NATURAL DISASTERS: Protecting the Public's Health
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adversus Paganos: Disaster, Dragons, and Episcopal Authority in Gregory of Tours
Adversus paganos: Disaster, Dragons, and Episcopal Authority in Gregory of Tours David J. Patterson Comitatus: A Journal of Medieval and Renaissance Studies, Volume 44, 2013, pp. 1-28 (Article) Published by Center for Medieval and Renaissance Studies, UCLA DOI: 10.1353/cjm.2013.0000 For additional information about this article http://muse.jhu.edu/journals/cjm/summary/v044/44.patterson.html Access provided by University of British Columbia Library (29 Aug 2013 02:49 GMT) ADVERSUS PAGANOS: DISASTER, DRAGONS, AND EPISCOPAL AUTHORITY IN GREGORY OF TOURS David J. Patterson* Abstract: In 589 a great flood of the Tiber sent a torrent of water rushing through Rome. According to Gregory of Tours, the floodwaters carried some remarkable detritus: several dying serpents and, perhaps most strikingly, the corpse of a dragon. The flooding was soon followed by plague and the death of a pope. This remarkable chain of events leaves us with puzzling questions: What significance would Gregory have located in such a narrative? For a modern reader, the account (apart from its dragon) reads like a descrip- tion of a natural disaster. Yet how did people in the early Middle Ages themselves per- ceive such events? This article argues that, in making sense of the disasters at Rome in 589, Gregory revealed something of his historical consciousness: drawing on both bibli- cal imagery and pagan historiography, Gregory struggled to identify appropriate objects of both blame and succor in the wake of calamity. Keywords: plague, natural disaster, Gregory of Tours, Gregory the Great, Asclepius, pagan survivals, dragon, serpent, sixth century, Rome. In 589, a great flood of the Tiber River sent a torrent of water rushing through the city of Rome. -

The Year That Shook the Rich: a Review of Natural Disasters in 2011
THE YEAR THAT SHOOK THE RICH: A REVIEW OF NATURAL DISASTERS IN 2011 The Brookings Institution – London School of Economics Project on Internal Displacement March 2012 Design: [email protected] Cover photo: © Thinkstock.com Back cover photos: left / © Awcnz62 | Dreamstime.com; right / © IOM 2011 - MPK0622 (Photo: Chris Lom) THE YEAR THAT SHOOK THE RICH: A REVIEW OF NATURAL DISASTERS IN 2011 By Elizabeth Ferris and Daniel Petz March 2012 PUBLISHED BY: THE BROOKINGS INSTITUTION – LONDON SCHOOL OF ECONOMICS PROJECT ON INTERNAL DISPLACEMENT Bangkok, Thailand — Severe monsoon floods, starting in late July 2011, affected millions of people. A truck with passengers aboard drives through a heavily flooded street. Photo: UN/Mark Garten TABLE OF CONTENTS Acronyms ................................................................................................................................. vi Foreword ................................................................................................................................. ix Executive Summary ................................................................................................................. xi Introduction .............................................................................................................................. xv Chapter 1 The Year that Shook the Rich ...................................................... 1 Section 1 Disasters in the “Rich” World, Some Numbers ............................................ 5 Section 2 Japan: The Most Expensive Disaster -
Psychological Issues in Escape, Rescue, and Survival in the Wake of Disaster
