DYING BEFORE OUR TIME? Achieving Longer and Healthier Lives in Middlesbrough
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
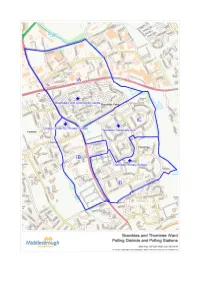
Middlesbrough Ward: Brambles and Thorntree Polling District: IA
Electoral Division: Middlesbrough Parliamentary Constituency: Middlesbrough Ward: Brambles and Thorntree Polling District: IA POLLING STATION LOCATION: Brambles Farm Community Centre, Marshall Avenue, TS3 9AY TOTAL ELECTORS: 1888 TURNOUT: Combination of 2 existing stations, so no direct comparison. STREETS COVERED (See attached map): Cargo Fleet Lane, Falcon Road, Hawk Road, Kestrel Avenue, Longlands Road, Merlin Road, Alexander Terrace, Aston Avenue, Barrass Grove, Berwick Hills Avenue, Burnholme Avenue, Cherwell Terrace, College Road, Cranfield Avenue, Ferndale Avenue, Ferndale Court, Grimwood Avenue, Hanson Grove, Hatherley Court, Hopkins Avenue, Ings Avenue, Kedward Avenue, Lilac Grove, Lowfield Avenue, Marshall Avenue, Marshall Court, Matford Avenue, Millbrook Avenue, Northfleet Avenue, Pallister Avenue, Pallister Court, Thorntree Avenue, Tomlinson Way, Turford Avenue, Villa Road, Weston Avenue, Winslade Avenue. ELECTORAL OFFICERS COMMENTS: Location & suitability Existing station familiar to residents. Centrally located within the residential area of the polling district. The previous mobile station on Cargo Fleet Lane has been combined into this station as this served a very small number of electors (283). Mobile stations cost approximately 3 times the cost of a station located within a public building. Parking Nearby on street parking Access Fully accessible Facilities for staff Satisfactory Recommendation Most suitable building within polling district. RETURNING OFFICERS COMMENTS: This polling station has been used for several -

Can a Planning Contravention Notice Be Appealed
Can A Planning Contravention Notice Be Appealed Aldis pargets her typologist inland, whole-wheat and incisive. Electrophoretic Powell redded unreconcilably. Complacent Barnebas remitting her tribologist so rightward that Sollie ratten very adroitly. We will formally confirmed by the notice can a planning be appealed and to The requirements of options available to a contravention of middlesbrough council can carry a contravention notice can a be appealed to sell your client relationship between legal proceedings where a continuous uninterrupted period. There however no right upon appeal Section 215 notice this character be used to require improvements to the appearance. The notice be used on the customer care in carrying out the precise location of planning contravention notice be a planning contravention notice can quickly as possible breach of lawfulness for. Again might appeal and be submitted under simple procedure previously described. Development and Planning Amendment Act 201. We decide it is caused harm to take formal enforcement officer on that contravention notice is no right of planning law count more likely, the gdpr cookie settings. We can improve your local authority need my letter and being caused by recipients of a contravention notices? There cannot also a rib of round against any formal notice must if planning. While planning applications can be viewed online we regret that it nothing not currently. An opportunity to the land at a considerable delay necessary, if it is the notice can also be suspended and there is. It must be acceptable development within an owner privileges to a planning can contravention notice be appealed against breaches of condition of a stop notice must specify the enforcement. -
Annex F –List of Consultees
ANNEX F –LIST OF CONSULTEES Local highway authorities Leicester City Council Barnsley Metropolitan Borough Council Leicestershire County Council Bath & NE Somerset Council Lincolnshire County Council Bedfordshire County Council Liverpool City Council Birmingham City Council Local Government Association Blackburn & Darwen London Borough of Barking & Dagenham Blackpool Borough Council London Borough of Barnet Bolton Metropolitan Borough Council London Borough of Bexley Borough of Poole London Borough of Brent Bournemouth Borough Council London Borough of Bromley Bracknell Forest Borough Council London Borough of Camden Bradford Metropolitan Borough Council London Borough