The Pharyngo- Esophageal Segment (PES)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Earthworm Dissection External Anatomy Examine Your Earthworm and Determine the Dorsal and Ventral Sides
Name(s): ___________________________________________Date:________ Earthworm Dissection External Anatomy Examine your earthworm and determine the dorsal and ventral sides. Locate the two openings on the ventral surface of the earthworm. Locate the openings toward the anterior of the worm which are the s perm ducts. Locate the openings near the clitellum which are the g enital setae . Locate the dark line that runs down the dorsal side of the worm, this is the dorsal blood vessel. The ventral blood vessel can be seen on the underside of the worm, though it is usually not as dark . Locate the worm’s anus on the far posterior end of the worm. Note the swelling of the earthworm near its anterior side - this is the clitellum. Label the earthworm pictured. A_____________________________ B _____________________________ C _____________________________ D _____________________________ Internal Anatomy 1. Place the specimen in the dissecting pan D ORSAL side up. 2. Locate the clitellum and insert the tip of the scissors about 3 cm posterior. 3. Cut carefully all the way up to the head. Try to keep the scissors pointed up, and only cut through the skin. 4. Spread the skin of the worm out, use a teasing needle to gently tear the s epta (little thread like structures that hold the skin to organs below it) 5. Place pins in the skin to hold it apart – set them at an angle so they aren’t in the way of your view. Reproductive System The first structures you probably see are the s eminal vesicles. They are cream colored and located toward the anterior of the worm. -

Programa De Pós-Graduação Em Ecologia Fluxo De
INSTITUTO NACIONAL DE PESQUISAS DA AMAZÔNIA - INPA PROGRAMA DE PÓS-GRADUAÇÃO EM ECOLOGIA FLUXO DE ENERGIA EM TEIAS ALIMENTARES DE ECOSSISTEMAS AQUÁTICOS TROPICAIS: DAS FONTES AUTOTRÓFICAS ATÉ OS GRANDES CONSUMIDORES ECTOTÉRMICOS FRANCISCO VILLAMARÍN Manaus, Amazonas i Agosto, 2016 Page i FRANCISCO VILLAMARÍN FLUXO DE ENERGIA EM TEIAS ALIMENTARES DE ECOSSISTEMAS AQUÁTICOS TROPICAIS: DAS FONTES AUTOTRÓFICAS ATÉ OS GRANDES CONSUMIDORES ECTOTÉRMICOS Orientador: WILLIAM E. MAGNUSSON Tese apresentada ao Instituto Nacional de Pesquisas da Amazônia como parte dos requisitos para obtenção do titulo de Doutor em BIOLOGIA-ECOLOGIA Manaus, Amazonas ii Agosto, 2016 Page ii V715 Villamarín, Francisco Fluxo de energia em teias alimentares de ecossistemas aquáticos tropicais: das fontes autotróficas até os grandes consumidores ectotérmicos / Francisco Villamarín. --- Manaus: [s.n.], 2016. 87 f.: il Tese (Doutorado) --- INPA, Manaus, 2016. Orientador: William E. Magnusson Área de concentração: Ecologia 1. Ecossistema aquático. 2. Teia alimentar. 3. Ecologia. I. Título. CDD 574.52632 iii Page iii Sinopse: Estudou-se o fluxo de energia em teias alimentares de ecossistemas aquáticos tropicais do Território Norte da Austrália e da Amazônia central. Aspectos como alocação de energia para reprodução em um peixe herbívoro-detritívoro e origens da energia e posição trófica de crocodilianos amazônicos foram avaliados. Palavras chave: isótopos estáveis, RNA:DNA, energia, consumidores ectotérmicos iv Page iv Dedicatória Mis abuelas Cecilia y Aída me enseñaron con cariño la importancia de la simplicidad y perseverancia en la vida. A ellas, dedico v Page v Agradecimentos O presente trabalho não seria possível sem o incentivo de todas as pessoas que acreditaram e que, de muitas maneiras, contribuiram sempre para que essa pesquisa seja realizada ao longo de todo esse tempo de Amazônia. -

