SSHM Proceedings 2012-2014
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Emergency Department Activity
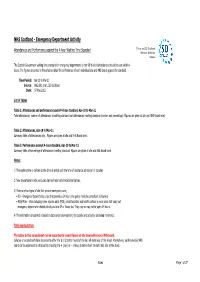
NHS Scotland - Emergency Department Activity Attendances and Performance against the 4-hour Waiting Time Standard This is an ISD Scotland National Statistics release. The Scottish Government waiting time standard for emergency departments is that 98 % of all attendances should be seen within 4 hours. The figures presented in these tables detail the performance of each individual site and NHS board against the standard. Time Period: Apr-10 to Mar-11 Source: A&E data mart, ISD Scotland Date: 07 May 2012 List of Tables Table 1: Attendances and performance against 4-hour standard, Apr-10 to Mar-11 Total attendances, number of attendances breaching standard and attendances meeting standard (number and percentage). Figures are given at site and NHS Board level. Table 2: Attendances, Apr-10 to Mar-11 Summary table of attendances only. Figures are given at site and NHS Board level. Table 3: Performance against 4-hour standard, Apr-10 to Mar-11 Summary table of percentage of attendances meeting standard. Figures are given at site and NHS Board level. Notes: 1) The waiting time is defined as the time of arrival until the time of discharge, admission or transfer. 2) New presentations only; excludes planned return and recall attendances. 3) There are two types of site that provide emergency care; • ED - Emergency Departments; sites that provide a 24 hour emergency medicine consultant led service • MIU/Other - sites including minor injuries units (MIU), small hospitals and health centres in rural areas that carry out emergency department related activity and are GP or Nurse led. They may or may not be open 24 hours. -

Contract Between Scottish Ministers
CONTRACT BETWEEN SCOTTISH MINISTERS AND GEOAMEY PECS LTD FOR THE SCOTTISH COURT CUSTODY AND PRISONER ESCORT SERVICE (SCCPES) REFERENCE: 01500 MARCH 2018 Official No part of this document may be disclosed orally or in writing, including by reproduction, to any third party without the prior written consent of SPS. This document, its associated appendices and any attachments remain the property of SPS and will be returned upon request. 1 | P a g e 01500 Scottish Court Custody and Prisoner Escort Service (SCCPES) FORM OF CONTRACT CONTRACT No. 01500 This Contract is entered in to between: The Scottish Ministers, referred to in the Scotland Act 1998, represented by the Scottish Prison Service at the: Scottish Prison Service Calton House 5 Redheughs Rigg Edinburgh EH12 9HW (hereinafter called the “Purchaser”) OF THE FIRST PART And GEOAmey PECS Ltd (07556404) The Sherard Building, Edmund Halley Road Oxford OX4 4DQ (hereinafter called the “Service Provider”) OF THE SECOND PART The Purchaser hereby appoints the Service Provider and the Service Provider hereby agrees to provide for the Purchaser, the Services (as hereinafter defined) on the Conditions of Contract set out in this Contract. The Purchaser agrees to pay to the Service Provider the relevant sums specified in Schedule C and due in terms of the Contract, in consideration of the due and proper performance by the Service Provider of its obligations under the Contract. The Service Provider agrees to look only to the Purchaser for the due performance of the Contract and the Purchaser will be entitled to enforce this Contract on behalf of the Scottish Ministers. -

Offers Over £220,000 Greystones, Leodebest, Latheron, KW5
Greystones, Leodebest, Latheron, KW5 6DQ This generous detached home enjoys a superb position affording unrivalled views and is offered for sale with approximately 3 acres of ground ensuring it to be an ideal family home/holiday home or for those seeking a "lifestyle" opportunity. • Entrance/Dining Hall • Music Room • Lounge • Upper Landing • Kitchen/Family Room • 5 Bedrooms (1 En-Suite) • Utility Room • Family Bathroom • Cloakroom • Garage Offers over £220,000 DESCRIPTION "Greystones" is an impressive 5 bedroom detached dwellinghouse, situated just off the famous North Coast 500 route and is set amidst some of the most spectacular scenery in the Highlands. The property, which was built in 2007, sits in generous grounds extending to approximately 3 acres, with the house site having been decrofted and the remainder of the ground is Owner Occupied croftland. In excellent order throughout, the property benefits from oil fired central heating and UPVC replacement double glazed windows. Viewing is a must of this beautiful home to fully appreciate the elevated location with stunning views and thoughtful layout of the accommodation which provides bright and airy rooms throughout. This delightful home will appeal to a spectrum of buyers to include those seeking a spacious family home, those with an equestrian interest or for other livestock, those seeking a "lifestyle" change or equally those looking for a holiday home as the property is well placed to take full advantage of a number of outdoor pursuits to include walking, shooting, fishing and is close to the beaches and harbour. LOCATION The property is situated at Latheron which is south west of Lybster on the A9 road and is part of the famous North Coast 500 route. -