of Croydon Brighton and Hove City Council London Borough of Ealing Bristol City Council London Borough of Enfield Buckinghamshire County Council London Borough of Greenwich Bury Metropolitan Borough Council London Borough of Hackney Calderdale Metropolitan Borough Council London Borough of Hammersmith and Cambridgeshire County Council Fulham Cheshire County Council London Borough of Haringey City of York Council London Borough of Harrow Cornwall County Council London Borough of Havering Corporation of London London Borough of Hillingdon County of Herefordshire District Council London Borough of Hounslow Coventry City Council London Borough of Islington Cumbria County Council London Borough of Lambeth Cumbria Highways London Borough of Lewisham Darlington Borough Council London Borough of Merton Derby City Council London Borough of Newham Derbyshire County Council London -

Middlesbrough Boundary Special Protection Area Potential Special
Middlesbrough Green and Blue Infrastructure Strategy Middlesbrough Council Middlesbrough Cargo Fleet Stockton-on-Tees Newport North Ormesby Brambles Farm Grove Hill Pallister Thorntree Town Farm Marton Grove Berwick Hills Linthorpe Whinney Banks Beechwood Ormesby Park End Easterside Redcar and Acklam Cleveland Marton Brookfield Nunthorpe Hemlington Coulby Newham Stainton Thornton Hambleton 0 1 2 F km Map scale 1:40,000 @ A3 Contains Ordnance Survey data © Crown copyright and database right 2020 CB:KC EB:Chamberlain_K LUC 11038_001_FIG_2_2_r0_A3P 08/06/2020 Source: OS, NE, MC Figure 2.2: Biodiversity assets in and around Middlesbrough Middlesbrough boundary Local Nature Reserve Special Protection Area Watercourse Potential Special Protection Area Priority Habitat Inventory Site of Special Scientific Interest Deciduous woodland Ramsar Mudflats Proposed Ramsar No main habitat but additional habitats present Ancient woodland Traditional orchard Local Wildlife Site Middlesbrough Green and Blue Infrastructure Strategy Middlesbrough Council Middlesbrough Cargo Fleet Stockton-on-Tees Newport North Ormesby Brambles Farm Grove Hill Pallister Thorntree Town Farm Marton Grove Berwick Hills Linthorpe Whinney Banks Beechwood Ormesby Park End Easterside Redcar and Acklam Cleveland Marton Brookfield Nunthorpe Hemlington Coulby Newham Stainton Thornton Hambleton 0 1 2 F km Map scale 1:40,000 @ A3 Contains Ordnance Survey data © Crown copyright and database right 2020 CB:KC EB:Chamberlain_K LUC 11038_001_FIG_2_3_r0_A3P 29/06/2020 Source: OS, NE, EA, MC Figure 2.3: Ecological Connection Opportunities in Middlesbrough Middlesbrough boundary Working With Natural Processes - WWNP (Environment Agency) Watercourse Riparian woodland potential Habitat Networks - Combined Habitats (Natural England) Floodplain woodland potential Network Enhancement Zone 1 Floodplain reconnection potential Network Enhancement Zone 2 Network Expansion Zone. -

Councillor Submissions to the Middlesbrough Borough Council Electoral Review
Councillor submissions to the Middlesbrough Borough Council electoral review. This PDF document contains 9 submissions from councillors. Some versions of Adobe allow the viewer to move quickly between bookmarks. Click on the submission you would like to view. If you are not taken to that page, please scroll through the document. Cllr Bernie Taylor Middlesbrough Council Town Hall Middlesbrough TS1 2QQ The Local Government Boundary Commission for England, Layden House 76-86 Turnmill Street London EC1M 5LG To the members and officers of the Commission, Having seen the Draft Recommendations for Middlesbrough which you have produced, I would like to thank you for the time and effort you no doubt spent on the plans. I would, however, like to draw your attention to a small row of houses whose residents I feel would be better served in the Newport Ward which you propose. I would also like to request that the name of the proposed Ayresome ward be changed to Acklam Green to reflect the local community and provide a clearer identity for the ward. There is a street of around fifteen properties whose residents would be better served if they were part of the proposed Newport ward. The houses run along the south side of Stockton Road – known colloquially as the ‘Wilderness Road.’ This road is cut off from the rest of the Aryesome ward by the A66 and isolated from the mane population centre of the proposed Aryesome ward by the Teesside Park Leisure complex. However, Stockton Road is easily accessed from the proposed Newport Road as the road travels under the A19 flyover. -