2008 Psychological Issues in Escape, Rescue, and Survival in the Wake of Disaster Report Submitted to the National Institute of Occupational Safety and Health, Pittsburgh Research Laboratory George S. Everly, Jr., PhD, ABPP Paul Perrin & George S. Everly, III Contents INTRODUCTION THE PSYCHOLOGICAL IMPACT OF CRISIS AND DISASTERS The Nature of Human Stress Physiology of Stress Psychology of Stress Excessive Stress Distress Depression Posttraumatic Stress Disorder (PTSD) Compassion Fatigue A Review of Empirical Investigations on the Mental Health Consequences of Crisis and Disaster Primary Victims/ Survivors Rescue and Recovery Personnel “RESISTANCE, RESILIENCE, AND RECOVERY” AS A STRATEGIC AND INTEGRATIVE INTERVENTION PARADIGM Historical Foundations Resistance, Resiliency, Recovery: A Continuum of Care Building Resistance Self‐efficacy Hardiness Enhancing Resilience Fostering Recovery LEADERSHIP AND THE INCIDENT MANAGEMENT AND INCIDENT COMMAND SYSTEMS (ICS) Leadership: What is it? Leadership Resides in Those Who Follow Incident Management Essential Information NIMS Components 1 Psychological Issues in Escape, Rescue, and Survival in the Wake of Disaster | George Everly, Jr. The Need for Incident Management Key Features of the ICS Placement of Psychological Crisis Intervention Teams in ICS Functional Areas in the Incident Command System Structuring the Mental Health Response Challenges of Rural and Isolated Response Caution: Fatigue in Incident Response Summary CONCLUSIONS AND RECOMMENDATIONS REFERENCES APPENDIX A – Training resources in disaster mental health and crisis intervention APPENDIX B – Psychological First Aid (PFA) 2 Psychological Issues in Escape, Rescue, and Survival in the Wake of Disaster | George Everly, Jr. Introduction The experience of disaster appears to have become an expected aspect of life. Whether it is a natural disaster such as a hurricane or tsunami, or a human‐made disaster such as terrorism, the effects can be both physically and psychological devastating. -
53 Rolling, Trying to Grab on with My Spike Claws
AN APPLE PAPERBACK SCHOLASTIC INC. New York Toronto London Auckland Sydney Mexico City New Delhi Hong Kong For Scott Bremner And for Michael and Jake <They're going after the elementary school,> Tobias said. <They're going after everything,> I answered. <Why are they doing this? It makes no sense,> Tobias said. <It's not just brutal; it's stu- pid. Pointless destruction.> The nearest Bug fighter swooped low and slow. It fired its Dracon beams and the two-story gym exploded into charred stucco and twisted steel beams. It drifted almost casually above the tired old low-slung classrooms and fired again, dragging the beam end-to-end along the buildings. <They're sending a message,> I said. <Mess with us and this is what we do.> 1 We had destroyed the Yeerk pool. The Yeerk More Bug fighters than I'd ever seen in one pool was now the world's biggest sinkhole. It place. Maybe fifty of the things. They blasted looked like a crater. It was a crater, with half the schools; they blasted businesses; they blasted mall in ruins on one slope, jumbled bits of homes and churches. The shock waves would fast-food restaurants, streetlights, ripped up reach us, echoes of destruction. Pillars of smoke concrete, cars, skinny trees, all tumbled rose high in the air. Fires, some blazing and roar- together at the bottom. The water of the Yeerk ing, others smoldering sullenly, created thermal pool, looking like molten lead, soaked up updrafts that were bread and butter to three through the dirt. -
Looting After a Disaster: a Myth Or Reality?
