Movements of Gi Tract
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Earthworm Dissection External Anatomy Examine Your Earthworm and Determine the Dorsal and Ventral Sides
Name(s): ___________________________________________Date:________ Earthworm Dissection External Anatomy Examine your earthworm and determine the dorsal and ventral sides. Locate the two openings on the ventral surface of the earthworm. Locate the openings toward the anterior of the worm which are the s perm ducts. Locate the openings near the clitellum which are the g enital setae . Locate the dark line that runs down the dorsal side of the worm, this is the dorsal blood vessel. The ventral blood vessel can be seen on the underside of the worm, though it is usually not as dark . Locate the worm’s anus on the far posterior end of the worm. Note the swelling of the earthworm near its anterior side - this is the clitellum. Label the earthworm pictured. A_____________________________ B _____________________________ C _____________________________ D _____________________________ Internal Anatomy 1. Place the specimen in the dissecting pan D ORSAL side up. 2. Locate the clitellum and insert the tip of the scissors about 3 cm posterior. 3. Cut carefully all the way up to the head. Try to keep the scissors pointed up, and only cut through the skin. 4. Spread the skin of the worm out, use a teasing needle to gently tear the s epta (little thread like structures that hold the skin to organs below it) 5. Place pins in the skin to hold it apart – set them at an angle so they aren’t in the way of your view. Reproductive System The first structures you probably see are the s eminal vesicles. They are cream colored and located toward the anterior of the worm. -

6. the Pharynx the Pharynx, Which Forms the Upper Part of the Digestive Tract, Consists of Three Parts: the Nasopharynx, the Oropharynx and the Laryngopharynx
6. The Pharynx The pharynx, which forms the upper part of the digestive tract, consists of three parts: the nasopharynx, the oropharynx and the laryngopharynx. The principle object of this dissection is to observe the pharyngeal constrictors that form the back wall of the vocal tract. Because the cadaver is lying face down, we will consider these muscles from the back. Figure 6.1 shows their location. stylopharyngeus suuperior phayngeal constrictor mandible medial hyoid bone phayngeal constrictor inferior phayngeal constrictor Figure 6.1. Posterior view of the muscles of the pharynx. Each of the three pharyngeal constrictors has a left and right part that interdigitate (join in fingerlike branches) in the midline, forming a raphe, or union. This raphe forms the back wall of the pharynx. The superior pharyngeal constrictor is largely in the nasopharynx. It has several origins (some texts regard it as more than one muscle) one of which is the medial pterygoid plate. It assists in the constriction of the nasopharynx, but has little role in speech production other than helping form a site against which the velum may be pulled when forming a velic closure. The medial pharyngeal constrictor, which originates on the greater horn of the hyoid bone, also has little function in speech. To some extent it can be considered as an elevator of the hyoid bone, but its most important role for speech is simply as the back wall of the vocal tract. The inferior pharyngeal constrictor also performs this function, but plays a more important role constricting the pharynx in the formation of pharyngeal consonants. -

Macrophage Density in Pharyngeal and Laryngeal Muscles Greatly Exceeds That in Other Striated Muscles: an Immunohistochemical Study Using Elderly Human Cadavers
Original Article http://dx.doi.org/10.5115/acb.2016.49.3.177 pISSN 2093-3665 eISSN 2093-3673 Macrophage density in pharyngeal and laryngeal muscles greatly exceeds that in other striated muscles: an immunohistochemical study using elderly human cadavers Sunki Rhee1, Masahito Yamamoto1, Kei Kitamura1, Kasahara Masaaki1, Yukio Katori2, Gen Murakami3, Shin-ichi Abe1 1Department of Anatomy, Tokyo Dental College, Tokyo, 2Department of Otorhinolaryngology, Tohoku University School of Medicine, Sendai, 3Division of Internal Medicine, Iwamizawa Asuka Hospital, Iwamizawa, Japan Abstract: Macrophages play an important role in aging-related muscle atrophy (i.e., sarcopenia). We examined macrophage density in six striated muscles (cricopharyngeus muscle, posterior cricoarytenoideus muscle, genioglossus muscle, masseter muscle, infraspinatus muscle, and external anal sphincter). We examined 14 donated male cadavers and utilized CD68 immunohistochemistry to clarify macrophage density in muscles. The numbers of macrophages per striated muscle fiber in the larynx and pharynx (0.34 and 0.31) were 5–6 times greater than those in the tongue, shoulder, and anus (0.05–0.07) with high statistical significance. Thick muscle fibers over 80 μm in diameter were seen in the pharynx, larynx, and anal sphincter of two limited specimens. Conversely, in the other sites or specimens, muscle fibers were thinner than 50 μm. We did not find any multinuclear muscle cells suggestive of regeneration. At the beginning of the study, we suspected that mucosal macrophages might have invaded into the muscle layer of the larynx and pharynx, but we found no evidence of inflammation in the mucosa. Likewise, the internal anal sphincter (a smooth muscle layer near the mucosa) usually contained fewer macrophages than the external sphincter. -