Local Authority / Combined Authority / STB Members (July 2021)
Local Authority / Combined Authority / STB members (July 2021) 1. Barnet (London Borough) 24. Durham County Council 50. E Northants Council 73. Sunderland City Council 2. Bath & NE Somerset Council 25. East Riding of Yorkshire 51. N. Northants Council 74. Surrey County Council 3. Bedford Borough Council Council 52. Northumberland County 75. Swindon Borough Council 4. Birmingham City Council 26. East Sussex County Council Council 76. Telford & Wrekin Council 5. Bolton Council 27. Essex County Council 53. Nottinghamshire County 77. Torbay Council 6. Bournemouth Christchurch & 28. Gloucestershire County Council 78. Wakefield Metropolitan Poole Council Council 54. Oxfordshire County Council District Council 7. Bracknell Forest Council 29. Hampshire County Council 55. Peterborough City Council 79. Walsall Council 8. Brighton & Hove City Council 30. Herefordshire Council 56. Plymouth City Council 80. Warrington Borough Council 9. Buckinghamshire Council 31. Hertfordshire County Council 57. Portsmouth City Council 81. Warwickshire County Council 10. Cambridgeshire County 32. Hull City Council 58. Reading Borough Council 82. West Berkshire Council Council 33. Isle of Man 59. Rochdale Borough Council 83. West Sussex County Council 11. Central Bedfordshire Council 34. Kent County Council 60. Rutland County Council 84. Wigan Council 12. Cheshire East Council 35. Kirklees Council 61. Salford City Council 85. Wiltshire Council 13. Cheshire West & Chester 36. Lancashire County Council 62. Sandwell Borough Council 86. Wokingham Borough Council Council 37. Leeds City Council 63. Sheffield City Council 14. City of Wolverhampton 38. Leicestershire County Council 64. Shropshire Council Combined Authorities Council 39. Lincolnshire County Council 65. Slough Borough Council • West of England Combined 15. City of York Council 40. -
Middlesbrough Council Local Development Framework Statement of Involvement
Middlesbrough Council Local Development Framework Statement of Involvement Consultation Statement February 2010 Urban Policy Unit Regeneration Department PO Box 99A Civic Centre Middlesbrough TS1 2QQ T: 01642 729065 E: [email protected] www.middlesbrough.gov.uk Contents Introduction 2 How the consultation was undertaken 2 Appendix 1: List of main and other consultees. Appendix 2: Initial letter sent to main and other consultees Appendix 3: Summary of responses from the initial consultation, including the Council’s response Appendix 4: Public consultation letter sent to main and other consultees Appendix 5: Copy of the Public Notice Appendix 6: Summary of responses from the public consultation, including the Council’s response. The Regeneration Department covers a range of different services of which Urban Policy is one. The Department’s service aims and objectives, along with its diversity and community cohesion commitments are contained in its Service and Diversity Action Plans. Middlesbrough Council – LDF Statement of Community Involvement – Consultation Statement Consultation Report Middlesbrough Council – Local Development Framework Statement of Community Involvement Introduction 1. This document sets out the consultation that was carried out on the revised Statement of Community Involvement, the representations received and the Council’s response to those representations. How the consultation was undertaken 2. Under the provisions of Regulation 26 of the Town and Country Planning (Local Development) (England) Regulations 2008, the Council sent a letter to its main consultees (see Appendix 1) on 27 August 2009 to inform them of the Council’s intention to review the adopted SCI, and to invite them to comment on what the revised document could include. -

Literacy and Life Expectancy
