Weekly Semaglutide Vs. Liraglutide Efficacy Profile: a Network Meta
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Semaglutide Versus Liraglutide for Treatment of Obesity
Archives of Diabetes & Obesity DOI: 10.32474/ADO.2021.03.000162 ISSN: 2638-5910 Review Article Semaglutide versus liraglutide for treatment of obesity Nasser Mikhail* *Department of Medicine, Endocrinology Division, David-Geffen UCLA Medical School, USA *Corresponding author: Nasser Mikhail, Endocrinology Division, Department of Medicine, Olive View-UCLA Medical Center, David- Geffen UCLA Medical School, CA, USA Received: April 02, 2021 Published: April 19, 2021 Abstract Background: Once weekly (OW) semaglutide is a glucagon-like peptide-1 receptor agonist (GLP-1 RA) currently under evaluation for treatment of obesity at a dose of 2.4 mg OW. Objective Methods : To compare weight-loss efficacy and safety of once daily (OD) liraglutide 3.0 mg versus OW semaglutide 2.4 mg. : Pubmed research up to March 31, 2021. Randomized trials, pertinent animal studies, and reviews are included. Search Results terms were glucagon-like peptide-1 receptor agonists, weight loss, obesity, liraglutide, semaglutide, efficacy, safety. semaglutide 2.4 mg. However, marked resemblance between trials in terms of study protocols and subjects’ characteristics may allow indirect: No comparison. head to head In clinical trials are trials available of OW tosemaglutide, provide direct this comparison drug was consistently of efficacy ofassociated OD liraglutide with greater 3.0 mg weightversus lossOW than in trials of OD liraglutide. Thus, placebo-corrected percentage weight reduction was -10.3 to -12.4% and -5.4% with OW semaglutide and OD liraglutide, respectively. In patients with type 2 diabetes, corresponding weight reduction was less pronounced with both drugs being -6.2% and -4.3% with OW semaglutide and OD liraglutide, respectively. -

GLP-1 Receptor Agonists
Cognitive Vitality Reports® are reports written by neuroscientists at the Alzheimer’s Drug Discovery Foundation (ADDF). These scientific reports include analysis of drugs, drugs-in- development, drug targets, supplements, nutraceuticals, food/drink, non-pharmacologic interventions, and risk factors. Neuroscientists evaluate the potential benefit (or harm) for brain health, as well as for age-related health concerns that can affect brain health (e.g., cardiovascular diseases, cancers, diabetes/metabolic syndrome). In addition, these reports include evaluation of safety data, from clinical trials if available, and from preclinical models. GLP-1 Receptor Agonists Evidence Summary GLP-1 agonists are beneficial for patients with type 2 diabetes and obesity. Some evidence suggests benefits for Alzheimer’s disease. It is unclear whether it is beneficial for individuals without underlying metabolic disease. Semaglutide seems to be most effective for metabolic dysfunction, though liraglutide has more preclinical data for Alzheimer’s disease. Neuroprotective Benefit: Evidence from many preclinical studies and a pilot biomarker study suggest some neuroprotective benefits with GLP-1 agonists. However, whether they may be beneficial for everyone or only a subset of individuals (e.g. diabetics) is unclear. Aging and related health concerns: GLP-1 agonists are beneficial for treating diabetes and cardiovascular complications relating to diabetes. It is not clear whether they have beneficial effects in otherwise healthy individuals. Safety: GLP-1 agonists are generally safe for most people with minor side effects. However, long-term side effects are not known. 1 Availability: Available Dose: Varies - see Chemical formula: C172H265N43O51 (Liraglutide) as a prescription chart at the end of MW: 3751.262 g/mol medicine. -