Neural Control of Swallowing
AG-2018-48 REVIEW dx.doi.org/10.1590/S0004-2803.201800000-45 Neural control of swallowing Milton Melciades Barbosa COSTA Received 11/4/2018 Accepted 9/5/2018 ABSTRACT – Background – Swallowing is a motor process with several discordances and a very difficult neurophysiological study. Maybe that is the reason for the scarcity of papers about it. Objective – It is to describe the chewing neural control and oral bolus qualification. A review the cranial nerves involved with swallowing and their relationship with the brainstem, cerebellum, base nuclei and cortex was made. Methods – From the reviewed literature including personal researches and new observations, a consistent and necessary revision of concepts was made, not rarely conflicting. Re- sults and Conclusion – Five different possibilities of the swallowing oral phase are described: nutritional voluntary, primary cortical, semiautomatic, subsequent gulps, and spontaneous. In relation to the neural control of the swallowing pharyngeal phase, the stimulus that triggers the pharyngeal phase is not the pharyngeal contact produced by the bolus passage, but the pharyngeal pressure distension, with or without contents. In nutritional swallowing, food and pressure are transferred, but in the primary cortical oral phase, only pressure is transferred, and the pharyngeal response is similar. The pharyngeal phase incorporates, as its functional part, the oral phase dynamics already in course. The pharyngeal phase starts by action of the pharyngeal plexus, composed of the glossopharyngeal (IX), vagus (X) and accessory (XI) nerves, with involvement of the trigeminal (V), facial (VII), glossopharyngeal (IX) and the hypoglossal (XII) nerves. The cervical plexus (C1, C2) and the hypoglossal nerve on each side form the ansa cervicalis, from where a pathway of cervical origin goes to the geniohyoid muscle, which acts in the elevation of the hyoid-laryngeal complex. -