Volume XXXI • Number 4 March 2007 Disaster Myths...Fourth in a Series Looting After a Disaster: A Myth or Reality? his special article in the Disaster Myths series pres- among those concerned with public safety and response Tents a point-counterpoint on the signifi cance and in disasters. prevalence of looting a� er disasters. Both authors were The fi rst author, E.L. Quarantelli, provides a his- asked to answer, independently, a series of questions, torical overview of looting in disaster research to help including whether looting a� er disasters is a myth, elucidate the myth. The fi ndings of previous disaster what evidence supports that opinion, what previous research are used to support the argument that looting, research has established about looting, and how the in fact, is not prevalent a� er disasters. In the end, there myths (and realities) about looting infl uence disaster is a lack of evidence showing that this behavior is com- planning and response. While the previous articles in monplace. This article can be found on page 2. this series were meant to help dispel disaster myths, As a counterpoint, Kelly Frailing focuses on the this article demonstrates the debate surrounding the events following Hurricane Katrina as evidence that controversial issue of looting and explores it in greater looting is not a myth, but a reality of disasters. This po- depth. Together these positions reveal the arguments sition is also supported by experience during previous and evidence for both sides of the debate. The editors events, such as Hurricane Betsy, and by crime statistics. -

Natural Disaster Emergency Planning and Preparedness Risk Bulletin
Natural disaster emergency planning and preparedness An Environmental Risk Toolkit AXA XL Environmental Risk Bulletin Be prepared. Natural Disaster Emergency Planning and Preparedness . 1 Disasters can happen at any time. Imagine that your business or facility is hit by a natural disaster, such as a hurricane, tornado, flood, earthquake or large wildfire. How will you ensure that your business quickly returns to normal operations and profitability? How will you protect your employees? One way to help do this is to create a Natural Disaster Preparedness and Response Plan. Both the final plan and the planning process are useful tools to respond to emergencies and to minimize costs and business interruptions. It can also be a strategic tool in business planning to ensure operational continuity. Being prepared and having a written plan should also help companies more effectively respond to any third party liabilities and claims that may arise from the surrounding community in the aftermath of a disaster. Why Plan for Natural Disasters? But why should we plan since natural disasters are rare? One of the primary reasons is potential cost savings to the affected business. Preparedness saves time and money by allowing a faster and more efficient resumption of routine business activities. Preparedness and periodic planning help businesses return to normal operation after a man-made or natural disaster. A disaster plan may also help enable a firm to stay in business and survive catastrophic events. According to the U.S. Federal Emergency Management Agency (FEMA), small businesses that don’t have a plan in place generally don’t survive after a disaster. -

Reading for Life and Adolescent Re-Arrest: Evaluating a Unique Juvenile Diversion Program
Reading For Life and Adolescent Re-Arrest: Evaluating a Unique Juvenile Diversion Program A. D. Seroczynski (Center for Children and Families, University of Notre Dame) William N. Evans (Wilson Sheehan Lab for Economic Opportunities, University of Notre Dame and NBER) Amy D. Jobst (Reading for Life, Inc.) Luke Horvath (Wilson Sheehan Lab for Economic Opportunities, University of Notre Dame) Giuliana Carozza (Wilson Sheehan Lab for Economic Opportunities, University of Notre Dame) July 15, 2015 Abstract We present results of an evaluation of Reading for Life (RFL), a diversion program for non-violent juvenile offenders in a medium-sized Midwestern county. The unique program uses philosophical virtue theory, works of literature, and small mentoring groups to foster moral development in juvenile offenders. Participants were randomly assigned to RFL treatment or a comparison program of community service. The RFL program generated large and statistically significant drops in future arrests. The program was particularly successful at reducing the recidivism of more serious offenses for those groups with the highest propensity for future offenses. Acknowledgements: This research was supported by grants from the Templeton Foundation and the University of Chicago’s Arête Initiative, the Florence V. Carroll Charitable Trust, the Stanley A. and Flora P. Clark Memorial Community Trust Foundation, the Muessel-Ellison Memorial Trust Foundation, the John, Anna and Martha Jane Fields Trust Foundation, the Wilson Sheehan Lab for Economic Opportunities, and the Fellow Irish Social Hub. The authors would like to thank the staff of the St. Joseph County Juvenile Justice Center’s Probation Department for their support of this project. Specifically, we would like to acknowledge the assistance of Bill Bruinsma, Ph.D., former Director, Thomas N. -