A 26-Week Randomized Controlled Trial of Semaglutide Once Daily Versus Liraglutide and Placebo in Patients with Type 2 Diabetes
1926 Diabetes Care Volume 41, September 2018 Ildiko Lingvay,1 Cyrus V. Desouza,2 A 26-Week Randomized Katarina S. Lalic,3 Ludger Rose,4 Thomas Hansen,5 Jeppe Zacho,5 and Controlled Trial of Semaglutide Thomas R. Pieber6 EMERGING THERAPIES: DRUGS AND REGIMENS Once Daily Versus Liraglutide and Placebo in Patients With Type 2 Diabetes Suboptimally Controlled on Diet and Exercise With or Without Metformin Diabetes Care 2018;41:1926–1937 | https://doi.org/10.2337/dc17-2381 OBJECTIVE To investigate the efficacy and safety of once-daily semaglutide in comparison with once-daily liraglutide and placebo in patients with type 2 diabetes. RESEARCH DESIGN AND METHODS This 26-week, multicenter, double-blind trial involved patients diagnosed with 1University of Texas Southwestern Medical Cen- type 2 diabetes with HbA1c 7.0–10.0% (53–86 mmol/mol) and treated with diet ter at Dallas, Dallas, TX and exercise with or without metformin. Patients were randomized 2:2:1 to once- 2University of Nebraska Medical Center, Omaha, daily semaglutide, liraglutide, or placebo in one of four volume-matched doses NE 3Faculty of Medicine, University of Belgrade, and (semaglutide 0.05, 0.1, 0.2, or 0.3 mg and liraglutide 0.3, 0.6, 1.2, or 1.8 mg, with Clinic for Endocrinology, Diabetes and Metabolic both compared within each volume-matched dose group). Primary end point was Diseases, Clinical Center of Serbia, Belgrade, Serbia change in HbA1c from baseline to week 26. 4Institute for Diabetes Research in Munster,¨ RESULTS Munster,¨ Germany 5Novo Nordisk A/S, Søborg, Denmark In total, 705 randomized patients were exposed to trial products. -

OZEMPIC (Semaglutide) Injection, for Subcutaneous Use Initial U.S
HIGHLIGHTS OF PRESCRIBING INFORMATION ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙CONTRAINDICATIONS∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ These highlights do not include all the information needed to use Personal or family history of medullary thyroid carcinoma or in patients OZEMPIC® safely and effectively. See full prescribing information with Multiple Endocrine Neoplasia syndrome type 2 (4). for OZEMPIC. Known hypersensitivity to OZEMPIC or any of the product components (4). OZEMPIC (semaglutide) injection, for subcutaneous use Initial U.S. Approval: 2017 ∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙WARNINGS AND PRECAUTIONS∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙∙ Pancreatitis: Has been reported in clinical trials. Discontinue promptly if WARNING: RISK OF THYROID C-CELL TUMORS pancreatitis is suspected. Do not restart if pancreatitis is confirmed (5.2). See full prescribing information for complete boxed warning. Diabetic Retinopathy Complications: Has been reported in a clinical trial. Patients with a history of diabetic retinopathy should be monitored (5.3). In rodents, semaglutide causes thyroid C-cell tumors. It is Never share an OZEMPIC pen between patients, even if the needle is unknown whether OZEMPIC causes thyroid C-cell tumors, changed (5.4). including medullary thyroid carcinoma (MTC), in humans as Hypoglycemia: When OZEMPIC is used with an insulin secretagogue or the human relevance of semaglutide-induced rodent thyroid C- insulin, consider lowering the dose of the secretagogue or insulin to reduce cell tumors has not been determined (5.1, 13.1). the risk of hypoglycemia (5.5). OZEMPIC is contraindicated in patients with a personal or Acute Kidney Injury: Monitor renal function in patients with renal family history of MTC or in patients with Multiple Endocrine impairment reporting severe adverse gastrointestinal reactions (5.6). Neoplasia syndrome type 2 (MEN 2). -