6. the Pharynx the Pharynx, Which Forms the Upper Part of the Digestive Tract, Consists of Three Parts: the Nasopharynx, the Oropharynx and the Laryngopharynx
6. The Pharynx The pharynx, which forms the upper part of the digestive tract, consists of three parts: the nasopharynx, the oropharynx and the laryngopharynx. The principle object of this dissection is to observe the pharyngeal constrictors that form the back wall of the vocal tract. Because the cadaver is lying face down, we will consider these muscles from the back. Figure 6.1 shows their location. stylopharyngeus suuperior phayngeal constrictor mandible medial hyoid bone phayngeal constrictor inferior phayngeal constrictor Figure 6.1. Posterior view of the muscles of the pharynx. Each of the three pharyngeal constrictors has a left and right part that interdigitate (join in fingerlike branches) in the midline, forming a raphe, or union. This raphe forms the back wall of the pharynx. The superior pharyngeal constrictor is largely in the nasopharynx. It has several origins (some texts regard it as more than one muscle) one of which is the medial pterygoid plate. It assists in the constriction of the nasopharynx, but has little role in speech production other than helping form a site against which the velum may be pulled when forming a velic closure. The medial pharyngeal constrictor, which originates on the greater horn of the hyoid bone, also has little function in speech. To some extent it can be considered as an elevator of the hyoid bone, but its most important role for speech is simply as the back wall of the vocal tract. The inferior pharyngeal constrictor also performs this function, but plays a more important role constricting the pharynx in the formation of pharyngeal consonants. -

The Annual Compendium of Commercial Space Transportation: 2017
Federal Aviation Administration The Annual Compendium of Commercial Space Transportation: 2017 January 2017 Annual Compendium of Commercial Space Transportation: 2017 i Contents About the FAA Office of Commercial Space Transportation The Federal Aviation Administration’s Office of Commercial Space Transportation (FAA AST) licenses and regulates U.S. commercial space launch and reentry activity, as well as the operation of non-federal launch and reentry sites, as authorized by Executive Order 12465 and Title 51 United States Code, Subtitle V, Chapter 509 (formerly the Commercial Space Launch Act). FAA AST’s mission is to ensure public health and safety and the safety of property while protecting the national security and foreign policy interests of the United States during commercial launch and reentry operations. In addition, FAA AST is directed to encourage, facilitate, and promote commercial space launches and reentries. Additional information concerning commercial space transportation can be found on FAA AST’s website: http://www.faa.gov/go/ast Cover art: Phil Smith, The Tauri Group (2017) Publication produced for FAA AST by The Tauri Group under contract. NOTICE Use of trade names or names of manufacturers in this document does not constitute an official endorsement of such products or manufacturers, either expressed or implied, by the Federal Aviation Administration. ii Annual Compendium of Commercial Space Transportation: 2017 GENERAL CONTENTS Executive Summary 1 Introduction 5 Launch Vehicles 9 Launch and Reentry Sites 21 Payloads 35 2016 Launch Events 39 2017 Annual Commercial Space Transportation Forecast 45 Space Transportation Law and Policy 83 Appendices 89 Orbital Launch Vehicle Fact Sheets 100 iii Contents DETAILED CONTENTS EXECUTIVE SUMMARY . -

Macrophage Density in Pharyngeal and Laryngeal Muscles Greatly Exceeds That in Other Striated Muscles: an Immunohistochemical Study Using Elderly Human Cadavers
Original Article http://dx.doi.org/10.5115/acb.2016.49.3.177 pISSN 2093-3665 eISSN 2093-3673 Macrophage density in pharyngeal and laryngeal muscles greatly exceeds that in other striated muscles: an immunohistochemical study using elderly human cadavers Sunki Rhee1, Masahito Yamamoto1, Kei Kitamura1, Kasahara Masaaki1, Yukio Katori2, Gen Murakami3, Shin-ichi Abe1 1Department of Anatomy, Tokyo Dental College, Tokyo, 2Department of Otorhinolaryngology, Tohoku University School of Medicine, Sendai, 3Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan Abstract: Macrophages play an important role in aging-related muscle atrophy (i.e., sarcopenia). We examined macrophage density in six striated muscles (cricopharyngeus muscle, posterior cricoarytenoideus muscle, genioglossus muscle, masseter muscle, infraspinatus muscle, and external anal sphincter). We examined 14 donated male cadavers and utilized CD68 immunohistochemistry to clarify macrophage density in muscles. The numbers of macrophages per striated muscle fiber in the larynx and pharynx (0.34 and 0.31) were 5–6 times greater than those in the tongue, shoulder, and anus (0.05–0.07) with high statistical significance. Thick muscle fibers over 80 μm in diameter were seen in the pharynx, larynx, and anal sphincter of two limited specimens. Conversely, in the other sites or specimens, muscle fibers were thinner than 50 μm. We did not find any multinuclear muscle cells suggestive of regeneration. At the beginning of the study, we suspected that mucosal macrophages might have invaded into the muscle layer of the larynx and pharynx, but we found no evidence of inflammation in the mucosa. Likewise, the internal anal sphincter (a smooth muscle layer near the mucosa) usually contained fewer macrophages than the external sphincter. -