An Hourglass Circuit Motif Transforms a Motor Program Via Subcellularly Localized Muscle Calcium Signaling and Contraction
RESEARCH ARTICLE An hourglass circuit motif transforms a motor program via subcellularly localized muscle calcium signaling and contraction Steven R Sando1, Nikhil Bhatla1,2,3, Eugene LQ Lee1,3, H Robert Horvitz1* 1Howard Hughes Medical Institute, Department of Biology, McGovern Institute for Brain Research, Massachusetts Institute of Technology, Cambridge, United States; 2Miller Institute, Helen Wills Neuroscience Institute, Department of Molecular and Cellular Biology, University of California, Berkeley, Berkeley, United States; 3Department of Brain and Cognitive Sciences, Massachusetts Institute of Technology, Cambridge, United States Abstract Neural control of muscle function is fundamental to animal behavior. Many muscles can generate multiple distinct behaviors. Nonetheless, individual muscle cells are generally regarded as the smallest units of motor control. We report that muscle cells can alter behavior by contracting subcellularly. We previously discovered that noxious tastes reverse the net flow of particles through the C. elegans pharynx, a neuromuscular pump, resulting in spitting. We now show that spitting results from the subcellular contraction of the anterior region of the pm3 muscle cell. Subcellularly localized calcium increases accompany this contraction. Spitting is controlled by an ‘hourglass’ circuit motif: parallel neural pathways converge onto a single motor neuron that differentially controls multiple muscles and the critical subcellular muscle compartment. We conclude that subcellular muscle units enable modulatory motor control and propose that subcellular muscle contraction is a fundamental mechanism by which neurons can reshape behavior. *For correspondence: [email protected] Competing interests: The Introduction authors declare that no How animal nervous systems differentially control muscle contractions to generate the variety of flex- competing interests exist. ible, context-appropriate behaviors necessary for survival and reproduction is a fundamental prob- Funding: See page 29 lem in neuroscience. -
Digestive System
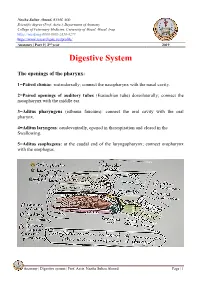
Naziha Sultan Ahmed, BVMS, MSc Scientific degree (Prof. Assis.), Department of Anatomy College of Veterinary Medicine, University of Mosul, Mosul, Iraq https://orcid.org/0000-0002-2856-8277 https://www.researchgate.net/profile/ Anatomy | Part 9 | 2nd year 2019 Digestive System The openings of the pharynx: 1=Paired chonae: rostrodorsally; connect the nasopharynx with the nasal cavity. 2=Paired openings of auditory tubes (Eustachian tube) dorsolaterally; connect the nasopharynx with the middle ear. 3=Aditus pharyngeus (isthmus faucium): connect the oral cavity with the oral pharynx. 4=Aditus laryngeus: caudoventrally, opened in therespiration and closed in the Swallowing. 5=Aditus esophageus: at the caudal end of the laryngopharynx; connect oropharynx with the esophagus. CouAnatomy | Digestive system | Prof. Assis. Naziha Sultan Ahmed Page | 1 Muscles of the pharynx: Pharyngeal muscles are striated, bilateral muscles, their function under the swallowing reflex. The constrictor muscles of the pharynx are: 1-Pterygopharyngeus muscle: originate from pterygoid bone, its fibers are longitudinal assist in shortening the pharynx .It inserts in pharyngeal raphe. 2-Palatopharyngeus muscle: lie immediately under the mucosa, act as sphincter for the nasopharynx and intrapharyngeal opening. It originates from the palatine aponeurosis and inserts in the pharyngeal raphe, act to shorten the pharynx. 3-Stylopharyngeus rostralis: originates from the rostral border of the ventral half of the stylohyoid bone and epihyoid and inserts in the pharyngeal raphe. 4-Hyopharyngeus muscle: originates from thyrohyoid and keratohyoid and inserts in the pharyngeal raphe. 5-Thyropharyngeus muscle: originates from the oblique line of thyroid cartilage of the larynx and inserts in the pharyngeal raphe. 6-Cricopharyngeus muscle: originates from the cricoid cartilage and inserts in the pharyngeal raphe. -

The Mouth the Mouth Extends from the Lips to the Oropharyngeal Isthmus, That Is, the Junction of the Mouth with the Pharynx
The Mouth The mouth extends from the lips to the oropharyngeal isthmus, that is, the junction of the mouth with the pharynx. It is subdivided into the vestibule, which lies between the lips and cheek externally and the gums and teeth internally, and the mouth cavity proper, which lies within the alveolar arches, gums, and teeth. The vestibule is a slitlike space that communicates with the exterior through the oral fissures. When the jaws are closed, it communicates with the mouth cavity proper behind the third molar tooth on each side. Superiorly and inferiorly, the vestibule is limited by the reflection of the mucous membrane from the lips and cheeks onto the gums. The cheek forms the lateral wall of the vestibule and is made up of the buccinator muscle, which is covered on the outside by fascia and skin and is lined by mucous membrane. Opposite the upper second molar teeth, a small papilla is present on the mucous membrane, marking the opening of the duct of the parotid salivary gland. The mouth proper has a roof, which is formed by the hard palate in front and the soft palate behind. The floor is formed by the anterior two-thirds of the tongue and by the reflection of the mucous membrane from the sides of the tongue to the gum on the mandible. In the midline, a fold of mucous membrane called frenulum of the tongue connects the undersurface of the tongue to the floor of the mouth. On each side of the frenulum is a small papilla, on the summit of which is the orifice of the duct of the submandibular salivary gland. -