Subcutaneous Semaglutide, Dulaglutide and Liraglutide 1.2Mg for the Treatment of Type
North Central London Joint Formulary Committee Factsheet Subcutaneous SEMAGLUTIDE▼ (Ozempic®), DULAGLUTIDE▼ (Trulicity®) and LIRAGLUTIDE 1.2mg (Victoza®) Treatment of Type 2 Diabetes Mellitus Start date: December 2019 Review date: August 2022 Document Control Date Version Action July 2016 1.0 New guideline August 2019 1.1 Subcutaneous semaglutide added as the preferred GLP-1 receptor agonist November 2019 1.2 Supply quantities added Agreed by NCL Shared Care Group: December 2019 FACTSHEET TO FACILITATE PRESCRIBING PLEASE NOTE THIS IS NOT A SHARED CARE GUIDELINE, NOR IS IT A FULL SUMMARY OF DRUG INFORMATION. ALWAYS REFER TO THE MOST RECENT BNF AND/OR SUMMARY OF PRODUCT CHARACTERISTICS. Disclaimer This Fact Sheet is registered at North Central London (NCL) Joint Formulary Committee (JFC) and is intended solely for use by healthcare professionals to aid the treatment of patients within NCL. However, this fact sheet is for guidance only, its interpretation and application remains the responsibility of the individual clinician. If in doubt, contact a senior colleague or expert. Clinicians are advised to refer to the manufacturer’s current prescribing information before treating individual patients. The authors and NCL JFC accept no liability for use of this information from this beyond its intended use. While we have tried to compile accurate information in this document, and to keep it updated in a timely manner, we cannot guarantee that it is fully complete and correct at all times. If you identify information within this document that is inaccurate, please report this to the [email protected]. If a patient is harmed as a consequence of following this document, please complete a local incident report and inform [email protected]. -
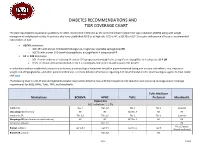
Diabetes Recommendations and Tier Coverage Chart
DIABETES RECOMMENDATIONS AND TIER COVERAGE CHART The American Diabetes Association guidelines for 2020, recommend metformin as the preferred initial treatment for type 2 diabetes (T2DM) along with weight management and physical activity. In patients who have established ASVD or at high risk, CKD, or HF, a SGLT2i or GLP-1 receptor with proven efficacy is recommended independent of A1C. • ASCVD dominates: o GLP-1RA with proven CVD benefit (dulaglutide, liraglutide, injectable semaglutide) OR o SGLT2i with proven CVD benefit (canagliflozin, empagliflozin) if adequate eGFR • HF or CKD dominates: o SGLT2i with evidence of reducing HF and/or CKD progression (empagliflozin, canagliflozin, dapagliflozin) if adequate eGFR OR o If SGLT2i intolerant/contraindicated or eGFR is inadequate, then GLP-1RA with proven CVD benefit In individuals without established cardiovascular disease, pharmacological treatment should be patient-centered taking into account side-effects, cost, impact on weight, risk of hypoglycemia, and other patient preferences. For more detailed information regarding ADA recommendations for pharmacological agents to treat T2DM click here. The following chart is a list of oral and injectable diabetes medications listed by class with their respective A1C reduction and insurance coverage and/or coverage requirements for BCBS, HPHC, Tufts, TMP, and MassHealth. Tufts Medicare Medications BCBSMA HPHC Tufts Preferred MassHealth Biguanides A1C reduction: 1-1.5% metformin Tier 1 Tier 1;2 Tier 1 Tier 1 Covered Glucoghage (metformin) NC NC NC;Tier -

Victoza® (Liraglutide) Injection LEADER: Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results
Novo Nordisk Victoza® (liraglutide) NDA 22341 S-027 Endocrinologic and Metabolic Drug Advisory Committee, June 20, 2017 Victoza® (liraglutide) injection LEADER: Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results NDA 22341 S-027 Briefing Document Endocrinologic and Metabolic Drug Advisory Committee June 20, 2017 Advisory Committee Briefing Materials: Available for Public Release Novo Nordisk Victoza® (liraglutide) NDA 22341 S-027 Endocrinologic and Metabolic Drug Advisory Committee, June 20, 2017 2 of 95 1 Executive summary Introduction Liraglutide is an analog with 97% homology to human glucagon-like peptide-1 (GLP-1) and acts as a GLP-1 receptor agonist (GLP-1 RA). Liraglutide (Victoza®) obtained marketing authorization in the United States (US) in 2010 and is currently approved in over 100 countries worldwide. In the US, Victoza® (for subcutaneous injection 1.2 mg and 1.8 mg once-daily) is indicated as an adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes mellitus (T2DM) as mono- or combination therapy.1 The exposure to Victoza® in the post-marketing setting is extensive; as of 30 June 2016, the cumulative exposure was estimated to be greater than 6 million patient-years of exposure to Victoza®. The LEADER trial (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) was a cardiovascular outcomes trial designed and conducted to determine the effect and long-term safety of liraglutide versus placebo on cardiovascular outcomes as -