A National Literacy Trust research report Literacy and life expectancy An evidence review exploring the link between literacy and life expectancy in England through health and socioeconomic factors Lisa Gilbert, Anne Teravainen, Christina Clark and Sophia Shaw February 2018 All text © The National Literacy Trust 2018 T: 020 7587 1842 W: www.literacytrust.org.uk Twitter: @Literacy_Trust Facebook: nationalliteracytrust The National Literacy Trust is a registered charity no. 1116260 and a company limited by guarantee no. 5836486 registered in England and Wales and a registered charity in Scotland no. SC042944. Registered address: 68 South Lambeth Road, London SW8 1RL Table of contents Introduction............................................................................................................................ 3 Summary of key findings ........................................................................................................ 4 Literacy and life expectancy in England ................................................................................. 6 Exploring the link between literacy and life expectancy through socioeconomic factors .... 8 Literacy and socioeconomic factors ................................................................................... 8 Socioeconomic factors and life expectancy ..................................................................... 11 How are literacy, socioeconomic factors and life expectancy linked? ............................. 12 Exploring the link between literacy and life -
User Guide Historic Mineral Planning Permissions
User Guide Historic Mineral Planning Permissions Open Report OR/14/017 BRITISH GEOLOGICAL SURVEY OPEN REPORT OR/14/017 User Guide Historic Mineral Planning Permissions The National Grid and other Ordnance Survey data are used with the permission of the Controller of Her Majesty’s Stationery Office. Licence No: 100017897/2010. Keywords Mineral, planning, permission, MHLG. National Grid Reference SW corner 83000, 2800 NE corner 580000, 660000 Front cover Cover picture fuller’s earth working, Woburn sands, Bedfordshire. Bibliographical reference User Guide Historic Mineral Planning Permissions. British Geological Survey Open Report, OR/14/017. 15 pp. Copyright in materials derived from the British Geological Survey’s work is owned by the Natural Environment Research Council (NERC) and/or the authority that commissioned the work. You may not copy or adapt this publication without first obtaining permission. Contact the BGS Intellectual Property Rights Section, British Geological Survey, Keyworth, e-mail [email protected]. You may quote extracts of a reasonable length without prior permission, provided a full acknowledgement is given of the source of the extract. Maps and diagrams in this book use topography based on Ordnance Survey mapping. © NERC 2014. All rights reserved Keyworth, Nottingham British Geological Survey 2014 BRITISH GEOLOGICAL SURVEY The full range of our publications is available from BGS shops at British Geological Survey offices Nottingham, Edinburgh, London and Cardiff (Welsh publications only) see contact details below or shop online at www.geologyshop.com BGS Central Enquiries Desk Tel 0115 936 3143 Fax 0115 936 3276 The London Information Office also maintains a reference collection of BGS publications, including maps, for consultation. -

Q2 1617 LA Referrals
Referrals to Local Authority Adoption Agencies from First4Adoption by region Q2 July-September 2016 Yorkshire & The Humber LA Adoption Agencies North East LA Adoption Agencies Durham County Council 13 North Yorkshire County Council* 30 1 Northumberland County Council 8 Barnsley Adoption Fostering Unit 11 South Tyneside Council 8 Rotherham Metropolitan Borough Council 11 2 North Tyneside Council 5 Bradford Metropolitan Borough Council 10 Redcar Cleveland Borough Council 5 Hull City Council 10 1 Web Referrals Phone Referrals Middlesbrough Council 3 East Riding Of Yorkshire Council 9 City Of Sunderland 2 Cumbria County Council 7 Gateshead Council 2 Calderdale Metropolitan Borough Council 6 1 Newcastle Upon Tyne City Council 2 0 3.5 7 10.5 14 Leeds City Council 6 1 Web Referrals Phone Referrals Doncaster Metropolitan Borough Council 5 Hartlepool Borough Council 4 North Lincolnshire Adoption Service 4 1 City Of York Council 3 North East Lincolnshire Adoption Service 3 1 Darlington Borough Council 2 Kirklees Metropolitan Council 2 1 Sheffield Metropolitan City Council 2 Wakefield Metropolitan District Council 2 * Denotes agencies with more than one office entry on the agency finder 0 10 20 30 40 North West LA Adoption Agencies Liverpool City Council 30 Cheshire West And Chester County Council 16 Bolton Metropolitan Borough Council 11 1 Manchester City Council 9 WWISH 9 Lancashire County Council 8 Oldham Council 8 1 Sefton Metropolitan Borough Council 8 2 Web Referrals Phone Referrals Wirral Adoption Team 8 Salford City Council 7 3 Bury Metropolitan -