Intrinsic and Extrinsic Factors Collaborate to Activate Pharyngeal Satellite Cells
bioRxiv preprint doi: https://doi.org/10.1101/2020.05.21.108951; this version posted May 23, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 1 Intrinsic and extrinsic factors collaborate to activate pharyngeal satellite cells 2 without muscle injury 3 4 Eunhye Kim1, Yiming Zhang1, Fang Wu1, James Allen1, Katherine E.Vest2, and Hyojung J. Choo1* 5 1Department of Cell Biology, School of Medicine, Emory University, Atlanta, GA 30322, USA 6 2Department of Molecular Genetics, Biochemistry and Microbiology, University of Cincinnati 7 College of Medicine, Cincinnati, OH 45267, USA 8 9 10 11 12 13 14 15 *Corresponding author 16 Hyojung J Choo, Ph.D. 17 Emory University, School of Medicine, Department of Cell Biology, 18 615 Michael street, Rm 542, Atlanta, GA 30322, USA. 19 Office: 404-727-3727, Email: [email protected] 20 1 bioRxiv preprint doi: https://doi.org/10.1101/2020.05.21.108951; this version posted May 23, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. 21 Abstract 22 Satellite cells (SCs), adult muscle stem cells in craniofacial muscles proliferate and 23 differentiate/fuse without injury, unlike quiescent SCs in uninjured limb muscle. However, 24 whether intrinsic or extrinsic factors driving their increased basal activity are largely unknown. -

Histochemical Properties of Myofiber Types and Lack of Muscle Spindles in the Caudal Pharyngeal Constrictor Muscles of Sheep
Histochemical Properties of Myofiber Types and Lack of Muscle Spindles in the Caudal Pharyngeal Constrictor Muscles of Sheep Kouichi WATANABE and Atsushi SUZUKI Graduate School of Agricultural Science, Tohoku University, Aoba-ku, Sendai-shi 981-8555, Japan (Received July 13, 1999; Accepted October 8, 1999) Abstract The purpose of the present study was to examine histochemical properties of myofiber types and presence or absence of muscle spindles in the caudal pharyngeal constrictor (thyropharyngeus and cricopharyngeus) muscles of sheep. Unfixed muscle sections were stained with myosin ATPase (preincubation pH4.3 and 10.5), reduced nicotinamido adenine dinucleotide dehydrogenase, and 3- hydroxybutyrate dehydrogenase (3-HBD). Myofiber types were classified by the differences of the histochemical properties. The thyropharyngeus muscle had 12% type I, 88% type IIA, and no type IIB myofibers. The cricopharyngeus muscle possessed 53% type I, 47% type IIA, and no type IIB myofibers. The myofiber types of the thyropharyngeus and cricopharyngeus muscles were small in diameter. Part of type I myofibers showed a strong 3-HBD activity, whereas all type IIA myofibers showed no 3-HBD activity in the two muscles. No muscle spindle was found in the two muscles. The thyropharyngeus and cricopharyngeus muscles composed of types I and IIA myofibers seem to be adapted to close the pharyngeal cavity repeatedly for the rumination. Animal Science Journal 71 (1): 71-75, 2000 Key words: Thyropharyngeus muscle, Cricopharyngeus muscle, Myofiber type, Muscle spindle, 3- hydroxybutyrate dehydrogenase The pharyngeal constrictor muscles, which include the skeletal muscles have muscle spindles which are the rostral, middle, and caudal muscle groups, transfer proprioceptive receptors sensitive to changes in muscle a bolus of food from the oral cavity through the length. -

Pharynx, Esophagus, Stomach
PHARYNX, ESOPHAGUS, STOMACH Andrea Heinzlmann Veterinary University Department of Anatomy and Histology 25th MARCH 2019 PHARYNX • musculo – membranous passage connects: a. the oral cavity with the esophagus b. the nasal cavity with the larynx http://bvetmed1.blogspot.com/2013/02/to ngue-hyoid-pharynx-deglutition_22.html https://www.imagenesmi.com/im%C3%A1genes/cat-epiglottis-and-glottis-50.html PHARYNX PARTS OF THE PHARYNX: 1. roof 2. lateral walls https://www.msdvetmanual.com/dog-owners/digestive- disorders-of-dogs/disorders-of-the-pharynx-throat-in-dogs 3. rostral portion 4. floor https://www.imagenesmi.com/im%C3%A1genes/cat-epiglottis-and-glottis-50.html http://bvetmed1.blogspot.com/2013/02/tongue-hyoid-pharynx-deglutition_22.html PHARYNX ROOF OF THE PHARYNX: – releated to the basis cranii, vomer and corpus sphenoidalis a. in Car – extends to the C2 b. in Eq 19 – 20 cm, rostral third of roof attached to the basis cranii, caudal two-thirds releated to the guttural pouches c. in Ru, short, not extend caudally beyond the base of the skull d. in Su extends to the level of axis https://markylla.eu/the-respiratory-system-nasal-cavity-pharynx-larynx.html http://vanat.cvm.umn.edu/ungDissect/Lab20/Img20-2.html PHARYNX LATERAL WALLS OF THE PHARYNX: releated to: a. the stylohyoid b. the pterygoid muscles http://bvetmed1.blogspot.com/2013/02/tongue-hyoid-pharynx-deglutition_22.html c. in Eq – the guttural pouches http://vanat.cvm.umn.edu/ungDissect/Lab20/Img20-2.html https://veteriankey.com/head/ PHARYNX FLOOR OF THE PHARYNX: extends: a. from the root of the tongue b. -

