World Bank Document
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

TAXON:Boswellia Sacra Flueck. SCORE:-3.0 RATING
TAXON: Boswellia sacra Flueck. SCORE: -3.0 RATING: Low Risk Taxon: Boswellia sacra Flueck. Family: Burseraceae Common Name(s): frankincense Synonym(s): Boswellia carteri Birdw. Assessor: Chuck Chimera Status: Assessor Approved End Date: 14 Jan 2021 WRA Score: -3.0 Designation: L Rating: Low Risk Keywords: Tree, Unarmed, Palatable, Self-Fertile, Wind-Dispersed Qsn # Question Answer Option Answer 101 Is the species highly domesticated? y=-3, n=0 n 102 Has the species become naturalized where grown? 103 Does the species have weedy races? Species suited to tropical or subtropical climate(s) - If 201 island is primarily wet habitat, then substitute "wet (0-low; 1-intermediate; 2-high) (See Appendix 2) High tropical" for "tropical or subtropical" 202 Quality of climate match data (0-low; 1-intermediate; 2-high) (See Appendix 2) High 203 Broad climate suitability (environmental versatility) y=1, n=0 y Native or naturalized in regions with tropical or 204 y=1, n=0 y subtropical climates Does the species have a history of repeated introductions 205 y=-2, ?=-1, n=0 ? outside its natural range? 301 Naturalized beyond native range y = 1*multiplier (see Appendix 2), n= question 205 n 302 Garden/amenity/disturbance weed n=0, y = 1*multiplier (see Appendix 2) n 303 Agricultural/forestry/horticultural weed n=0, y = 2*multiplier (see Appendix 2) n 304 Environmental weed n=0, y = 2*multiplier (see Appendix 2) n 305 Congeneric weed n=0, y = 1*multiplier (see Appendix 2) n 401 Produces spines, thorns or burrs y=1, n=0 n 402 Allelopathic 403 Parasitic y=1, n=0 n 404 Unpalatable to grazing animals y=1, n=-1 n 405 Toxic to animals y=1, n=0 n 406 Host for recognized pests and pathogens 407 Causes allergies or is otherwise toxic to humans y=1, n=0 n 408 Creates a fire hazard in natural ecosystems y=1, n=0 n 409 Is a shade tolerant plant at some stage of its life cycle y=1, n=0 n Tolerates a wide range of soil conditions (or limestone 410 y=1, n=0 n conditions if not a volcanic island) Creation Date: 14 Jan 2021 (Boswellia sacra Flueck.) Page 1 of 16 TAXON: Boswellia sacra Flueck. -

An Ecological Assessment of the Coastal Plains of North Western Somalia (Somaliland)
IUCN Eastern Africa Programme Somali Natural Resources Management Programme An Ecological Assessment of the Coastal Plains of North Western Somalia (Somaliland) Malte Sommerlatte and Abdi Umar May 2000 IUCN Eastern Africa Programme Somali Natural Resources Management Programme An Ecological Assessment of the Coastal Plains of North Western Somalia (Somaliland) By: Malte Sommerlatte and Abdi Umar IUCN CONSULTANTS May 2000 Table of Contents SUMMARY....................................................................................................................................... i ACKNOWLEDGEMENTS ................................................................................................................ iii 1. INTRODUCTION ....................................................................................................................... 1 1.1 OBJECTIVES OF ASSESSMENT ............................................................................................. 1 1.2 A REVIEW OF PREVIOUS STUDIES ...................................................................................... 1 1.3 SOCIAL STRUCTURES OF THE SOMALILAND COASTAL PLAINS PASTORALISTS ............... 3 1.4 LOCAL REGULATIONS CONTROLLING LAND USE AND NATURAL RESOURCES .............. 4 1.5 THE PRESENT POLITICAL SITUATION IN SOMALILAND..................................................... 6 2. SURVEY METHODS.................................................................................................................... 7 2.1. VEGETATION TRANSECTS.................................................................................................. -

