First Do No Harm
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
MHA/ONL Patientcarelink Nursing-Sensitive Measure Report
MHA/ONL PatientCareLink Nursing-Sensitive Measure Report Statistical Appendix April 2016 April 2016 Statistical Appendix Contents Explanation of Analysis of the Statistical Significance of Hospital Measure Rates Acute Care Hospitals Bed-size Group Category Listing Specialty Hospital Listing Acute Care Hospitals o NSC-2 Pressure Ulcer Prevalence . Acute Care Hospital Bed-size Group Measure Data Graphs o NSC-3 Patient Falls . Acute Care Hospital Bed-size Group Measure Data Graphs o NSC-4 Falls with Injury . Acute Care Hospital Bed-size Group Measure Data Graphs Specialty Hospitals o NSC-2 Pressure Ulcer Prevalence . Rehabilitation Hospitals Group Measure Data Graphs . Long-term Acute Care Hospitals Group Measure Data Graphs o NSC-3 Patient Falls . Rehabilitation Hospitals Group Measure Data Graphs . Long-term Acute Care Hospitals Group Measure Data Graphs o NSC-4 Falls with Injury . Rehabilitation Hospitals Group Measure Data Graphs . Long-term Acute Care Hospitals Group Measure Data Graphs April 2016 MHA OCT 2007 Analysis of the Statistical Significance of Hospital Measure Rates Because the measure rates for the hospitals are for a specific period of time, and because there is variability in performance over time because of chance and other factors, there is a degree of uncertainty about the extent to which a hospital’s measure rate may reflect its true underlying performance. Without taking this uncertainty into account, we cannot conclude that a hospital with a measure rate that is higher or lower than the group rate is truly performing at a worse or better rate than the group. Statisticians use confidence intervals to account for this uncertainty. -

Community Choice Acute Care Hospital Listing Effective July 1, 2017 When You Use a Community Choice Hospital, You Pay a $275 Inpatient Copay Per Calendar Quarter
UNICARE STATE INDEMNITY PLAN Community Choice Acute Care Hospital Listing Effective July 1, 2017 When you use a Community Choice hospital, you pay a $275 inpatient copay per calendar quarter. Community Choice members can also use additional hospitals for the same $275 copay for certain complex procedures and neonatal ICUs. To look for hospitals, go to unicarestateplan.com and, under the Quick Links tab on the Members page, select Look for health care providers. When you use non-Community Choice hospitals, your out-of-pocket costs are higher. Addison Gilbert Hospital Lawrence Memorial Hospital Anna Jaques Hospital Leominster Hospital (UMass Memorial) Athol Memorial Hospital Leonard Morse Hospital Baystate Franklin Medical Center Lowell General Hospital Baystate Medical Center Mary Lane Hospital (Baystate) Berkshire Medical Center Massachusetts Eye and Ear Beth Israel Deaconess Medical Center – Boston Melrose-Wakefield Hospital Beverly Hospital Mercy Medical Center Brockton Hospital Merrimack Valley Hospital Burbank Hospital (UMass Memorial) Milford Regional Medical Center Cambridge Hospital Milton Hospital (Beth Israel Deaconess) Cape Cod Hospital Morton Hospital Carney Hospital Mount Auburn Hospital Charlton Memorial Hospital Nashoba Valley Medical Center Children’s Hospital Boston Needham Hospital (Beth Israel Deaconess) Cooley Dickinson Hospital New England Baptist Hospital *Dana-Farber Cancer Institute (Boston location only) Noble Hospital (Baystate) Emerson Hospital Norwood Hospital Everett Hospital (formerly Whidden Hospital) Plymouth -