Accident and Emergency: Performance Update
Accident and Emergency Performance update Prepared by Audit Scotland May 2014 Auditor General for Scotland The Auditor General’s role is to: • appoint auditors to Scotland’s central government and NHS bodies • examine how public bodies spend public money • help them to manage their finances to the highest standards • check whether they achieve value for money. The Auditor General is independent and reports to the Scottish Parliament on the performance of: • directorates of the Scottish Government • government agencies, eg the Scottish Prison Service, Historic Scotland • NHS bodies • further education colleges • Scottish Water • NDPBs and others, eg Scottish Police Authority, Scottish Fire and Rescue Service. You can find out more about the work of the Auditor General on our website: www.audit-scotland.gov.uk/about/ags Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. We help the Auditor General for Scotland and the Accounts Commission check that organisations spending public money use it properly, efficiently and effectively. Accident and Emergency | 3 Contents Summary 4 Key messages 7 Part 1. A&E waiting times 9 Part 2. Reasons for delays in A&E 20 Part 3. Action by the Scottish Government 37 Endnotes 41 Appendix 1. NHS Scotland A&E departments and minor injury units 43 Appendix 2. National context for A&E and unscheduled care, 2004 to 2014 45 Exhibit data When viewing this report online, you can access background data by clicking on the graph icon. The data file will -

A Guide for Families Living with Dementia in West Highland
A guide for families living with dementia in West Highland Supported by Argyll & Bute Council, The Highland Council and NHS Highland Compiled May 2012 2 Welcome and how to use this guide This guide has been produced as a result of many discussions with families and staff who are supporting someone with dementia in the NHS Highland area. The guide is broken into three sections: • Section 1 Issues and things to think about. This section provides an overview of important issues and identifies where to find out further information. • Section 2 Who’s who and what’s their role. This outlines the main staff and agencies likely to be involved in supporting the person with dementia and their key roles. • Section 3 Local and national supports and services. This section provides contact details for advice, information and support in your area for you and the person with dementia. We hope you find this guide a real help to you and your family in living with dementia. Signatories: Henry Simmons – Chief Executive, Alzheimer Scotland Elaine Mead - Chief Executive, NHS Highland Cleland Sneddon - Executive Director, Community Services, Argyll & Bute Council Bill Alexander - Director of Health & Social Care, Highland Council 3 Acknowledgements We are indebted to all the family members who took part in the research for giving their time, suggestions and commitment, which has provided the foundation of the content, design and style of the guide. The guide has drawn on a number of resources. In particular we would like to thank NHS Health Scotland (www.healthscotland.com) for their permission to refer to the following publications: • Facing dementia – how to live well with your diagnosis • Coping with dementia – a practical handbook for carers Single copies of the above booklets and their accompanying DVDs are available to people with dementia, their partners, families and friends from the Dementia Helpline on 0808 808 3000. -
Caithness and Sutherland Proposed Local Development Plan Committee Version November, 2015
Caithness and Sutherland Proposed Local Development Plan Committee Version November, 2015 Proposed CaSPlan The Highland Council Foreword Foreword Foreword to be added after PDI committee meeting The Highland Council Proposed CaSPlan About this Proposed Plan About this Proposed Plan The Caithness and Sutherland Local Development Plan (CaSPlan) is the second of three new area local development plans that, along with the Highland-wide Local Development Plan (HwLDP) and Supplementary Guidance, will form the Highland Council’s Development Plan that guides future development in Highland. The Plan covers the area shown on the Strategy Map on page 3). CaSPlan focuses on where development should and should not occur in the Caithness and Sutherland area over the next 10-20 years. Along the north coast the Pilot Marine Spatial Plan for the Pentland Firth and Orkney Waters will also influence what happens in the area. This Proposed Plan is the third stage in the plan preparation process. It has been approved by the Council as its settled view on where and how growth should be delivered in Caithness and Sutherland. However, it is a consultation document which means you can tell us what you think about it. It will be of particular interest to people who live, work or invest in the Caithness and Sutherland area. In preparing this Proposed Plan, the Highland Council have held various consultations. These included the development of a North Highland Onshore Vision to support growth of the marine renewables sector, Charrettes in Wick and Thurso to prepare whole-town visions and a Call for Sites and Ideas, all followed by a Main Issues Report and Additional Sites and Issues consultation. -