SOMALIA History British and Italian Have Colonized Somalia Until The
SOMALIA History British and Italian have colonized Somalia until the coup d’etat in 1969 leaded by Mohamed Siad Barre. He was able to stabilize the country for a couple of decades before his government fell down in 1991. During that period, Somalia went through wars and anarchy. The northern clans of the Republic of Somaliland declared themselves independent in May 1991 but were not recognized by any government. They have tried to establish a stable and democratic government with parliamentary and presidential elections. The state of Puntland has also self governed since 1998, but did not declared themselves as independent. Their government suffered a civil war when Puntland tried to protect its borders with Somaliland. The UN tried to intervene by helping with the famine but after leaving the territory the situation has only gotten worse. The UN supported talks between the Transitional Federal Government (TFG) and the opposition Alliance for the Re-Liberation of Somalia (ARS) in 2008. A TFG-ARS unity government was created in January 2009, and Ethiopian forces withdrew from the country. Sheikh Sharif Sheikh Ahmed was elected as president on January 31, 2009 in Djibouti. Current and Interesting Facts: Capital: Mogadishu Official Languages: Somali and Arabic Government: Coalition Government. President: Sharif Ahmed. Economy: relies heavily on agriculture (bananas, sorghum, corn, coconuts, rice, sugarcane, mangoes, sesame seeds, beans) with livestock (cattle, sheep, goats, fish). The main industries include sugar refining, textiles, and wireless communication. Demography: about 9 millions of inhabitants. 85% are Somali, 15% are Bantu and other non-Somali (including Arabs). Religion: majority are Sunni Muslims. -

The Watson Files- the Key to Saving Somalia Is Gathering Dust in the British Countryside
The Watson Files- The Key to Saving Somalia is Gathering Dust in the British Countryside Feature What if there were a blueprint for climate adaptation that could end a civil war? An English scientist spent his life developing one — then he vanished without a trace. By Laura Heaton | Photographs by Nichole Sobecki | June 4, 2017 After sunrise on April 1, 2008, the renowned English ecologist Murray Watson left the Saakow Hotel, a modest concrete guesthouse in rural southern Somalia, heading off for work in a Nissan Patrol. He and a Kenyan colleague, an engineer named Patrick Amukhuma, along with a translator and two guards, were on their way to finish up a survey of flood-prone areas for the United Nations using an aerial and ground survey technique Watson had pioneered decades earlier. One of the more lush regions in a largely arid country, the area covered by Watson’s survey was also among the most hazardous. It was crawling with al-Shabab extremists, who had taken to extorting the banana and sugarcane farms that unfurled along the banks of the Shabelle and Jubba rivers. Increasingly erratic rainfall, a phenomenon scientists have linked to climate change, was further threatening the farms by causing frequent floods that Watson hoped his survey could help mitigate. Though the 69-year-old Englishman wouldn’t have described it as such, he was leading a groundbreaking climate adaptation effort in a country that is among the most vulnerable to climate change — and to the conflict that often follows in its wake. Watson knew the dangers of working in this region, but over the years he had honed a set of instincts that usually kept him out of harm’s way. -