Abstract Volume
T I I II I II I I I rl I Abstract Volume LPI LPI Contribution No. 1097 II I II III I • • WORKSHOP ON MERCURY: SPACE ENVIRONMENT, SURFACE, AND INTERIOR The Field Museum Chicago, Illinois October 4-5, 2001 Conveners Mark Robinbson, Northwestern University G. Jeffrey Taylor, University of Hawai'i Sponsored by Lunar and Planetary Institute The Field Museum National Aeronautics and Space Administration Lunar and Planetary Institute 3600 Bay Area Boulevard Houston TX 77058-1113 LPI Contribution No. 1097 Compiled in 2001 by LUNAR AND PLANETARY INSTITUTE The Institute is operated by the Universities Space Research Association under Contract No. NASW-4574 with the National Aeronautics and Space Administration. Material in this volume may be copied without restraint for library, abstract service, education, or personal research purposes; however, republication of any paper or portion thereof requires the written permission of the authors as well as the appropriate acknowledgment of this publication .... This volume may be cited as Author A. B. (2001)Title of abstract. In Workshop on Mercury: Space Environment, Surface, and Interior, p. xx. LPI Contribution No. 1097, Lunar and Planetary Institute, Houston. This report is distributed by ORDER DEPARTMENT Lunar and Planetary institute 3600 Bay Area Boulevard Houston TX 77058-1113, USA Phone: 281-486-2172 Fax: 281-486-2186 E-mail: order@lpi:usra.edu Please contact the Order Department for ordering information, i,-J_,.,,,-_r ,_,,,,.r pA<.><--.,// ,: Mercury Workshop 2001 iii / jaO/ Preface This volume contains abstracts that have been accepted for presentation at the Workshop on Mercury: Space Environment, Surface, and Interior, October 4-5, 2001. -

View Relevant for Our Research
DEVELOPMENT AND EVALUATION OF CLICKER METHODOLOGY FOR INTRODUCTORY PHYSICS COURSES DISSERTATION Presented in Partial Fulfillment of the Requirements for the Degree Doctor of Philosophy in the Graduate School of The Ohio State University By Albert H. Lee, B.S. ***** The Ohio State University 2009 Dissertation Committee: Approved by Professor Lei Bao, Adviser Professor Neville W. Reay, Co-Adviser _______________________ Professor Andrew F. Heckler Adviser Physics Graduate Program Professor Bruce R. Patton Professor Evan R. Sugarbaker Copyright by Albert H. Lee 2009 ABSTRACT Many educators understand that lectures are cost effective but not learning efficient, so continue to search for ways to increase active student participation in this traditionally passive learning environment. In-class polling systems, or “clickers”, are inexpensive and reliable tools allowing students to actively participate in lectures by answering multiple-choice questions. Students assess their learning in real time by observing instant polling summaries displayed in front of them. This in turn motivates additional discussions which increase the opportunity for active learning. We wanted to develop a comprehensive clicker methodology that creates an active lecture environment for a broad spectrum of students taking introductory physics courses. We wanted our methodology to incorporate many findings of contemporary learning science. It is recognized that learning requires active construction; students need to be actively involved in their own learning process. Learning also depends on preexisting knowledge; students construct new knowledge and understandings based on what they already know and believe. Learning is context dependent; students who have learned to apply a concept in one context may not be able to recognize and apply the same concept in a different context, even when both contexts are considered to be isomorphic by experts. -