Efficacy and Safety of Taspoglutide Versus Sitagliptin
Diabetes Ther (2012) 3:13 DOI 10.1007/s13300-012-0013-8 ORIGINAL RESEARCH Efficacy and Safety of Taspoglutide Versus Sitagliptin for Type 2 Diabetes Mellitus (T-Emerge 4 Trial) Richard M. Bergenstal • Adriana Forti • Jean-Louis Chiasson • Michael Woloschak • Mark Boldrin • Raffaella Balena To view enhanced content go to www.diabetestherapy-open.com Received: August 9, 2012 / Published online: November 9, 2012 Ó The Author(s) 2012. This article is published with open access at Springerlink.com ABSTRACT sitagliptin or placebo, as adjunct to metformin, in patients with inadequately Introduction: The efficacy and safety of controlled type 2 diabetes. taspoglutide, a long-acting human glucagon- Methods: In this randomized, double-blind, like peptide-1 analog, were compared with double-dummy, parallel-group trial, patients were randomized to taspoglutide 10 mg once For the T-emerge 4 Study Group. weekly (QW), 20 mg QW, 100 mg sitagliptin Study investigators listed in the Appendix. once daily (QD), or placebo for 24 weeks, ClinicalTrials.gov identifier: NCT00754988. followed by 28-week short-term and 104-week long-term extension periods. The primary R. M. Bergenstal (&) endpoint was change in glycosylated Park Nicollet International Diabetes Center, hemoglobin (HbA ) after 24 weeks. Minneapolis, MN 55416, USA 1c e-mail: [email protected] Results: In this study, 666 patients (baseline HbA , 7.96% [SD, 0.87]; fasting plasma glucose, A. Forti 1c Universidade Federal do Ceara´, Fortaleza, Brazil 9.61 mmol/L [2.56]; body weight, 92.4 kg [19.3]) were randomized to taspoglutide 10 mg J.-L. Chiasson Centre de Recherche, Centre Hospitalier de QW (n = 190), 20 mg QW (n = 198), l’Universite´ de Montre´al, Universite´ de Montre´al, 100 mg sitagliptin QD (n = 185), or placebo Montreal, QC H2Q 1T8, Canada (n = 93) for 24 weeks. -

Management of Type 2 Diabetes Mellitus Dr Naomi Achong Endocrinologist MBBS(Hons) Bsc FRACP Phd Overview
Management of Type 2 Diabetes Mellitus Dr Naomi Achong Endocrinologist MBBS(Hons) BSc FRACP PhD Overview • Overview of T2DM & glycaemic targets • Treatment after metformin – newer agents on the market • SGLT2 inhibitors • DPP4 agonists • GLP1 antagonists • Insulin options • Newer options – coformulation Diagnosis • ADS position statement • Criteria: • HbA1c > 6.5% • Fasting glucose > 7mmol/L. • Random glucose > 11.1mmol/L • GTT showing fasting > 7 or 2hr > 11.1mmol/L • Patients with IGT have an increased risk of death and vascular disease (regardless of progression to diabetes) as well as microvascular complications • Risk of progression to T2DM is reduced by 58% with lifestyle modification and 31% with metformin 1.The DECODE Study. Arch Intern Med 2001; 161:397-405 2. Singleton JR et al. Diabetes 2003;52(12):2867-2873 3. Diabetes Prevention Program Research Group. N Engl J Med 2002; 346:393-403 Optimising health outcomes in diabetes • Glucose control • Smoking cessation • Blood pressure control • Lipid management with priority to statins • Some circumstances, antiplatelet therapy ADA/EASD – 2015 position statement • Glycaemic targets need to be individualised • Based on modifiable and non-modifiable factors 1. Inzucchi S.E., Bergenstal R.M., Buse J.B., Diamant M., Ferrannini E., Nauck M. et al Diabetologia. 2015; 58: 429-442 1. Inzucchi S.E. et al. Diabetologia. 2015; 58: 429-442 Importance of glycaemic control GOOD GLYCAEMIC CONTROL Reduces diabetes-related complications Reduces total diabetes-related costs UKPDS1 Retrospective database analysis2 1% mean HbA1c reduction results in: HbA1c ≤7% continuously for 1 year results in . 37% 14% 21% 25% Which included: Myocardial 22% lower diabetes infarction medical costs Diabetes-related 28% lower diabetes mortality Diabetes-related pharmacy costs treatment costs Microvascular complications . -

Changing Lives with Next Generation Peptide Therapeutics
Changing lives with next generation peptide therapeutics Zealand Pharma Corporate Presentation May 2019 Forward-looking statements This presentation contains information pertaining to Zealand Pharma A/S (“Zealand"). Neither Zealand nor its management, directors, employees or representatives make any representation or warranty, express or implied, as to the accuracy or completeness of any of the information contained in this presentation or any other information transmitted or made available to the viewer or recipient hereof, whether communicated in written or oral form. This presentation does not constitute or form part of, and should not be construed as, an offer to sell or issue or the solicitation of an offer to buy or acquire Zealand securities, in any jurisdiction, or an inducement to enter into investment activity, nor shall there be any sale of Zealand securities in any state or jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under the securities laws of any such state or jurisdiction. No part of this presentation, nor the fact of its distribution, should form the basis of, or be relied on in connection with, any contract or commitment or investment decision whatsoever. This presentation contains forward-looking statements that reflect management's current views with respect to Zealand's product candidates' development, clinical and regulatory timelines and anticipated results, market opportunity, potential financial performance and other statements of future events or conditions. Although Zealand believes that the expectations reflected in such forward-looking statements are reasonable, no assurance can be given that such expectations will prove to have been correct. -