SOMALIË Veiligheidssituatie in Somaliland En Puntland
COMMISSARIAAT-GENERAAL VOOR DE VLUCHTELINGEN EN DE STAATLOZEN COI Focus SOMALIË Veiligheidssituatie in Somaliland en Puntland 18 juni 2017 (update) Cedoca Oorspronkelijke taal: Nederlands DISCLAIMER: Dit COI-product is geschreven door de documentatie- en researchdienst This COI-product has been written by Cedoca, the Documentation and Cedoca van het CGVS en geeft informatie voor de behandeling van Research Department of the CGRS, and it provides information for the individuele asielaanvragen. Het document bevat geen beleidsrichtlijnen of processing of individual asylum applications. The document does not contain opinies en oordeelt niet over de waarde van de asielaanvraag. Het volgt de policy guidelines or opinions and does not pass judgment on the merits of richtlijnen van de Europese Unie voor de behandeling van informatie over the asylum application. It follows the Common EU Guidelines for processing herkomstlanden van april 2008 en is opgesteld conform de van kracht zijnde country of origin information (April 2008) and is written in accordance with wettelijke bepalingen. the statutory legal provisions. De auteur heeft de tekst gebaseerd op een zo ruim mogelijk aanbod aan The author has based the text on a wide range of public information selected zorgvuldig geselecteerde publieke informatie en heeft de bronnen aan elkaar with care and with a permanent concern for crosschecking sources. Even getoetst. Het document probeert alle relevante aspecten van het onderwerp though the document tries to cover all the relevant aspects of the subject, the te behandelen, maar is niet noodzakelijk exhaustief. Als bepaalde text is not necessarily exhaustive. If certain events, people or organisations gebeurtenissen, personen of organisaties niet vernoemd worden, betekent are not mentioned, this does not mean that they did not exist. -
TM March 10, 2017
THE JAMESTOWN FOUNDATION MARCH 10, 2017 VOLUME XV, ISSUE 5 p.1 p.3 p.5 p.7 Alexander Sehmer Animesh Roul Rafid Jaboori Michael Horton BRIEFS Myanmar’s Muslim In- Islamic State’s Deir al- Al-Shabaab: Why Soma- surgency Gaining Zour Offensive Puts lia’s al-Qaeda Affiliate Prominence With Ji- the Syrian Regime Wants Puntland hadist Groups Under Pressure SOMALIA: ONE STEP CLOSER TO DEFEATING AL- told politicians and diplomats that the group could be SHABAAB broken in the next two years (Horseed Media, February 19). Despite this, his pre-election appeal to al-Shabaab Alexander Sehmer has not been entirely forgotten. In the build up to his election as Somalia’s president, Al-Shabaab, meanwhile, has vowed its fight against the Mohamed Abdullahi Mohamed announced he would United Nations-backed government will continue, invite al-Shabaab for a “sit down and discussion” (Twit- branding Farmaajo, who has dual U.S. and Somali citi- ter, January, 28). His rhetoric toward the group since zenship, an “American puppet” (Mareeg, February 27). then has been less welcoming. The new president, known as Farmaajo, appears confident that he could be The group continues to menace the country. There have the one to bring an end to the al-Qaeda affiliate’s vio- been several attacks in Mogadishu, and this month mili- lent insurgency. Indeed, there is much that is in his favor. tants seized the town of El Baraf in the Middle Shabelle region as the army and African Union (AU) forces pulled Farmaajo was elected by legislators in the second round back (Garowe Online, March 8). -

European Union Training Mission Somalia
European Union Training Mission Somalia PRESS SUMMARY 28th July 2018 “In ‘Media’ stat virtus” EUTM - SOMALIA 28/07/2018 SUMMARY TITLE PAGE SNA Kills Several Al-Shabaab Fighters In Southern Somalia 2 A Former Lawmaker Shot Dead In Mogadishu 3 Islamist leader, 5 others killed in Somalia fighting 4 Puntland security officer killed in Galkayo 5 Cabinet Approves Replacement Of Mogadishu Stabilization Force By 6 Civil Defence Forces Somali President to visit Eritrea’s capital, Asmara 7 Eritrea says leader of Somalia, another rival, to visit 8 Somalia protests against Kenya after Elwak attack 9 Outgoing Ugandan Troops Receive Service Medals 10 Somali Military Court Sentences ISIS Linked Man Life Imprisonment 11 PM Khaire Receives Educational Experts Who Attended Recent 12 Education Conference In Mogadishu Dadaab refugees get food aid after UN cuts funding 13 Somaliland eyes key Red Sea trade role with Berbera port 14 12 Interesting Facts About Somalia (The Land of Pirates!) 17 US Counterterrorism strikes: Tempo remains high in Somalia and 21 Yemen, transparency improves UAE ready to take on greater security burden in Middle East 25 EUTM - SOMALIA 1 EUTM - SOMALIA 28/07/2018 SNA Kills Several Al-Shabaab Fighters In Southern Somalia 27 July 2018 Several Al-Shabaab fighters have been killed in a battle with Somali soldiers in Bay region. The soldiers raided the militia group’s camp on Thursday, forcing a number of the Al- Shabaab fighters to abandon their camp, according to Southwest state spokesperson, Nuradin Yussuf Ga’ma. Ga’ma, who spoke to the media, said among those killed were two Al-Shabaab ringleaders: “During the operations, the government forces killed several Al-Shabaab members. -