How to Find Us!
How To Find Us! FLOATING HOSPITAL FOR CHILDREN is easily accessible by car from the Massachusetts Turnpike (Route 90), the Central Artery and the Southeast Expressway (Route 93). The hospital is located in downtown Boston — in Chinatown and the Theater District — and within walking distance of the Boston Common, Downtown Crossing and many hotels and restaurants. The main entrance for patients and visitors at Tufts Medical Center is 800 Washington Street, Boston, MA 02111. Floating Hospital for Children is located at 755 Washington Street. Emergency services for adult as well as pediatric patients are located at the North Building, 830 Washington Street. Telephone driving directions are available by calling 617-636-5000, ext. 5 or visit www.tuftsmedicalcenter.org/directions. IF USING GPS for directions, we recommend you plug in the address of our from from 93 New Hampshire 95 New Hampshire parking garage: 274 Tremont Street, Boston, MA 02111. Be sure to include the zipcode. from and Maine Western MA 128 BY CAB AND TRAIN: The hospital is a 15-to-20-minute cab ride from Logan Airport 2 95 and within walking distance of South Station. 1 FROM THE NORTH (I-93 SOUTHBOUND): Logan TUFTS MEDICAL International ▶ Take Exit 20 A (South Station) onto Purchase Street. Continue along Purchase Street Airport from CENTER and FLOATING HOSPITAL (this becomes Surface Artery). New York FOR CHILDREN ▶ Turn right onto Kneeland Street. Go straight several blocks. 90 ▶ Turn left onto Tremont Street. Tufts Medical Center and Floating Hospital for Children Boston Harbor Garage is on your left, just past the Citi Performing Arts Center. -

1 Harvard Medical School Curriculum Vitae Date Prepared
Harvard Medical School Curriculum Vitae Date Prepared: November 1, 2018 Name: Kelly Edwards Irwin, M.D., M.P.H. Home Address: 47 Lexington Road, Concord, MA 01742 Office Address: Center for Psychiatric Oncology and Behavioral Sciences Massachusetts General Hospital Cancer Center 55 Fruit Street, Yawkey 10B, Boston, MA 02114 Work Phone: 617-643-4453 Work Email: [email protected] Work Fax: 617-643-4453 Place of Birth: Methuen, Massachusetts Education 09/97 - 06/01 B.A. Psychology Harvard University (Magna Cum Laude) 08/03 - 06/08 M.D. Medicine Harvard Medical School 07/15 - 05/17 M.P.H. Clinical Effectiveness Harvard School of Public Health Postdoctoral Training 06/08 - 06/09 Internship Medicine Massachusetts General Hospital 06/09 - 06/12 Residency Psychiatry Massachusetts General Hospital/ McLean Hospital 07/11 - 06/12 Chief Resident Psychopharmacology/ Massachusetts General Hospital Outpatient Psychiatry 07/13 - 06/15 Fellowship Dupont-Warren Massachusetts General Hospital Research Fellowship 07/15 - 06/17 Fellowship Program in Cancer Dana-Farber/Harvard Cancer Outcomes Research Center Training Faculty Academic Appointments 07/12 – 08/18 Instructor Psychiatry Harvard Medical School 09/18- present Assistant Professor Psychiatry Harvard Medical School Appointments at Hospitals/Affiliated Institutions 07/12 - present Assistant in Psychiatry Massachusetts General Hospital Psychiatry 07/12 – 06/15 Assistant in Psychiatry McLean Hospital Psychiatry Other Professional Positions 1 09/01 – 4/03 Volunteer, Community Health Promotion Doctors -

A GUIDE to Mclean HOSPITAL Putting People First in Mental Health Care
A GUIDE TO McLEAN HOSPITAL Putting people first in mental health care, research, and education. – Former McLean patient Addiction McLean Hospital provides comprehensive support management, if required, and a daily educational for individuals who want to reduce chemical curriculum to promote prolonged recovery. dependency and regain control of their lives. Knowing that substance use is often seen alongside other psychiatric disorders, such as depression, Our Signature Addiction Recovery Programs anxiety, and trauma, our programs leverage the combine world-class treatment with luxury expertise and wide-ranging mental health and amenities. Each self-pay setting—Fernside, evaluative services throughout McLean Hospital. located in scenic Princeton, Massachusetts, Addiction care is provided in a variety of and Borden Cottage, located in Camden, environments—including inpatient, residential, Maine—offers private accommodations in and day programs (partial hospital)—in order a serene location, which allows patients to to meet the needs of all McLean patients. In- focus on recovery. A month-long stay at either depth assessment, personalized treatment, location allows individuals the opportunity case management, and ongoing support and to concentrate only on their treatment and education are hallmarks of these services. is recommended to ensure success. Based on the proven success of a residential These programs are ideal for adults ages 18 model to treat addiction, McLean offers both and older entering treatment for the first insurance-based and self-pay treatment options. time, those who have previously completed Each of our programs combines evidence-based a treatment program but have relapsed or psychosocial treatment provided by Harvard are at risk to relapse, or those who have tried Medical School-affiliated clinicians. -

