Modeling Potential Responses to Smallpox As a Bioterrorist Weapon
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
History and Epidemiology of Global Smallpox Eradication Smallpox
History and Epidemiology of Global Smallpox Eradication Smallpox Three Egyptian Mummies 1570-1085 BC Ramses the Vth Died 1157 BC Early Written Description of Smallpox India 400 AD “Severe pain is felt in the large and small joints, with cough, shaking, listlessness and langour; the palate, lips, and tongue are dry with thirst and no appetite. The pustules are red, yellow, and white and they are accompanied by burning pain. The form soon ripens …the body has a blue color and seems studded with rice. The pustules become black and flat, are depressed in the centre, with much pain.” Smallpox and History • In the Elephant war in Mecca 568 AD, smallpox decimated the Ethiopian soldiers • Introduction of smallpox into the new world (Carribean 1507, Mexico 1520, Peru 1524, and Brazil 1555 ) facilitated Spanish conquest • Smallpox destroys Hottentots (1713) • In 1738, smallpox killed half the Cherokee Indian population • Smallpox disrupted colonial army in 1776 Smallpox Control Strategies • Smallpox hospitals (Japan 982 AD). • Variolation 10th Century. • Quarantine 1650s. • Home isolation of smallpox in Virginia 1667. • Inoculation and isolation (Haygarth 1793). • Jenner and widespread practice of vaccination throughout Europe and rest of the world. • Mass vaccination. • Surveillance containment. Variolation Inoculation with Smallpox Pus • Observations: – Pocked marked persons never affected with smallpox – Persons inoculated with smallpox pustular fluid or dried scabs usually had milder disease • Not ideal control strategy – Case fatality rate still 2% – Can transmit disease to others during illness The 1st Smallpox Vaccination Jenner 1796 Cowpox lesions on the hand of Sarah Nelmes (case XVI in Jenner’s Inquiry), from which material was taken for the vaccination of James Phipps below in 1796 History of Smallpox Vaccination 1805 Growth of virus on the flank of a calf in Italy. -

Global Effort Pays Off.. Smallpox at Target "Zero"
DXIEIJMECIX: CENTER FOR DISEASE CONTROL ATLANTA, GEORGIA 30333 VOLUME 11, NO. 10 Zero Smallpox Issue This issue of DATELINE: CDC is devoted to the story of the eradi cation of smallpox and CDC's in volvement. Inside stories include: • Historical vignettes • Pictures of field work • The last case of U.S. smallpox • An early campaign to eliminate the disease • Technology of eradication • Future of the smallpox virus • Chronology of smallpox, and others ft#***#*####*#****#*#*********** Throughout this issue are scattered stories o f "unsung heroes" from many nations who worked with CDC staff in V A R IO LA MAJOR'S last case Rahima Banu, AFTER RECOVERY, Ali Maow Maalin, the fight against smallpox. We have a little girl in Bangladesh who survived. will have chance for normal life. asked the staffers who worked with them to write about them, and all Global Effort Pays Off.. represent true stories o f the eradica tion battle. Smallpox at Target "Zero" -ft****************************** The last documented, naturally occurring case of smallpox was diagnosed in Physicians Challenged Merka, Somalia, in 1977. On October 26, 1979, the world celebrated its second anniversary free from smallpox transmission. Smallpox in 1844 A li Maow Maalin, then 23, was a of confidence among a trained army of The WHO campaign against small cook in Somalia when he came down smallpox fighters from most of the pox wasn't the first time war had been with smallpox. When he recovered, nations of the world — confidence that declared on the disease. he became the last recorded case of they could be successful in combat In 1844 the progress of a vaccina variola minor, a less severe form of with an old enemy. -