Download De COI Focus
COMMISSARIAAT-GENERAAL VOOR DE VLUCHTELINGEN EN DE STAATLOZEN COI Focus SOMALIË Veiligheidssituatie in Somaliland en Puntland 24 april 2018 (update) Cedoca Oorspronkelijke taal: Nederlands DISCLAIMER: Dit COI-product is geschreven door de documentatie- en researchdienst This COI-product has been written by Cedoca, the Documentation and Cedoca van het CGVS en geeft informatie voor de behandeling van Research Department of the CGRS, and it provides information for the individuele asielaanvragen. Het document bevat geen beleidsrichtlijnen of processing of individual asylum applications. The document does not contain opinies en oordeelt niet over de waarde van de asielaanvraag. Het volgt de policy guidelines or opinions and does not pass judgment on the merits of richtlijnen van de Europese Unie voor de behandeling van informatie over the asylum application. It follows the Common EU Guidelines for processing herkomstlanden van april 2008 en is opgesteld conform de van kracht zijnde country of origin information (April 2008) and is written in accordance with wettelijke bepalingen. the statutory legal provisions. De auteur heeft de tekst gebaseerd op een zo ruim mogelijk aanbod aan The author has based the text on a wide range of public information selected zorgvuldig geselecteerde publieke informatie en heeft de bronnen aan elkaar with care and with a permanent concern for crosschecking sources. Even getoetst. Het document probeert alle relevante aspecten van het onderwerp though the document tries to cover all the relevant aspects of the subject, the te behandelen, maar is niet noodzakelijk exhaustief. Als bepaalde text is not necessarily exhaustive. If certain events, people or organisations gebeurtenissen, personen of organisaties niet vernoemd worden, betekent are not mentioned, this does not mean that they did not exist. -
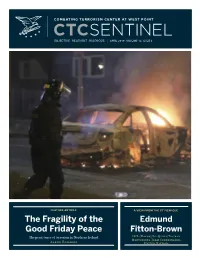
CTC Sentinel Welcomes Submissions
OBJECTIVE ·· RELEVANT ·· RIGOROUS || JUNE/JULYAPRIL 2019 2018 · VOLUME · VOLUME 12, ISSUE 11, ISSUE 4 6 FEATURE ARTICLE A VIEW FROM THE CT FOXHOLE The FragilityJihadi Threat of the Edmund LTC(R) Bryan Price Good Friday Peace Fitton-Brown to Indonesia ISIL (Daesh)/Al-Qaida/Taliban The persistence of terrorism in Northern Ireland Former Director, Monitoring Team Coordinator, Combating Terrorism Center KirstenAaron E.Edwards Schulze United Nations FEATURE ARTICLE Editor in Chief 1 The Fragility of the Good Friday Peace: The Persistence of Terrorism in Northern Ireland Paul Cruickshank Aaron Edwards Managing Editor Kristina Hummel INTERVIEW 7 A View from the CT Foxhole: Edmund Fitton-Brown, Coordinator, EDITORIAL BOARD ISIL (Daesh)/Al-Qaida/Taliban Monitoring Team, United Nations Paul Cruickshank Colonel Suzanne Nielsen, Ph.D. Department Head ANALYSIS Dept. of Social Sciences (West Point) 16 Profit-Minded Suppliers: The WMD Pathways and Combating Convergence Brian Dodwell Stephen Hummel, Douglas McNair, F. John Burpo, and Director, CTC James Bonner Don Rassler 22 Doxing and Defacements: Examining the Islamic State's Hacking Capabilities Audrey Alexander and Bennett Clifford Director of Strategic Initiatives, CTC 29 Reigniting the Rivalry: The Islamic State in Somalia vs. al-Shabaab Caleb Weiss CONTACT Combating Terrorism Center U.S. Military Academy The murder earlier this month of journalist Lyra McKee in Northern Ire- land on the night before Good Friday illustrates the fragility of peace in a 607 Cullum Road, Lincoln Hall region in which -

European Union Training Mission Somalia
European Union Training Mission Somalia PRESS SUMMARY 20th April 2018 “In ‘Media’ stat virtus” EUTM - SOMALIA 20/04/2018 Somali National Army conduct operation in some areas in Central Somalia Apr 19, 2018 Mogadishu(SONNA)-Somali National Army on Thursday conducted operations at Camara and Bacad-weyne areas in Mudug region to fight against the militant group of Al-Shabaab, SONNA reported. ”Operations are aimed at to liberate terrorist militants hiding out in those locations, Somali National Army will continue until all areas under the terrorists’ control are completely managed to take control and secure them”, Army Commander in the area, Abdulahi Aden Hassan told SONNA. Such military operations are also taking place in some areas in Hiiraan and Middle Shabelle regions according to the military officials. http://sonna.so/en/?p=13061 EUTM - SOMALIA 1 EUTM - SOMALIA 20/04/2018 AMISOM convenes humanitarian facilitation training for civilian partners in Somalia’s HirShabelle state Apr 19, 2018 - Jowhar(SONNA)-The African Union Mission in Somalia (AMISOM) held a one-day training for partners in Jowhar, the administrative capital of HirShabelle state, to familiarize them with the Somalia Country Specific Humanitarian Civil- Military Guidelines, which guides the interaction between partners and the Mission. “Humanitarian challenges call for increased coordination and dialogue between AMISOM and partners operating in the recovered areas,” said Abdul Diabagate, AMISOM’s Senior Humanitarian Liaison Officer, during the highly interactive sessions. Diabagate expressed the need to increase humanitarian facilitation activities and interaction with communities in areas undergoing acute crises and natural disasters. The training aimed at fostering partnerships between AMISOM civilian liaison officers and the partners, also sensitized participants on the importance of observing the International Humanitarian Law, humanitarian principles and International Refugee Law. -