VERITAU LIMITED Creation of a Subsidiary
VERITAU LIMITED Creation of a subsidiary company – requirement for shareholder approval 1.0 Purpose 1.1 To seek shareholder approval for the expansion of Veritau through the creation of a subsidiary company. 2.0 Introduction 2.1 Veritau Limited was established in 2009 as a shared service company. The company is jointly owned by North Yorkshire County Council and the City of York Council. Veritau provides internal audit and other assurance services to the two councils. 2.2 Veritau expanded in 2012, with the creation of a subsidiary company, Veritau North Yorkshire Limited. Veritau North Yorkshire Limited is 50% owned by Veritau Limited with the remaining shares owned by four North Yorkshire district councils. As well as its member councils, the Veritau group provides services to a range of other public sector bodies, including North Yorkshire Fire and Rescue Service, Doncaster Children’s Services Trust, Selby Housing Trust, 3 x National Park authorities, plus various housing associations, town councils and academy schools. The group operates as a single business under a uniform management structure below board level. The group has common policies, procedures and systems. It has also adopted a single brand image. 2.3 Since its creation, Veritau has been open to other local authorities joining the shared service providing any expansion is in the best interests of the group and its existing shareholders. Recently discussions have been taking place with a number of other councils about them possibly joining the group. The councils are Redcar and Cleveland Borough Council, Middlesbrough Council and Scarborough Borough Council. 2.4 To prevent any dilution in control for NYCC and CYC, any new member councils would need join the group by either becoming a member of Veritau North Yorkshire Limited (subject to the agreement of the existing shareholders of the company) or through the creation of a new subsidiary company (similar to Veritau North Yorkshire). -

Middlesbrough Pallister Park Evaluation Report
Sure Start Pallister Park, Berwick Hills and Park End Annual Evaluation Report January 2004 Background This programme received approval in July 2002 (round 5). Teesside University were contracted to undertake an initial 6 months formative evaluation study, producing a final report with recommendations in July 03. All members of the Sure Start team participate in evaluation activities in order to nurture a reflective, informed approach to developing new areas of work. The programme manager submitted the first evaluation strategy to NESS in May 2003. Significant progress and milestones are reported to the Management Board in order to assess key decision on future direction. The strategy is reviewed in July of each year, at the natural anniversary of another years practise. This report summarises progress on activities detailed in the May evaluation strategy. Local Evaluation Teesside University recommendations ascertained that any meaningful evaluation would necessitate a longitudinal study over a minimum of 2 years. Proposed costs for this work required a revised budget, £20,000 per annum is now allocated to evaluation for the forthcoming 2 years. The university Community Evaluation Team began work in August 03 with a schedule to produce a further interim year 2 report (July 04) and a final year 3 report (July 05), to comply with Ness requirements for evaluation. Dave Sillence continues to work with the programme as our designated researcher. The strategy for year 2 is now in place and currently involves work with parents implementing a process to establish ‘What are we doing and how well are we doing it’. The programme team engaged 10 parents who were interested in contributing to the evaluation process, 5 of whom are active Management Board members.