Glossary of Terms
page GLO-1 Glossary of Terms Words, phrases, abbreviations, and acronyms relevant to emergency management should be defined. Many terms in emergency management have special meanings, so it is important to establish precise definitions. Such definitions allow the users of the EOP to share an understanding of the EOP. American Red The American Red Cross is a humanitarian organization, led by volunteers, that Cross provides relief to victims of disasters and helps people prevent, prepare for, and respond to emergencies. It does this through services that are consistent with its Congressional Charter and the Principles of the International Red Cross Movement. Attack A hostile action taken against the United States by foreign forces or terrorists, resulting in the destruction of or damage to military targets, injury or death to the civilian population, or damage or destruction to public and private property. Checklist Written (or computerized) enumeration of actions to be taken by an individual or organization, meant to aid memory rather than provide detailed instruction. Chief The official of the community who is charged with authority to implement and Executive administer laws, ordinances, and regulations for the community. He or she Official may be a mayor, city manager, etc. Community A political entity which has the authority to adopt and enforce laws and ordinances for the area under its jurisdiction. In most cases, the community is an incorporated town, city, township, village, or unincorporated area of a county. However, each State defines its own political subdivisions and forms of government. Contamination The undesirable deposition of a chemical, biological, or radiological material on the surface of structures, areas, objects, or people. -
Responding to Victims of Terrorism and Mass Violence Crimes Coordination and Collaboration Between American Red Cross Workers and Crime Victim Service Providers
U.S. Department of Justice Office of Justice Programs Responding to Victims of Terrorism and Mass Violence Crimes Coordination and Collaboration Between American Red Cross Workers and Crime Victim Service Providers “Putting Victims First” U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Alberto R. Gonzales Attorney General Regina B. Schofield Assistant Attorney General John W. Gillis Director, Office for Victims of Crime Office of Justice Programs Partnerships for Safer Communities www.ojp.usdoj.gov Office for Victims of Crime www.ovc.gov NCJ 209681 This document was prepared by the Office for Victims of Crime and the American Red Cross under contract number OJP–2001–253–M, awarded by the Office for Victims of Crime, Office of Justice Programs, U.S. Department of Justice. The opinions, findings, and conclusions expressed in this document are those of the author and do not necessarily represent the official position or policies of the U.S. Department of Justice. The Office for Victims of Crime is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance, the Bureau of Justice Statistics, the National Institute of Justice, and the Office of Juvenile Justice and Delinquency Prevention. Contents Introduction and Overview . .1 OVC/American Red Cross Collaborative Timeline . .2 Natural Disasters, Acts of Terrorism, and Mass Violence Crimes: Similarities and Differences . .3 Office for Victims of Crime . .6 Crime Victim Assistance and Services . .8 Grants and Funding Available to Organizations Through OVC . .10 Basics of the Criminal Justice Process . .11 Conclusion . .13 References and Resources . -

Disaster Recovery: COVID-19 Pandemic Intensifies Disaster Recovery Challenges for K- 12 Schools
441 G St. N.W. Washington, DC 20548 October 14, 2020 Congressional Committees Disaster Recovery: COVID-19 Pandemic Intensifies Disaster Recovery Challenges for K- 12 Schools More than 260 presidentially-declared major disasters have occurred since 2017, affecting every state and several U.S. territories, according to the Federal Emergency Management Agency (FEMA).1 Many of these natural disasters have had devastating effects, including rendering K-12 school facilities unusable for extended periods of time. These schools are now experiencing the compounding challenge of recovering from these natural disasters while managing effects of the Coronavirus Disease 2019 (COVID-19). Social distancing practices and building closures are meant to keep staff and students safe, but may also complicate recovery efforts for disaster-affected districts. The Additional