Lawrence General Hospital
Massachusetts Hospital Payment Variation 2015 2016 Share of # Hospital Relative Relative Commercial MA Acute Hospital Commercial Relative Price (Weighted Average 2016) Price Price Payments Statewide Results Published By CHIA February 2018 1 Baystate Noble 0.681 0.682 0.2% Baystate Noble Hospital 2 Holyoke Medical Center 0.722 0.728 0.2% Holyoke Medical Center 3 Lawrence General 0.754 0.736 0.4% Lawrence General Hospital 4 Anna Jaques 0.756 0.743 0.5% Anna Jaques Hospital 5 Baystate Wing 0.749 0.752 0.2% Baystate Wing Hospital 6 Cambridge Health Alliance 0.797 0.754 0.6% Cambridge Health Alliance 7 BIDH - Milton 0.760 0.757 0.4% Beth Israel Deaconess- Milton 8 Massachusetts Eye & Ear 0.833 0.760 Massachusetts Eye & Ear 9 Heywood Hospital 0.752 0.763 0.4% Heywood Hospital 10 Signature Brockton 0.785 0.787 0.7% Signature Brockton Hospital 11 Mercy Medical Center 0.806 0.796 0.6% Mercy Medical Center 12 HealthAlliance 0.781 0.804 0.4% HealthAlliance Hospital 80% of Average 13 Emerson 0.846 0.824 1.1% Emerson Hospital 14 Steward Morton 0.855 0.837 0.4% Steward Morton Hospital 15 Milford Regional 0.840 0.840 1.1% Milford Regional Medical Center 16 Lowell General 0.822 0.850 1.6% Lowell General Hospital 85% of Average 17 Northeast Beverly 0.867 0.851 1.3% Northeast Hospital 18 MetroWest 0.856 0.853 1.0% MetroWest Medical Center 19 Steward Holy Family 0.859 0.857 0.7% Steward Holy Family Hospital 20 Winchester Hospital 0.892 0.865 1.6% Beth Israel Deaconess - Plymouth 21 BIDH - Plymouth 0.861 0.865 0.8% Winchester Hospital Underpaid Hospitals -

