2016 Stamford Hospital Community Health Needs Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
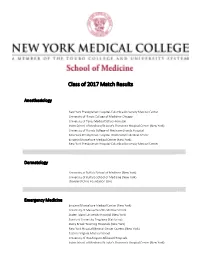
2017 Match Day Results by Program
Class of 2017 Match Results Anesthesiology New York Presbyterian Hospital-Columbia University Medical Center University of Illinois College of Medicine-Chicago University of Texas Medical School-Houston Icahn School of Medicine/St Luke's-Roosevelt Hospital Center (New York) University of Florida College of Medicine-Shands Hospital New York Presbyterian Hospital-Weill Cornell Medical Center Einstein/Montefiore Medical Center (New York) New York Presbyterian Hospital-Columbia University Medical Center Dermatology University at Buffalo School of Medicine (New York) University of Buffalo School of Medicine (New York) Cleveland Clinic Foundation (OH) Emergency Medicine Einstein/Montefiore Medical Center (New York) University of Massachusetts Medical School Staten Island University Hospital (New York) Stanford University Programs (California) Stony Brook Teaching Hospitals (New York) New York Hospital Medical Center Queens (New York) Eastern Virginia Medical School University of Washington Affiliated Hospitals Icahn School of Medicine/St Luke's-Roosevelt Hospital Center (New York) University of Connecticut School of Medicine Rhode Island Hospital/Brown University Wake Forest Baptist Medical Center (North Carolina) Icahn School of Medicine/St Luke's-Roosevelt Hospital Center (New York) Einstein/Montefiore Medical Center (New York) Oregon Health and Science University Dartmouth-Hitchcock Medical Center (New Hampshire) Einstein/Montefiore Medical Center (New York) University of Washington Affiliated Hospitals Einstein/Montefiore Medical Center -
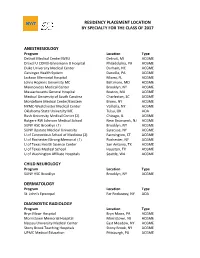
Residency Placement Location by Specialty for the Class of 2017
RESIDENCY PLACEMENT LOCATION BY SPECIALTY FOR THE CLASS OF 2017 ANESTHESIOLOGY Program Location Type Detroit Medical Center/WSU Detroit, MI ACGME Drexel U COM/Hahnemann U Hospital Philadelphia, PA ACGME Duke University Medical Center Durham, NC ACGME Geisinger Health System Danville, PA ACGME Jackson Memorial Hospital Miami, FL ACGME Johns Hopkins University MC Baltimore, MD ACGME Maimonides Medical Center Brooklyn, NY ACGME Massachusetts General Hospital Boston, MA ACGME Medical University of South Carolina Charleston, SC ACGME Montefiore Medical Center/Einstein Bronx, NY ACGME NYMC-Westchester Medical Center Valhalla, NY ACGME Oklahoma State University MC Tulsa, OK AOA Rush University Medical Center (2) Chicago, IL ACGME Rutgers-RW Johnson Medical School New Brunswick, NJ ACGME SUNY HSC Brooklyn (3) Brooklyn, NY ACGME SUNY Upstate Medical University Syracuse, NY ACGME U of Connecticut School of Medicine (2) Farmington, CT ACGME U of Rochester/Strong Memorial (3) Rochester, NY ACGME U of Texas Health Science Center San Antonio, TX ACGME U of Texas Medical School Houston, TX ACGME U of Washington Affiliate Hospitals Seattle, WA ACGME CHILD NEUROLOGY Program Location Type SUNY HSC Brooklyn Brooklyn, NY ACGME DERMATOLOGY Program Location Type St. John’s Episcopal Far Rockaway, NY AOA DIAGNOSTIC RADIOLOGY Program Location Type Bryn Mawr Hospital Bryn Mawr, PA ACGME Morristown Memorial Hospital Morristown, NJ ACGME Nassau University Medical Center East Meadow, NY ACGME Stony Brook Teaching Hospitals Stony Brook, NY ACGME UPMC Medical Education -