Small Launchers in a Pandemic World - 2021 Edition of the Annual Industry Survey
SSC21- IV-07 Small Launchers in a Pandemic World - 2021 Edition of the Annual Industry Survey Carlos Niederstrasser Northrop Grumman Corporation 45101 Warp Drive, Dulles, VA 20166 USA; +1.703.406.5504 [email protected] ABSTRACT Even with the challenges posed by the world-wide COVID pandemic, small vehicle "Launch Fever" has not abated. In 2015 we first presented this survey at the AIAA/USU Conference on Small Satellites1, and we identified twenty small launch vehicles under development. By mid-2021 ten vehicles in this class were operational, 48 were identified under development, and a staggering 43 more were potential new entrants. Some are spurred by renewed government investment in space, such as what we see in the U.K. Others are new commercial entries from unexpected markets such as China. All are inspired by the success of SpaceX and the desire to capitalize on the perceived demand caused by the mega constellations. In this paper we present an overview of the small launch vehicles under development today. When available, we compare their capabilities, stated mission goals, cost and funding sources, and their publicized testing progress. We also review the growing number of entrants that have dropped out since we first started this report. Despite the COVID-19 pandemic, one system became operational in the past 12 months and two or three more systems hope to achieve their first successful launch in 2021. There is evidence that this could be the year when the small launch market finally becomes saturated; however, expectations continue to be high and many new entrants hope that there is room for more providers. -

Neural Control of Swallowing
AG-2018-48 REVIEW dx.doi.org/10.1590/S0004-2803.201800000-45 Neural control of swallowing Milton Melciades Barbosa COSTA Received 11/4/2018 Accepted 9/5/2018 ABSTRACT – Background – Swallowing is a motor process with several discordances and a very difficult neurophysiological study. Maybe that is the reason for the scarcity of papers about it. Objective – It is to describe the chewing neural control and oral bolus qualification. A review the cranial nerves involved with swallowing and their relationship with the brainstem, cerebellum, base nuclei and cortex was made. Methods – From the reviewed literature including personal researches and new observations, a consistent and necessary revision of concepts was made, not rarely conflicting. Re- sults and Conclusion – Five different possibilities of the swallowing oral phase are described: nutritional voluntary, primary cortical, semiautomatic, subsequent gulps, and spontaneous. In relation to the neural control of the swallowing pharyngeal phase, the stimulus that triggers the pharyngeal phase is not the pharyngeal contact produced by the bolus passage, but the pharyngeal pressure distension, with or without contents. In nutritional swallowing, food and pressure are transferred, but in the primary cortical oral phase, only pressure is transferred, and the pharyngeal response is similar. The pharyngeal phase incorporates, as its functional part, the oral phase dynamics already in course. The pharyngeal phase starts by action of the pharyngeal plexus, composed of the glossopharyngeal (IX), vagus (X) and accessory (XI) nerves, with involvement of the trigeminal (V), facial (VII), glossopharyngeal (IX) and the hypoglossal (XII) nerves. The cervical plexus (C1, C2) and the hypoglossal nerve on each side form the ansa cervicalis, from where a pathway of cervical origin goes to the geniohyoid muscle, which acts in the elevation of the hyoid-laryngeal complex. -