Pathophysiology of Obstructive Sleep Apnoea/Hypopnoea Syndrome
159 REVIEW SERIES Thorax: first published as 10.1136/thorax.2003.015859 on 3 February 2004. Downloaded from Sleep ? 2: Pathophysiology of obstructive sleep apnoea/hypopnoea syndrome R B Fogel, A Malhotra, D P White ............................................................................................................................... Thorax 2004;59:159–163. doi: 10.1136/thx.2003.015859 The pathogenesis of airway obstruction in patients with airway. When pharyngeal collapse does occur, it generally does so in the velopharynx (behind the obstructive sleep apnoea/hypopnoea syndrome is soft palate), the oropharynx (from the tip of the reviewed. The primary defect is probably an anatomically soft palate to the epiglottis), or both.45 small or collapsible pharyngeal airway, in combination The human pharynx can be modelled as a collapsible tube, the patency of which can be with a sleep induced fall in upper airway muscle activity. described using a ‘‘balance of pressures’’ con- ........................................................................... cept.26The size of the upper airway depends on the balance between those forces that would collapse the airway (such as negative intralum- bstructive sleep apnoea/hypopnoea syn- inal pressure and increased tissue (extraluminal) drome (OSAHS) is a common disorder pressure) and those that maintain airway which affects 2–4% of middle aged patency (contraction of pharyngeal dilator mus- O 1 cles, see below). The transmural pressure of the women and men in the United States. This disorder is characterised by recurrent sleep pharynx (Ptm) is thus equal to the pressure in the induced collapse of the pharyngeal airway2 lumen (Pl) minus the surrounding pressure in leading to hypoxaemia and hypercapnia, with the tissue (Pti), with the airway lumen becoming arousal from sleep being required to re-establish smaller as Ptm decreases. -
Deep Cervical Fascia
DEEP CERVICAL FASCIA BY DR.M.MD.MUSTAFA SHARIFF DEPT OF ANATOMY SENIOR LECTURER SRMDC&H DEEP CERVICAL FASCIA • It is also called FASCIA COLLI • The deep cervical fascia of neck is clinically very important for it forms various fascial spaces in the neck. • It also provides capsule to the glands and invests the muscles in the region. • It forms protective sheaths around neurovascular structures. • The layers of deep cervical fascia forms planes to direct the spread of infection or pus in the neck. INVESTING LAYER • It lies deep to the platysma and surrounds the neck like a collar. • It forms the roof of the posterior triangle of the neck. • It encloses the sternocleidomastoid and trapezius the two large superficial muscles of the neck on either side. ATTACHMENTS SUPERIORLY: o External occipital protuberance o Superior nuchal line o Mastoid process o Lower border of mandible ▪ Anterior and superiorly it is attached to the lower border of the mandible. ▪ Anteroinferiorly it is attached to the clavicle and manubrium sterni. Posteriorly: ▪ It is attached to the ligamentum nuchae , spine of the C7 vertebrae, spine of scapula , acromian process of the scapula. ▪ The investing layer encloses two salivary glands namely the parotid and submandibular gland. ▪ Tracing the fascia upwards from the clavicle to the lower border of the mandible , it divides into two layers. ▪ Superficial layer is attached to the lower border of mandible and deep layer attached to mylohyoid line. ▪ Between the two layers the submandibular salivary gland and the lymph glands are enclosed. • Near the angle of mandible the investing layer divides into two layers to enclose the parotid gland.