2019 Greater Bridgeport Region Bridgeport Hospital and St. Vincent's Medical Center Collaborative Community Health Needs Asse
2019 Greater Bridgeport Region Bridgeport Hospital and St. Vincent’s Medical Center Collaborative Community Health Needs Assessment and Implementation Plan By the Health Improvement Alliance This document is a special section of the Fairfield County Community Wellbeing Index 2019, a core program of DataHaven (ctdatahaven.org), in partnership with Fairfield County’s Community Foundation and a Community Health Needs Assessment for the towns served by all Fairfield County hospitals including Bridgeport Hospital and St. Vincent’s Medical Center 1 | Page ABOUT THIS REPORT This document is a special section of the Fairfield County Community Wellbeing Index 2019 (Appendix A), a comprehensive report about Fairfield County and the towns within it. The Community Index was produced by DataHaven in partnership with Fairfield County’s Community Foundation and many other regional partners, including the Health Improvement Alliance (HIA), a coalition serving towns in the Greater Bridgeport region. This document serves as the Community Health Needs Assessment for the six towns in the HIA area (Bridgeport, Easton, Fairfield, Monroe, Stratford, and Trumbull). The Community Health Needs Assessment documents the process that the HIA used to conduct the regional health assessment and health improvement activities. You may find the full Community Wellbeing Index attached to this section, or posted on the DataHaven, Fairfield County’s Community Foundation, Bridgeport Hospital, St. Vincent’s Medical Center, or any of the town health department websites. The Community Health Needs Assessment and Community Health Improvement Plan were approved by the Board of Trustees for St. Vincent’s Medical Center in June 13, 2019 and the Board of Trustees for Bridgeport Hospital in July 9, 2019. -

Norwalk Community Food Report
Norwalk Community Food Report January 2020 Prepared and Presented by: Fairfield University’s Center for Social Impact Norwalk Health Department Additional Data Analysis provided by: CT Food Bank Research Team: Director of Center for Social Impact: Melissa Quan Research Coordinator: Jonathan Delgado Student Researcher: Mahammad Camara ‘19 Editors: Sophia Gourgiotis Luckario Alcide Eileen Michaud Research Partners: Norwalk Health Department Health Educator: Theresa Argondezzi Food Access Project Coordinator: Pamela Flausino Melo da Silva Additional Data Resources Made Available by CT Food Bank: Jamie Foster, PhD Acknowledgments Center for Social Impact 4 Healthy for Life Project 5 Project Overview 6 How To Use This Report 7 Norwalk Food Agencies 8 Norwalk Maps And Tables Food Insecurity 9 Populations Children 12 Immigrant (Foreign Born) Population 14 Seniors 16 Single Parent/Guardian 18 Services Disability 20 Free & Reduced-Price Lunch 22 SNAP & WIC 24 Social Determinants Educational Attainment 28 Housing Burden 32 Transportation 34 Unemployment 36 Key Findings 38 Taking Action: Norwalk Food Access Initiative 39 Appendix A: Census Boundary Reference Map 41 Appendix B: Population Density Table 42 Appendix C: SNAP & WIC Retailers 43 Appendix D: SNAP & WIC Information 45 Appendix E: Data Source Tables 46 Glossary 47 References 48 TABLE OF Contents Page 3 of 50 Center for Social Impact The Center for Social Impact was founded in 2006 with the goal of integrating the Jesuit, Catholic mission of Fairfield University, which includes a commitment to service and social justice, through the academic work of teaching and research. The Center for Social Impact has three major programs: 1. Community-Engaged Learning (formerly known as Service Learning) 2. -