The Milk of the Boswellia Forests: Frankincense Production Among the Pastoral Somali
/ 1 THE MILK OF THE BOSWELLIA FORESTS: FRANKINCENSE PRODUCTION AMONG THE PASTORAL SOMALI Ahmed Yusuf Farah Submitted in fulfillment of the requirements for the degree of Doctor of Philosophy of the University of London at the London School of Economics and Political Science December 1988 2 ABSTRACT The thesis is a study of the 'ownership', production and marketing of frankincense in Somalia. It considers first the various local and wider uses of frankincense, both industrial and non-industrial. It then examines the place of frankincense trees in the general classification of property in Somalia, with further consideration of the dominance of pastoral concepts in the frankincense sector and sedentary cultivation in northern Somalia. The thesis also analysis the organisation and social relations of frankincense production prior to 1969, and examines the subsequent transformations which have followed the introduction of cooperatives in this sector of the Somali economy. 3 CONTENTS List of Figures and Tables 5 ACKNOWLEDGEMENTS 6 INTRODUCTION 8 CHAPTER ONE: SOMALIA AND THE FRANKINCENSE TRADE Major Types of Frankincense and their Source 13 Marketing Policies of Previous Governments 18 Aden Market 22 Organisation of Marketing in Somalia Today 40 International Trade 47 CHAPTER TWO: NON-INDUSTRIAL USES OF INCENSE IN SOMALIA AND ELSEWHERE Social Organisation of the Somali 62 Local Thoughts about the Industrial Use of Incense 71 Some Practical Uses of Frankincense 72 Fumigation and Purification 77 Medicinal Uses of Frankincense 83 Medicinal Use -

P14 Layout 1
MONDAY, DECEMBER 26, 2016 ANALYSIS THE LEADING INDEPENDENT DAILY IN THE ARABIAN GULF ESTABLISHED 1961 Founder and Publisher YOUSUF S. AL-ALYAN Editor-in-Chief ABD AL-RAHMAN AL-ALYAN EDITORIAL : 24833199-24833358-24833432 ADVERTISING : 24835616/7 FAX : 24835620/1 CIRCULATION : 24833199 Extn. 163 ACCOUNTS : 24835619 COMMERCIAL : 24835618 P.O.Box 1301 Safat,13014 Kuwait. E MAIL :[email protected] Website: www.kuwaittimes.net Focus Icahn regulatory role gives activist investors voice S chief executives, already wrestling with a steady flow of activist investors in their board Urooms, face a newly challenging landscape now that the loudest voice of the bunch will have the ear of the next president and his securities’ rule mak- ers. The advisory role granted to billionaire investor Carl Icahn by President-elect Donald Trump is a poten- tial blow to CEOs and board directors who hoped the new Securities and Exchange Commission would favor corporate management teams over shareholder proposals that they deem too friendly to shareholders. Icahn’s appointment, announced on Wednesday, spans all regulatory matters. That includes vetting SEC candidates, a significant boost to shareholder activists who want commissioners to keep corporate gover- Venezuela claim unlikely to convince US nance initiatives on the front burner. While Icahn has spent four decades antagonizing CEOs and boards, the extent of his Washington influence and where he legal strategy switch by Venezuela’s state-owned about alleged malfeasance. “It’s possible this will come break during a 2002-2003 oil strike against late leader will lean on shareholder issues remains to be seen. oil giant PDVSA to portray itself as a victim in a back to haunt PDVSA,” said Mike Koehler, an FCPA expert Hugo Chavez when Rincon’s main firm Tradequip Services Still, it is clear that holding the feet of executives and Amassive bribery scheme detected by the US gov- at Southern Illinois University school of law.