An Hourglass Circuit Motif Transforms a Motor Program Via Subcellularly Localized Muscle Calcium Signaling and Contraction
RESEARCH ARTICLE An hourglass circuit motif transforms a motor program via subcellularly localized muscle calcium signaling and contraction Steven R Sando1, Nikhil Bhatla1,2,3, Eugene LQ Lee1,3, H Robert Horvitz1* 1Howard Hughes Medical Institute, Department of Biology, McGovern Institute for Brain Research, Massachusetts Institute of Technology, Cambridge, United States; 2Miller Institute, Helen Wills Neuroscience Institute, Department of Molecular and Cellular Biology, University of California, Berkeley, Berkeley, United States; 3Department of Brain and Cognitive Sciences, Massachusetts Institute of Technology, Cambridge, United States Abstract Neural control of muscle function is fundamental to animal behavior. Many muscles can generate multiple distinct behaviors. Nonetheless, individual muscle cells are generally regarded as the smallest units of motor control. We report that muscle cells can alter behavior by contracting subcellularly. We previously discovered that noxious tastes reverse the net flow of particles through the C. elegans pharynx, a neuromuscular pump, resulting in spitting. We now show that spitting results from the subcellular contraction of the anterior region of the pm3 muscle cell. Subcellularly localized calcium increases accompany this contraction. Spitting is controlled by an ‘hourglass’ circuit motif: parallel neural pathways converge onto a single motor neuron that differentially controls multiple muscles and the critical subcellular muscle compartment. We conclude that subcellular muscle units enable modulatory motor control and propose that subcellular muscle contraction is a fundamental mechanism by which neurons can reshape behavior. *For correspondence: [email protected] Competing interests: The Introduction authors declare that no How animal nervous systems differentially control muscle contractions to generate the variety of flex- competing interests exist. ible, context-appropriate behaviors necessary for survival and reproduction is a fundamental prob- Funding: See page 29 lem in neuroscience. -
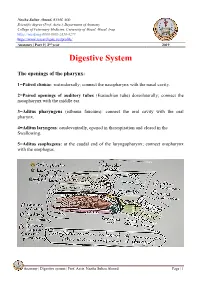
Digestive System
Naziha Sultan Ahmed, BVMS, MSc Scientific degree (Prof. Assis.), Department of Anatomy College of Veterinary Medicine, University of Mosul, Mosul, Iraq https://orcid.org/0000-0002-2856-8277 https://www.researchgate.net/profile/ Anatomy | Part 9 | 2nd year 2019 Digestive System The openings of the pharynx: 1=Paired chonae: rostrodorsally; connect the nasopharynx with the nasal cavity. 2=Paired openings of auditory tubes (Eustachian tube) dorsolaterally; connect the nasopharynx with the middle ear. 3=Aditus pharyngeus (isthmus faucium): connect the oral cavity with the oral pharynx. 4=Aditus laryngeus: caudoventrally, opened in therespiration and closed in the Swallowing. 5=Aditus esophageus: at the caudal end of the laryngopharynx; connect oropharynx with the esophagus. CouAnatomy | Digestive system | Prof. Assis. Naziha Sultan Ahmed Page | 1 Muscles of the pharynx: Pharyngeal muscles are striated, bilateral muscles, their function under the swallowing reflex. The constrictor muscles of the pharynx are: 1-Pterygopharyngeus muscle: originate from pterygoid bone, its fibers are longitudinal assist in shortening the pharynx .It inserts in pharyngeal raphe. 2-Palatopharyngeus muscle: lie immediately under the mucosa, act as sphincter for the nasopharynx and intrapharyngeal opening. It originates from the palatine aponeurosis and inserts in the pharyngeal raphe, act to shorten the pharynx. 3-Stylopharyngeus rostralis: originates from the rostral border of the ventral half of the stylohyoid bone and epihyoid and inserts in the pharyngeal raphe. 4-Hyopharyngeus muscle: originates from thyrohyoid and keratohyoid and inserts in the pharyngeal raphe. 5-Thyropharyngeus muscle: originates from the oblique line of thyroid cartilage of the larynx and inserts in the pharyngeal raphe. 6-Cricopharyngeus muscle: originates from the cricoid cartilage and inserts in the pharyngeal raphe. -

The Mouth the Mouth Extends from the Lips to the Oropharyngeal Isthmus, That Is, the Junction of the Mouth with the Pharynx
The Mouth The mouth extends from the lips to the oropharyngeal isthmus, that is, the junction of the mouth with the pharynx. It is subdivided into the vestibule, which lies between the lips and cheek externally and the gums and teeth internally, and the mouth cavity proper, which lies within the alveolar arches, gums, and teeth. The vestibule is a slitlike space that communicates with the exterior through the oral fissures. When the jaws are closed, it communicates with the mouth cavity proper behind the third molar tooth on each side. Superiorly and inferiorly, the vestibule is limited by the reflection of the mucous membrane from the lips and cheeks onto the gums. The cheek forms the lateral wall of the vestibule and is made up of the buccinator muscle, which is covered on the outside by fascia and skin and is lined by mucous membrane. Opposite the upper second molar teeth, a small papilla is present on the mucous membrane, marking the opening of the duct of the parotid salivary gland. The mouth proper has a roof, which is formed by the hard palate in front and the soft palate behind. The floor is formed by the anterior two-thirds of the tongue and by the reflection of the mucous membrane from the sides of the tongue to the gum on the mandible. In the midline, a fold of mucous membrane called frenulum of the tongue connects the undersurface of the tongue to the floor of the mouth. On each side of the frenulum is a small papilla, on the summit of which is the orifice of the duct of the submandibular salivary gland.