1 TRACYLAIN EVANS, RN, MS, MPH, MBA, EMT/P 277 Fillow Street
1 TRACYLAIN EVANS, RN, MS, MPH, MBA, EMT/P 277 Fillow Street Norwalk, CT 06850 [email protected] 203-524-5558 SUMMARY Experienced professional healthcare leader with over 30 years of clinical leadership experience in management, education, nursing and emergency services and 40 in care delivery. Demonstrated progressive growth from flight nurse/paramedic, to acute care nurse practitioner, and leader. Focusing on prevention, population health, social determinants, and engaging patients in self-directed care to reduce. Experience with stakeholder engagement, process management, and performance improvement. EDUCATION Chamberlain University, Chicago, IL DNP – Nursing Leadership 2020 Pace University, White Plains, NY MBA - Strategic Management 2006 Columbia University, New York, NY MS – Nurse Practitioner 2000 New York Medical College, Valhalla, NY MPH - Public Health 2000 Pace University, Pleasantville, NY BSN - Nursing 1995 Norwalk Community College, CT EMT-P - Paramedic 1992 University of Denver, Denver, CO BS - Business Administration 1987 WORK HISTORY St Joseph’s University Medical Center – Paterson, NJ (2019 – present) Trauma Program Manager o Support a team of Trauma/Critical Care Surgeons o Lead a team of 6 clinical and administrative trauma professionals o Evaluate effectiveness of Performance Improvement process o Financial responsibility for annual budget, payroll, and human resources o Develop Outreach/Inreach program o Course Director and Faculty for trauma educational programs o Project Lead: Hospital-Linked Violence Intervention -

Norwalk Hospital Chooses Dräger for a Comprehensive Anesthesia Solution
Norwalk Hospital Chooses Dräger for a Comprehensive Anesthesia Solution At Norwalk Hospital, clinicians are reaping the benefits of a multi-tiered platform in one, user-friendly format. D-12409-2011 When Eric Kitain, MD, of Norwalk Hospital rooms and obstetrical suites where general About Norwalk Hospital in Norwalk, Connecticut sought to replace anesthesia is less often required; and his department‘s anesthesia equipment, he Fabius Tiro®, a compact, feature-rich Norwalk Hospital is a not-for-profit, acute had several ambitious safety, quality and option for anesthesia in remote locations care, community teaching hospital in financial goals to achieve. “We needed such as Endoscopy and Radiology (see Fairfield County, Connecticut. Hospital machines at various performance levels sidebar). The three-tiered system allowed services include oncology; an emergency corresponding to the requirements of our the hospital to get the level of care and level-2 trauma care; in- and outpatient in- and outpatient settings,” says Dr. Kitain. required while minimizing expenditure. ambulatory surgery; diagnosis and “We also wanted some standardization treatment of sleep disorders; hyperbaric among these machines so that if users In addition, the choice equipped the hospital medicine; in- and outpatient psychiatric were trained on one, they could use them with a range of devices incorporating the services; and in- and outpatient addiction all. To meet these needs, we looked for latest ventilation and gas delivery technology rehabilitation. one vendor who could provide machines at — all with the same familiar user interface. multiple platform levels. We also knew that “This is a huge safety issue because it FY 2007 using a single vendor would allow us to allows us to respond effectively during Licensed Beds: 328 negotiate a better service contract and a emergency and critical care situations,” Emergency Department visits: 48,715 better, more cost-effective deal.” says Dr. -

Medical Staff News Newsletter for the Medical Staff of Bridgeport Hospital | January 2018
Medical Staff News Newsletter for the Medical Staff of Bridgeport Hospital | January 2018 From the Medical Staff Office that was due in large part to receiving the Medicaid funds that were in doubt for much of the year. Happy New Year! If you have seen the new Newborn ICU, you know how I thought I would start off with good news. I have started important the infrastructure updates are to our patients to talk about our performance on what I consider to be the and staff. It is magnificent! best quality measures: the Centers for Medicare & Medicaid I also wanted to let everyone know that Robert Folman, Services’ 30-day mortality measures. MD, is retiring from the medical staff. Bob has been the We are statistically better than the national average in three driving force behind the growth and development of the of six categories: acute myocardial infarction, heart failure cancer services we have provided at Bridgeport Hospital. and pneumonia. We are average for stroke, coronary artery In addition to that, he also stepped up for the hospital in bypass grafting and chronic obstructive pulmonary disease. a time of need and assumed the presidency of the Medical Only 10 percent of hospitals are better than average on Staff Executive Committee. Bob has improved not just the one measure. Only 48 hospitals nationwide, or 1.2 percent, lives of his patients, but also the lives of all the patients are better than average in three or more categories. Our who came here with cancer. His efforts didn’t just improve peer group includes Massachusetts General Hospital, the cancer care, they made us a better hospital! He is going to Cleveland Clinic and the Mayo Clinic in Scottsdale. -