BIOGRAPHICAL SKETCH NAME: Lois Wonsun Choi
OMB No. 0925-0001 and 0925-0002 (Rev. 03/2020 Approved Through 02/28/2023) BIOGRAPHICAL SKETCH Provide the following information for the Senior/key personnel and other significant contributors. Follow this format for each person. DO NOT EXCEED FIVE PAGES. NAME: Lois Wonsun Choi-Kain eRA COMMONS USER NAME (credential, e.g., agency login): LCHOIKAIN POSITION TITLE: Assistant Professor of Psychiatry, Harvard Medical School; Director, Gunderson Personality Disorder Institute EDUCATION/TRAINING (Begin with baccalaureate or other initial professional education, such as nursing, include postdoctoral training and residency training if applicable. Add/delete rows as necessary.) DEGREE CoMpletion (if Date FIELD OF STUDY INSTITUTION AND LOCATION applicable) MM/YYYY Harvard-Radcliffe College, CaMbridge, MA AB 05/1996 Social Studies Harvard Graduate School of Education, MEd 05/1998 Education CaMbridge, MA ThoMas Jefferson University, Philadelphia, PA MD 06/2002 Medicine Carney Hospital, Dorchester, MA Internship 06/2003 PreliMinary Medicine Massachusetts General Hospital, Boston, Residency 06/2006 Psychiatry MA/McLean Hospital, Belmont, MA McLean Hospital, Belmont, MA Fellowship 06/2008 Psychosocial Fellowship American Psychiatric Institute for Research and Fellowship 06/2009 PrograM for Minority Education (APIRE) and National Institute for Research Training in Mental Health (NIMH) Psychiatry (PMRTP) A. Personal Statement I aM currently the Director of the Gunderson Personality Disorders Institute (GPDI), an internationally recognized center of training -
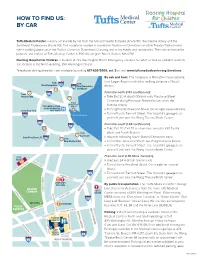
How to Find Us: by Car
HOW TO FIND US: BY CAR Tufts Medical Center is easily accessible by car from the Massachusetts Turnpike (Route 90), the Central Artery and the Southeast Expressway (Route 93). The hospital is located in downtown Boston—in Chinatown and the Theater District—and within walking distance of the Boston Common, Downtown Crossing and many hotels and restaurants. The main entrance for patients and visitors at Tufts Medical Center is 800 Washington Street, Boston, MA 02111. Floating Hospital for Children is located at 755 Washington Street. Emergency services for adult as well as pediatric patients are located at the North Building, 830 Washington Street. Telephone driving directions are available by calling 617-636-5000, ext. 5 or visit www.tuftsmedicalcenter.org/directions. By cab and train: The hospital is a 15-to-20-minute cab ride from Logan Airport and within walking distance of South from from New Hampshire 93 95 New Hampshire Station. 128 and Maine 2 From the north (I-93 southbound): from 95 Western MA » 1 Take Exit 20 A (South Station) onto Purchase Street. Continue along Purchase Street (this becomes the Logan International TUFTS MEDICAL CENTER Airport Surface Artery). & FLOATING HOSPITAL from New York FOR CHILDREN » Turn right onto Kneeland Street. Go straight several blocks. » Turn left onto Tremont Street. The hospital’s garage is on 90 Boston Harbor your left, just past the Wang Theatre/Boch Center. 95 From the south (I-93 northbound): 93 128 » Take Exit 20 (Exit 20 is a two-lane ramp for I-90 East & from West, and South Station). 3 Cape Cod from Providence, RI » Stay left, following South Station/Chinatown signs. -

Fallonhealth.Org Find Your Doctor
Your Network Get more choice with Select Care NETW O O M R H K D H A O S E R L B E SC C T H C E A R What you get • Greater choice at a competitive price. • Access to an expansive network that includes physician practices, community-based hospitals and medical facilities across the Commonwealth and southern New Hampshire. • Plus, worldwide emergency coverage! Please see the back of this insert for a full listing of participating Massachusetts, New Hampshire and Vermont hospitals in Select Care. Participating hospitals Select Care service area fallonhealth.org Find your doctor Just visit fallonhealth.org and follow these simple steps: • Click on “Find a doctor” in the members section, or on the home page. • Click on “Search our regional networks.” If you are looking for a specific provider, type his/her last name. Once you start typing, you will be given a list of providers to choose from. Within the search results, you will see if the provider accepts Select Care. • If you don’t have a particular provider in mind, you can use the advanced search option to search by ZIP code to find a provider convenient to you. You can use this advanced search option for specialists as well as for primary care providers. We update the provider listing on fallonhealth.org every day, so you can trust that you are seeing the most up-to-date information. You can also call our Customer Service Department to have a representative help you find the doctor you’re looking for. -

PEDIATRIC Emergency Medicine
Newton-Wellesley Hospital’s HeaHealthSolthSoururcece Summer 2016 Family-centered Care Shark Bite on Spring Break Pediatric Emergency Medicine Programs & Classes “We were standing in the water getting ready to head back to the “I decided not to have surgery in Florida because it wasn’t urgent. beach when it felt like a bear trap grabbed the back of my foot. I was leaving the next day and decided I wanted to wait until I re- Right in the muscle,” says Dan. “I screamed and then took a couple turned to Boston to determine the best place to have the procedure.” steps to run when I felt something bite me again. With the second bite, the shark got my Achilles tendon so my leg gave out from When Dan returned to Massachusetts, he and his mom visited under me and I shouted, ‘I'm bit! I'm bit!’” Newton-Wellesley Hospital’s Emergency Department to determine his next steps. His care team in the ED recommended that he con- Dan managed to crawl out of the water and look at his ankle. sult an orthopaedic surgeon about the tear in his Achilles tendon There was a big gash across his Achilles down to the bone and his and the possibility of some of the shark tooth still being in his foot was limp. His friends carried him off the beach to get help. ankle, which they were able to see in an X-ray and MRI. “I almost fainted at that moment but didn't,” he says. “It started “After my trip to the Emergency Room my mom and I went to a to bleed like crazy but there was no pain; I guess I was in shock. -