GLP-1) Agonists Annual Review Date: 12/17/2020
Policy: Glucagon-Like Peptide-1 (GLP-1) Agonists Annual Review Date: 12/17/2020 Impacted Last Revised Date: Drugs: • Tanzeum (albiglutide) • Victoza (liraglutide) 12/17/2020 • Adlyxin (lixisenatide) OVERVIEW Bydureon, Byetta, Tanzeum, Trulicity, Victoza, Adlyxin, Rybelsus and Ozempic are glucagon-like peptide-1(GLP-1) agonists indicated in adjunct to diet and exercise to improve glycemic control in adults with type 2 diabetes. Incretins, such as GLP-1, enhance glucose-dependent insulin secretion and exhibit other antihyperglycemic actions following their release into circulation from the gut. The GLP-1 agonists enhance glucose-dependent insulin secretion by the pancreatic beta-cell, suppress inappropriately elevated glucagon secretion, and slow gastric emptying. All of the GLP-1 agonists, except Rybelsus, are administered by subcutaneous (SC) injection. Bydureon is an extended release formulation of Byetta allowing for once-weekly (QW) administration. Unlike Byetta, Trulicity and Victoza, Bydureon and Tanzeum require reconstitution. Byetta is a twice-daily (BID) injection, Trulicity, Ozempic, and Tanzeum are once-weekly (QW) injections, and Victoza and Adlyxin are a once-daily (QD) injection. Rybelsus is a once daily oral tablet. The prescribing information for Bydureon and Byetta note that neither of these agents are recommended in patients with severe renal impairment (creatinine clearance [CrCl] < 30 mL/min) or end-stage renal disease (ESRD) and should be used with caution in patients with renal transplantation. Victoza’s prescribing information notes that it has not been found to be directly nephrotoxic in animal studies or clinical trials. Caution is recommended when initiating or escalating doses of Victoza in patients with renal impairment. -

INSULIN-CONTAINING PRODUCTS from NOVO NORDISK Storage, and Savings Information
Please see the following pages for Tresiba®, ® ® Xultophy 100/3.6, and Fiasp Dosing, 1 INSULIN-CONTAINING PRODUCTS FROM NOVO NORDISK Storage, and Savings Information. BASAL 100 units/mL; total of 200 units/mL; total of 100 units/mL; total of 300 units/pen; 5-pen pack1 600 units/pen; 3-pen pack1 1000 units/vial; 1 vial/pack1 NDC: 0169-2660-15 NDC: 0169-2550-13 NDC: 0169-2662-11 100 units/mL insulin degludec and 3.6 mg/mL liraglutide; total of 300 units insulin degludec and 10.8 mg liraglutide; 5-pen pack2 NDC: 0169-2911-15 BASAL/GLP-1 RA Approved for use in pumps3 Refer to the insulin infusion pump user manual to see if Fiasp® can be used. Use in accordance with the insulin pump’s Instructions for Use. 100 units/mL; total of 300 units; 100 units/mL; total of 100 units/mL; total of PRANDIAL 5-pen pack3 300 units/pen; 5-cartridge pack3 1000 units/vial; 1 vial/pack3 NDC: 0169-3204-15 NDC: 0169-3205-15 NDC: 0169-3201-11 GLP-1 RA=glucagon-like peptide-1 receptor agonist. Tresiba® Indications and Usage Xultophy® 100/3.6 Indications and Xultophy® 100/3.6 Important Safety Fiasp® Indications and Usage Tresiba® (insulin degludec injection) is indicated to Limitations of Use Information Fiasp® (insulin aspart injection) 100 U/mL is a improve glycemic control in patients 1 year of age and Xultophy® 100/3.6 (insulin degludec and liraglutide injection) rapid-acting insulin analog indicated to improve older with diabetes mellitus. WARNING: RISK OF THYROID C-CELL TUMORS 100 units/mL and 3.6 mg/mL is a combination of insulin ® glycemic control in adult and pediatric patients with degludec and liraglutide and is indicated as an adjunct to diet • Liraglutide, one of the components of Xultophy 100/3.6, causes dose-dependent and treatment-duration-dependent thyroid diabetes mellitus.