Supplemental Appropriations for Disaster Relief Act of 2019 provided funds for GAO to audit issues related to presidentially-declared major disasters that occurred in 2018.2 We reviewed (1) how the COVID-19 pandemic has affected schools recovering from recent natural disasters, and (2) support the U.S. Department of Education (Education) has provided to help schools recover from recent natural disasters and how the COVID-19 pandemic has affected schools’ use of these resources. In April 2020 we adjusted the scope of our work on school communities’ recovery efforts from recent natural disasters to refocus on how such efforts were affected by the COVID-19 pandemic. We interviewed 29 local education officials representing over 50 school districts in California, Commonwealth of the Northern Mariana Islands, Florida, and Hawaii, which were selected because they were affected by a diverse set of major natural disasters in 2018 that occurred in a mix of populated and less-populated areas.3 In addition, through a national school superintendents association, we convened a discussion group of seven district leaders who have experienced natural disasters and mentor other affected districts. -
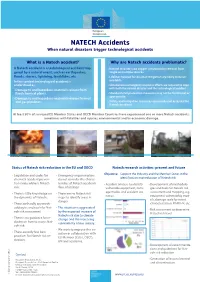
Natech Leaflet
NATECH Accidents When natural disasters trigger technological accidents What is a Natech accident? Why are Natech accidents problematic? A Natech accident is a technological accident trig- • Natural disasters can trigger simultaneous releases from gered by a natural event, such as earthquakes, single or multiple sources. floods, storms, lightning, landslides, etc. • Lifelines needed for disaster mitigation are likely to be un- In this context technological accident is available. understood as: • Simultaneous emergency response efforts are required to cope • Damage to and hazardous-materials release from with both the natural disaster and the technological accident. fixed chemical plants. • Standard civil protection measures may not be functional or appropriate. • Damage to and hazardous-materials release from oil and gas pipelines. • Safety and mitigation measures are usually not assessed for Natech accidents. At least 50% of surveyed EU Member States and OECD Member Countries have experienced one or more Natech accidents, sometimes with fatalities and injuries, environmental and/or economic damage. Earthquake, Turkey, 1999 Floods, Czech Republic, 2002 Status of Natech risk reduction in the EU and OECD Natech research activities: present and future • Legislation and codes for • Emergency response plans Objective: Support the industry and the Member States in the chemical accident preven- do not consider the charac- identification and reduction of Natech risk. tion rarely address Natech teristics of Natech accidents • Accident analysis to identify • Development of methodolo- risk. (loss of utilities). vulnerable equipment, dam- gies and tools for Natech risk • There is little knowledge on • There are no Natech risk age modes and accident sce- assessment and mapping, e.g. narios. -
Natural Disasters and Emergency Preparedness
Risk Management Guidebook Natural Disasters and Emergency Preparedness USI Insurance Services Property & Casualty usi.com DISCLAIMER: The information contained in this document is for informational purposes only and is not intended as, nor does it constitute, legal or professional advice to the reader. In no event will USI or any of its affiliates be liable in tort or in contract to anyone who has access to or uses this information. USI does not warrant that the information in this document constitutes a complete and finite list of each and every item or procedure related to the topics and issues referenced herein. Federal, state, and local laws, regulations, standards and codes may change over time, and the reader should always refer to the most current requirements, as applicable. © 2021 USI Insurance Services. All rights reserved. TABLE OF CONTENTS Is Your Organizaton Prepared? 3 This Natural Disasters and Emergency Preparedness Develop an Emergency Response Team and guide was developed Emergency Action Plan 5 to assist employers and residents in addressing the challenges of a catastrophic Severe Storm/Wildfire/Flood Preparedness 6 event, such as a flood, earthquake, tornado, Natural Disaster and Disaster Recovery/Restoration hurricane or wildfire, Checklist (Pre- and Post-Event) 8 against the backdrop of the COVID-19 pandemic. Catastrophic Event Preparedness Checklist for Facilities 10 Resources and Links 11 Is Your Organization Prepared? Don’t wait until a natural disaster is imminent: Proactively prepare before the next hurricane, flood, earthquake, wildfire or severe weather event to help keep yourself, your business and your employees safe. The potential for future surges of COVID-19 cases could create additional challenges in the wake of a catastrophic event.