The Following Is a List of Hospitals in Connecticut. Included Are Phone Numbers, Emergency Room Phone Numbers and Driving Directions
The following is a list of hospitals in Connecticut. Included are phone numbers, Emergency Room phone numbers and driving directions. Table of Contents BACKUS HOSPITAL ........................................................................................................2 BRIDGEPORT HOSPITAL - TRAUMA CENTER........................................................3 BRADLEY MEMORIAL HOSPITAL ...............................................................................4 BRISTOL HOSPITAL .......................................................................................................4 CHARLOTTE HUNGERFORD HOSPITAL ....................................................................5 CONNECTICUT CHILDREN'S MEDICAL CENTER ....................................................6 DANBURY HOSPITAL ....................................................................................................7 DAY KIMBALL HOSPITAL.............................................................................................7 GREENWICH HOSPITAL.................................................................................................8 GRIFFIN HOSPITAL .........................................................................................................8 HARTFORD HOSPITAL – TRAUMA CENTER............................................................9 HOSPITAL OF SAINT RAPHAEL .................................................................................10 JOHNSON MEMORIAL HOSPITAL..............................................................................11 -

Bridgeport Hospital Medical Staff News for January 2020
Medical Staff News Newsletter for the Medical Staff of Bridgeport Hospital | January 2020 From the desk of the CMO U.S. News & World Report voting begins Happy New Year! in February With the end of the calendar year, I tend to reflect on major All board-certified physicians within each of the applicable events, and 2019 was a big year for Bridgeport Hospital. Most specialties evaluated by U.S. News & World Report (i.e., notably, our medical staff expanded significantly as members Cancer, Cardiology/CT Surgery, Diabetes/Endocrinology, of the Milford Hospital Medical Staff integrated into a single ENT, Gastroenterology/GI Surgery, Geriatrics, Gynecology, Bridgeport Hospital Medical Staff across two campuses. As Nephrology, Neurology/Neurosurgery, Ophthalmology, Mike Ivy assumed the role of associate chief medical officer Orthopedics, Psychiatry, Pulmonary, Rehabilitation, for YNHHS, Anne Diamond joined Bridgeport as our Rheumatology and Urology) will soon receive a request to president. As Tito Vasquez moves into the role of president vote in the U.S. News reputation ranking. of the medical staff, I want to share my appreciation to The request will come via email from Doximity, an online Ken Lipow for his two years serving in that role. networking website for physicians used to calculate the The end of the year is also the time that I contemplate how reputational portion of the hospital rankings. Registered much CME I’ve completed in the year. In addition to events users may also receive a prompt when logging into the such as the Physician Summit and numerous departmental site. As the U.S. News & World Report rankings are heavily Grand Rounds that offer CME, I want to make sure you weighted towards an institution’s reputation, the survey know that Yale CME is available to all Bridgeport Hospital provides the opportunity for members of the medical staff Medical Staff. -

Bridgeport Hospital Medical Staff News | February 2020
Medical Staff News Newsletter for the Medical Staff of Bridgeport Hospital | February 2020 From the desk of the CMO YNHHS educates public about I’d like to open my final message as Bridgeport Hospital the coronavirus interim chief medical officer with gratitude – to you. It has News of the coronavirus, called the 2019 Novel Coronavirus been an honor to get to know you and work closely with or COVID-19, has prompted concern about risk of you during my 16 years at Bridgeport Hospital. Above all, I transmission in the United States. Although influenza deeply value the trusting relationships we have built over the viruses and coronaviruses have similar symptoms, the risk years. The partnership between my team and the medical of catching the flu in the U.S. remains far greater. staff officers, medical executive committee and all those they represent has been very meaningful as well as impactful. The COVID-19 is associated with mild-to-severe respiratory illness with fever and cough. Healthcare associated spread We have so much to be proud of. We are a much larger, of COVID-19 has been identified. Medical staff have been more diverse medical staff, having grown in primary care advised that patients who may be at risk for COVID-19 as well as specialties. Our intersection with Yale New Haven infection must be identified upon presentation to allow rapid Hospital’s medical staff is now very significant, and within isolation and use of proper personal protective equipment. the past year alone, we have been joined by more than 1. -