LHB37 LOTHIAN HEALTH BOARD Introduction 1 Agenda of Meetings of Lothian Health Board, 1987-1995 2 Agenda of Meetings of Lothia
LHB37 LOTHIAN HEALTH BOARD Introduction 1 Agenda of Meetings of Lothian Health Board, 1987-1995 2 Agenda of Meetings of Lothian Health Board Committees, 1987-1989 2A Minutes of Board, Standing Committees and Sub-Committees, 1973-1986 2B Draft Minutes of Board Meetings, 1991-2001 2C [not used] 2D Area Executive Group Minutes, 1973-1986 2E Area Executive Group Agendas and Papers, 1978-1985 2F Agenda Papers for Contracts Directorate Business Meetings, 1993-1994 2G Agenda Papers of Finance, Manpower and Establishment Committee, 1975-1979 2H Agenda papers of the Policy and Commissioning Team Finance and Corporate Services Sub- Group, 1994-1995 2I [not used] 2J Minutes and Papers of the Research Ethics Sub-Committees, 1993-1995 3 Annual Reports, 1975-2004 4 Annual Reports of Director of Public Health, 1989-2008 5 Year Books, 1977-1992 6 Internal Policy Documents and Reports, 1975-2005 7 Publications, 1960-2002 8 Administrative Papers, 1973-1994 8A Numbered Administrative Files, 1968-1993 8B Numbered Registry Files, 1970-1996 8C Unregistered Files, 1971-1997 8D Files of the Health Emergency Planning Officer, 1978-1993 9 Annual Financial Reviews, 1974-1987 10 Annual Accounts, 1976-1992 10A Requests for a major item of equipment, 1987-1990 LHB37 LOTHIAN HEALTH BOARD 11 Lothian Medical Audit Committee, 1988-1997 12 Records of the Finance Department, 1976-1997 13 Endowment Fund Accounts, 1972-2004 14 Statistical Papers, 1974-1990 15 Scottish Health Service Costs, 1975-1987 16 Focus on Health , 1982-1986 17 Lothian Health News , 1973-2001 18 Press -

8-12 Weeks Questionnaire
Scottish Government Maternal and Infant Nutrition Survey Investigating health care and early feeding choices and experiences in the first 12 weeks following the birth of your new baby This is a survey about your choices and experiences in the first 12 weeks following the birth of your new baby. Please complete this questionnaire with respect to your baby who was born between March and April 2017. The information you provide will help us to understand more about the choices new parents make and help health care professionals to better support new parents. All of the answers you provide will be entirely confidential. Please read the enclosed letter for more information about this survey. Instructions The survey takes around 15-20 minutes to complete. Please answer all questions, unless the instructions ask you to skip a question. For most questions, you will be asked to put a tick in the box next to the statement which most applies to you. For example, if your answer is yes, write in a tick as below: P Yes No Don’t worry if you make a mistake; just cross it out and tick the correct answer. Sometimes you will be asked to write in a number. Please enter numbers as figures rather than words. For example: 6 Weeks 2 Days If you prefer, you can complete this survey online at: survey.natcen.ac.uk/MINS5 You will be asked to enter the User Code that can be found on the letter that came with this survey. Alternatively, you can give your answers by calling the FREEPHONE survey helpline on 0800 652 4568. -

Family of Donald Bremner and Margaret Gunn. Latheron, CAI December 2Nd, 2015
Family of Donald Bremner and Margaret Gunn. Latheron, CAI December 2nd, 2015 Generation One 1. Donald Bremner #14801, b. c 1750? in Latheron?, CAI, SCT, occupation Weaver. He married Margaret Gunn #14802, 01 February 1774 in Latheron, CAI, SCT.1 Children: 2. i. George Bremner #14796 b. 1776. 3. ii. Ann Bremner #14810 b. April 1778. 4. iii. Mary Bremner #14803 b. 1780. 5. iv. Elizabeth Bremner #14838 b. 1784. 6. v. John Bremner #14839 b. 1786. 7. vi. James Bremner #14840 b. 1788. 8. vii. Margaret Bremner #14827 b. 1791. 9. viii. Donald Bremner #14806 b. 1795. Generation Two 2. George Bremner #14796, b. 1776 in Latheron, CAI, SCT,2 baptized 12 March 1776 in Latheron, CAI, SCT,3 d. 29 March 1862 in Achsinegar Swiney, Latheron, CAI,4 occupation 1851 Farmer of 3 acres. 1851-1861: At Achsinegar, Latheron. 1861: Farmed 12 acres. Noted as "Ground Officer" at time of death; parents names verified from death certificate. He married (1) Ann Henderson #14797, 08 June 1797 in Latheron, CAI, SCT,1 b. c 1775 in Latheron, CAI, SCT,2 (daughter of John Henderson #14799 [Blacksmith] and Margaret Sinclair #14800), d. 23 August 1857 in Achsinegar, Latheron, CAI, SCT.5 Ann: Ann is shown as blind in the 1851 census. Children: 10. i. John Bremner #14771 b. 1798. 11. ii. Donald Bremner #14833 b. 1799. 12. iii. Alexander McLean Bremner #14834 b. 1802. 13. iv. Margaret Bremner #14835 b. 1804. 14. v. Donald Bremner #14836 b. 1807. 15. vi. George Bremner #15931 b. c 1809. 16. vii. James Bremner #14846 b. -