Health Care System ACUTE INPATIENT HOSPITALS
A B C D E 1 ACUTE INPATIENT HOSPITALS PARTICIPATING IN MASSHEALTH (June 2021) Has Inpatient 2 Health Care System Acute Inpatient Hospital Town Psychiatric Unit? 3 Beth Israel Lahey Health Anna Jaques Hospital Newburyport X 4 Heywood Healthcare Athol Hospital Athol 5 Baystate Health Baystate Franklin Medical Center Greenfield X 6 Baystate Health Baystate Medical Center Springfield X 7 Baystate Health Baystate Noble Hospital Westfield X 8 Baystate Health Baystate Wing Hospital Palmer X 9 Berkshire Health Systems Berkshire Fairview Hospital Great Barrington 10 Berkshire Health Systems Berkshire Medical Center Pittsfield X 11 Beth Israel Lahey Health Beth Israel Deaconess Hospital - Milton Milton 12 Beth Israel Lahey Health Beth Israel Deaconess Hospital - Needham Needham 13 Beth Israel Lahey Health Beth Israel Deaconess Hospital - Plymouth Plymouth X 14 Beth Israel Lahey Health Beth Israel Deaconess Medical Center Boston X 15 Beth Israel Lahey Health Beverly Hospital (aka Northeast Health) Beverly X 16 Boston Children's Hospital Boston X 17 Boston Medical Center Boston 18 MassGeneralBrigham Brigham & Women's Hospital Boston 19 MassGeneralBrigham Brigham and Women's Faulkner Hospital Boston X 20 Cambridge Health Alliance Cambridge Hospital Cambridge X 21 Cape Cod Healthcare Cape Cod Hospital Hyannis X 22 Steward Health Care Carney Hospital Boston X 23 MassGeneralBrigham Cooley Dickinson Hospital Northampton X 24 Dana Farber Cancer Institute Boston 25 Emerson Hospital Concord X 26 Cambridge Health Alliance Everett Hospital Everett X 27 Cape -

Invention Disclosure Form
Invention Disclosure Form For Internal Use Only Invention Number: Contact/Submission Info Please address all questions and return an electronic copy of the completed form to: Anthony Sutton, Senior Invention Administrator Email: [email protected] P: (617) 954-9721 When complete, please save F: (617) 954-9361 and hit ‘Submit’ button to (While filing form online, please have ‘insert’ key inactive) email directly for submission. 1. TITLE OF INVENTION 2. CATEGORY OF INVENTION Patent Material Software Copyright Trademark 3. DESCRIPTION OF THE INVENTION Describe the Invention to the extent known at this time. A. Key concepts of Invention, including nature, stage, purpose of operation of the invention including technical characteristics: (In addition, please attach manuscript, presentation, poster, or other documents, including any public disclosure documents) B. Distinguishing novel features of Invention: C. Envisioned commercial products or processes: INVENTION DISCLOSURE FORM 4. PUBLIC DISCLOSURE OR USE Public disclosure or use of an invention prior to filing a patent application will either limit or eliminate patent rights, dependent upon the extent of what was disclosed. A. Any past or future manuscript submission of Invention ? Yes, Date: No Expected date of online or paper publication B. Any past or future abstract, poster or talk of Invention? Yes, Date: No C. Any past or future journal publications (online and print)? Yes, Date: No D. Any past or future disclosures outside hospital of Invention? Yes, Date: Entity: No E. Any other past or future public disclosures? Type: Yes, Date: Entity: No F. Has Invention been used, tested or offered for sale? Yes, Date: No 5.