Planetree Partners CERTIFICATION* ORGANIZATION LOCATION
Planetree Partners CERTIFICATION* ORGANIZATION LOCATION CIMED Argentina Hospital Universitario Austral Argentina Centro de Rehabilitacion Quantum Argentina Hospital Universitario Austral Argentina Paseo Champagnat Argentina Sede Escobar Argentina Sede Lujan Argentina Sede Officia Argentina Sede San Miguel Argentina Aurrum Australia Aurrum – Healesville Australia Aurrum – Reservoir Australia Children’s Health Queensland Hospital and Health Service Australia Child and Youth Community Health Service Australia Child and Youth Mental Health Service Australia Lady Cilento Children’s Hospital Australia Logan Central Community Health Centre Australia Metro South Health Australia Beaudesert Hospital Australia Beenleigh Community Health Centre Australia Browns Plains Community Health Centre Australia Corinda Community Health Centre Australia Eight Mile Plains Community Health Centre Australia WWW.PLANETREE.ORG 1 Planetree Partners CERTIFICATION* ORGANIZATION LOCATION Inala Community Health Centre Australia Logan Hospital Australia Marie Rod Community Health Centre Australia Princess Alexandra Hospital Australia Queen Elizabeth II Jubilee Hospital Australia Redland Community Health Centre Australia Redland Hospital Australia Wynnum Community Health Centre Australia Associação De Assistência A Criança Deficiente (AACD) Brazil Hospital Anchieta Brazil Hospital Marcelino Champagnat Brazil Hospital Mater Dei SA Brazil Mãe de Deus (Mother of God Hospital) Brazil Moinhos de Vento Hospital Brazil Sociedade Beneficente Israelita Brasileira Albert Einstein -

Greenwich to Westport Guide for Mental Health and Substance
Children's Services (ages 0-18) ( O )UTPATIENT; ( I )NPATIENT; ( H )OME ( O )UTPATIENT; ( I )NPATIENT; ( D )ETOX; INTENSIVE (IOP) Child Guidance of Mid-Fairfield County (O)..………….................................203-299-1315 Norwalk Substance Use Access Line………………………………800-563-4086 Statewide Child Guidance of Southern CT (O)…………………................................203-324-6127 Stamford Circle Care (O) (specializing in LGBTQ) ………………………………………………………..203-852-9525 Norwalk 203-983-5294 Greenwich Community Health Center, Franklin Street Center (O)……………………….……….203-969-0802 Stamford 203-662-9380 Darien CT Counseling Centers, Inc (O, IOP)………………………........................................203-838-6508 Norwalk 203-324-6127 New Canaan Opening March 1st Stamford Community Health Center, Day Street Center (O)…………………………...................203-854-9292 Norwalk CT Renaissance, Inc (O, IOP)……………………………............................203-866-2541 Various CT Renaissance (O, H, IOP)……………………………………………..203-866-2541 Various Family & Children's Agency (Project Reward) (O,IOP)..........................................203-523-5790 Norwalk Family and Children's Agency (O)…………………………………..……………….............203-855-8765 Norwalk Greenwich Hospital Addiction Recovery Center (I, O, IOP, D)...................................203-863-4673 Greenwich Family Centers, Inc. (O).………………………………………...………………….................203-324-3167 Stamford Liberation Programs, Inc…………………………………………….. 203-869-4848 Greenwich Adult (I, O).........................................................................................203-851-2077