SEVEN WOMEN of the 1967 REFERENDUM Project For
SEVEN WOMEN OF THE 1967 REFERENDUM Project for Reconciliation Australia 2007 Dr Lenore Coltheart There are many stories worth repeating about the road to the Referendum that removed a handful of words from Australia’s Constitution in 1967. Here are the stories of seven women that tell how that road was made. INTRODUCING: SHIRLEY ANDREWS FAITH BANDLER MARY BENNETT ADA BROMHAM PEARL GIBBS OODGEROO NOONUCCAL JESSIE STREET Their stories reveal the prominence of Indigenous and non-Indigenous women around Australia in a campaign that started in kitchens and local community halls and stretched around the world. These are not stories of heroines - alongside each of those seven women were many other men and women just as closely involved. And all of those depended on hundreds of campaigners, who relied on thousands of supporters. In all, 80 000 people signed the petition that required Parliament to hold the Referendum. And on 27 May 1967, 5 183 113 Australians – 90.77% of the voters – made this the most successful Referendum in Australia’s history. These seven women would be the first to point out that it was not outstanding individuals, but everyday people working together that achieved this step to a more just Australia. Let them tell us how that happened – how they got involved, what they did, whether their hopes were realised – and why this is so important for us to know. 2 SHIRLEY ANDREWS 6 November 1915 - 15 September 2001 A dancer in the original Borovansky Ballet, a musician whose passion promoted an Australian folk music tradition, a campaigner for Aboriginal rights, and a biochemist - Shirley Andrews was a remarkable woman. -

4.11 Chief Executive and Directors Report
NHS Highland Board 24 July 2018 Item 4.11 CHIEF EXECUTIVE AND DIRECTORS REPORT – EMERGING ISSUES AND UPDATES Report by Elaine Mead, Chief Executive The Board is asked to: • Note the updates provided in the report. Chief Officer Argyll and Bute Health and Social Care Partnership It is with much regret to report that Christina West has resigned from the post of Chief Officer for Argyll and Bute Health and Social Care Partnership with a leaving date of 30th September 2018. Integration of health and social care has been one of the most significant changes in the public sector for decades. Under Christina’s Leadership she leaves Argyll and Bute’s Health and Social Care Partnership in a positive position to move forward, with plans in place to redesign services not least to meet the demographic challenges. Christina takes with her our grateful thanks, for her hard work, determination and commitment to developing health and social care services for the people of Argyll and Bute. She embraced the Highland Quality Approach and has been an invaluable member of NHS Highland’s Senior Leadership team. The recruitment process is underway to secure a new Chief Officer. Dr Grays Temporary Service Model for Women and Children’s services A new temporary service model for Women and Children’s services at Dr Gray’s Hospital is to be put in place to allow maternity and paediatric service to continue in Elgin. The change comes after NHS Education for Scotland said initial indications were that only two trainee doctors had elected to work at Dr Gray’s at the next intake in August – six less than the number required. -

Item 5.07 Capital Plan
Highland NHS Board 14 April 2015 Item 5.7 FIVE YEAR CAPITAL PLAN & INDICATIVE TEN YEAR CAPITAL PLAN Report by Nick Kenton, Director of Finance The Board is asked to: • Approve the attached five year capital plan. 1 Background and Context Every year NHS Highland is required to submit a Capital Plan to the Scottish Government that sets out our proposed investment in our infrastructure for the coming five years. This year’s Plan includes an indicative ten-year look ahead. This Plan is set in the context of the Asset Management Strategy that was approved by the Board in August 2014 and the Ten Year Operational Implementation Plan that was approved by the Board in February 2015. This paper should also be read in tandem with the Local Delivery Plan paper elsewhere on this agenda. The Plan has been scrutinised in detail by the Asset Management Group (AMG), which is content to recommend it to the Board for formal approval. This Plan highlights all proposed capital expenditure on projects that are either planned or in progress. Also included is likely income form other sources such as disposal of assets no longer required. The Plan includes projects funded from traditional public sector capital (provided by the Scottish Government direct) as well as potential projects to be funded by up-front investment from out-with the public sector and paid for from revenue allocations. The plan should be seen in the context of continuing significant constraint on the NHSScotland capital position. Broadly, the Board’s capital plan is underpinned by four sources