.678_686del p.Gly229_Gly231del N/A Yes, not enhanced Proband_010 Netherlands Azoospermia LTBP1 chr2:33246090 NM_206943:c.680C>G p.Ser227Trp P Yes, not enhanced Proband_012 Netherlands Extreme oligozoospermia RP1L1 chr8:10480174 NM_178857:c.538G>A p.Ala180Thr SP Yes, not enhanced Proband_013 Netherlands Azoospermia ERG chr21:39755563 NM_182918:c.1202C>T p.Pro401Leu MP Yes, not enhanced Proband_017 Netherlands Azoospermia CDC5L chr6:44413480 NM_001253:c.2180G>A p.Arg727His SMP Yes, not enhanced Proband_019 Netherlands Azoospermia ABLIM1 chr10:116205100 NM_002313:c.1798C>T p.Arg600Trp SMP Yes, not enhanced CCDC126 chr7:23682709 NM_001253:c.2180G>A p.Thr133Met - Yes, enhanced expression in testis Proband_020 Netherlands Azoospermia RASEF chr9:85607885 NM_152573:c.1976G>A p.Arg659His SMP Yes, not enhanced Proband_022 Netherlands -
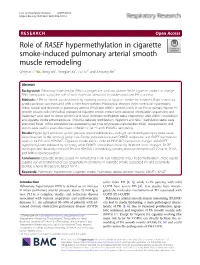
Role of RASEF Hypermethylation in Cigarette Smoke-Induced Pulmonary
Li et al. Respiratory Research (2019) 20:52 https://doi.org/10.1186/s12931-019-1014-1 RESEARCH Open Access Role of RASEF hypermethylation in cigarette smoke-induced pulmonary arterial smooth muscle remodeling Qinghai Li1,2 , Jixing Wu1, Yongjian Xu1, Lu Liu3* and Jungang Xie1* Abstract Background: Pulmonary hypertension (PH) is a progressive and fatal disease. While cigarette smoke can change DNA methylation status, the role of such molecular alterations in smoke-associated PH is unclear. Methods: A PH rat model was developed by exposing animals to cigarette smoke for 3 months. Right ventricular systolic pressure was measured with a right heart catheter. Histological changes (right ventricular hypertrophy index, medial wall thickness in pulmonary arteries (PAs)) and DNMT1 protein levels in rat PAs or primary human PA smooth muscle cells (HPASMCs) exposed to cigarette smoke extract were assessed. Methylation sequencing and MassArray® were used to detect genomic and RASEF promoter methylation status, respectively. After DNMT1 knockdown and cigarette smoke extract exposure, HPASMCs behavior (proliferation, migration) and RASEF methylation status were examined; RASEF mRNA expression was evaluated by real-time-polymerase chain reaction. RASEF overexpression viral vectors were used to assess the impact of RASEF on rat PH and HPASMCs remodeling. Results: Higher right ventricular systolic pressure, medial wall thickness, and right ventricular hypertrophy index values were observed in the smoking group rats. Smoke exposure increased DNMT1 expression and RASEF methylation levels in rat PAs and HPASMCs. Cigarette smoke extract induced HPASMCs behavioral changes and RASEF hypermethylation followed by silencing, while DNMT1 knockdown markedly inhibited these changes. RASEF overexpression distinctly inhibited PH and HPASMCs remodeling, possibly through phospho-AKT (Ser473), PCNA, and MMP9 downregulation. -

Supplementary Materials
Supplementary Materials 1 Supplementary Figure S1. Expression of BPIFB4 in murine hearts. Representative immunohistochemistry images showing the expression of BPIFB4 in the left ventricle of non-diabetic mice (ND) and diabetic mice (Diab) given vehicle or LAV-BPIFB4. BPIFB4 is shown in green, nuclei are identified by the blue fluorescence of DAPI. Scale bars: 1 mm and 100 μm. 2 Supplementary Table S1 – List of PCR primers. Target gene Primer Sequence NCBI Accession number / Reference Forward AAGTCCCTCACCCTCCCAA Actb [1] Reverse AAGCAATGCTGTCACCTTC Forward TCTAGGCAATGCCGTTCAC Cpt1b [2] Reverse GAGCACATGGGCACCATAC Forward GGAAATGATCAACAAAAAAAGAAGTATTT Acadm (Mcad) [2] Reverse GCCGCCACATCAGA Forward TGATGGTTTGGAGGTTGGGG Acot1 NM_012006.2 Reverse TGAAACTCCATTCCCAGCCC Forward GGTGTCCCGTCTAATGGAGA Hmgcs2 NM_008256.4 Reverse ACACCCAGGATTCACAGAGG Forward CAAGCAGCAACATGGGAAGA Cs [2] Reverse GTCAGGATCAAGAACCGAAGTCT Forward GCCATTGTCAACTGTGCTGA Ucp3 NM_009464.3 Reverse TCCTGAGCCACCATCTTCAG Forward CGTGAGGGCAATGATTTATACCAT Atp5b [2] Reverse TCCTGGTCTCTGAAGTATTCAGCAA Pdk4 Forward CCGCTGTCCATGAAGCA [2] 3 Reverse GCAGAAAAGCAAAGGACGTT Forward AGAGTCCTATGCAGCCCAGA Tomm20 NM_024214.2 Reverse CAAAGCCCCACATCTGTCCT Forward GCCTCAGATCGTCGTAGTGG Drp1 NM_152816.3 Reverse TTCCATGTGGCAGGGTCATT Forward GGGAAGGTGAAGAAGCTTGGA Mfn2 NM_001285920.1 Reverse ACAACTGGAACAGAGGAGAAGTT Forward CGGAAATCATATCCAACCAG [2] Ppargc1a (Pgc1α) Reverse TGAGAACCGCTAGCAAGTTTG Forward AGGCTTGGAAAAATCTGTCTC [2] Tfam Reverse TGCTCTTCCCAAGACTTCATT Forward TGCCCCAGAGCTGTTAATGA Bcl2l1 NM_001289716.1 -

Molecular Genetic Studies of Recessively Inherited Eye Diseases
MOLECULAR GENETIC STUDIES OF RECESSIVELY INHERITED EYE DISEASES by SARAH JOYCE A thesis submitted to The University of Birmingham for the degree of DOCTOR OF PHILOSOPHY School of Clinical and Experimental Medicine The Medical School University of Birmingham July 2011 University of Birmingham Research Archive e-theses repository This unpublished thesis/dissertation is copyright of the author and/or third parties. The intellectual property rights of the author or third parties in respect of this work are as defined by The Copyright Designs and Patents Act 1988 or as modified by any successor legislation. Any use made of information contained in this thesis/dissertation must be in accordance with that legislation and must be properly acknowledged. Further distribution or reproduction in any format is prohibited without the permission of the copyright holder. Abstract Cataract is the opacification of the crystalline lens of the eye. Both childhood and later-onset cataracts have been linked with complex genetic factors. Cataracts vary in phenotype and exhibit genetic heterogeneity. They can appear as isolated abnormalities, or as part of a syndrome. During this project, analysis of syndromic and non-syndromic cataract families using genetic linkage studies was undertaken in order to identify the genes involved, using an autozygosity mapping and positional candidate approach. Causative mutations were identified in families with syndromes involving cataracts. The finding of a mutation in CYP27A1 in a family with Cerebrotendinous Xanthomatosis permitted clinical intervention as this is a treatable disorder. A mutation that segregated with disease status in a family with Marinesco Sjogren Syndrome was identified in SIL1. In a family with Knobloch Syndrome, a frameshift mutation in COL18A1 was detected in all affected individuals.