ROTA NEWS July 25 Th , 2013
ROTA NEWS July 25 th , 2013 Rotary Club of Barbados, Barbados Chartered March 07, 1962 District 7030 Club Officers President Ronald Davis President Elect Ron Davis Vice President Elvin Sealy Secretary Paul Ashby Treasurer Brian Cole Club Service Director R.I Theme 2013-2014 H. Waldo Clarke Vocational Service Director Officers District Officers Jedder Robinson District Governor President Community Service Director Herve Honoré Shawn Franklin Ron Burton District Governor Elect International Service Director President Elect Elwin Atmodimedjo Lisa Cummins Gary C.K. Huang Youth Service Director District Governor Nominee Warren Mottley Milton Inniss Immediate Past President Assistant Governor (Barbados) Anthony Williams Katrina Sam-Prescod Sergeant-At-Arms Alexander McDonald District Grants PDG David Edwards, Chair District Disaster Relief PDG Tony Watkins, Chair The Four Way Test Weekly meetings on Thursdays at Hilton Barbados Of the things we think, say or do Needham’s Point, Aquatic Gap, 1. Is it the TRUTH? St. Michael at 12 noon 2. Is it FAIR to all concerned? 3. Will it build GOODWILL and BETTER P.O. Box 148B, Brittons Hill, FRIENDSHIPS ? St. Michael, Barbados 4. Will it be BENEFICIAL to all concerned? www.clubrunner.ca/barbados Biography Burton has received the RI Service Above Self Award and the Foundation’s Citation for Meritorious Ron D. Burton Service, Distinguished Service Award, and International Service Award for a Polio-Free World. Rotary Club of Norman, Oklahoma, USA, He and his wife, Jetta, are Paul Harris Fellows, President, Rotary International, 2013-14 Benefactors, Major Donors, and members of the Paul Harris, Bequest, and Arch C. Klumph Societies. -

The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More Information
Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information The Life and Death of Smallpox This is an engaging and fascinating story of a conditional human success story. Smallpox has been one of the most devastating scourges of humanity throughout recorded history, and it is the only human illness to have been eradicated, though polio may soon follow it to official extinction through human agency. However, while smallpox is officially extinct in nature, our fears that stocks of smallpox virus may return as a weapon of bioterrorists have led to the stockpiling of vaccine, and continuing vigilance, even though the official victory over smallpox is now 15 years old. The Life and Death of Smallpox presents the entire engaging history of our struggle and ultimate (?) victory over one of our oldest and worst enemies. The story of the campaign to track down and eradicate the virus, throughout the world – the difficulties, setbacks, and the challenges successfully met – is a highlight of a fascinating book, but we cannot be confident of the ending. The final chapter of the book clearly and authoritatively explains the current status of the threat from the deliberate release of smallpox or other potential agents of biological terrorism. Ian Glynn is Professor Emeritus of Physiology at Cambridge University and Fellow of Trinity College. He is the author of An Anatomy of Thought (1999). Jenifer Glynn is a Cambridge historian and author of Tidings From Zion (2000). © Cambridge University Press www.cambridge.org Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information The Life and Death of Smallpox IAN AND JENIFER GLYNN © Cambridge University Press www.cambridge.org Cambridge University Press 0521845424 - The Life and Death of Smallpox Ian and Jenifer Glynn Frontmatter More information PUBLISHED BY CAMBRIDGE UNIVERSITY PRESS 40 We s t 20th Street, New York, NY 10011-4211, USA http://www.cambridge.org c Ian and Jenifer Glynn 2004 This book is in copyright. -
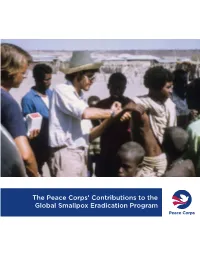
The Peace Corps' Contributions to the Global Smallpox Eradication Program
The Peace Corps’ Contributions to the Global Smallpox Eradication Program About the Office of Strategic Information, Research, and Planning (OSIRP) It is the mission of OSIRP to advance evidence-based management at the Peace Corps by guiding agency strategic planning; monitoring and evaluating agency-level performance and programs; conducting research to generate new insights in the fields of international development, cultural exchange, and Volunteer service; enhancing the stewardship and governance of agency data; and helping to shape agency engagement on high-level, governmentwide initiatives. Front Cover: Peace Corps Volunteers Robert Steinglass and Doug Arbuckle administering the smallpox vaccine in Mille, Ethiopia, in 1974. Photo: Steinglass, personal collection. ii Dedication This report is dedicated to the memory of Dr. Donald Ainslie “D. A.” Henderson (September 7, 1928—August 19, 2016), a seminal figure in the field of smallpox eradication. The Peace Corps is deeply appreciative of having had the opportunity to correspond with Dr. Henderson about the contributions of Peace Corps Volunteers and returned Volunteers within the context of the global eradication program. His charismatic leadership, tireless energy, and unflagging devotion to this program inspired countless public health workers around the world, including many of the returned Peace Corps Volunteers interviewed for this report. iii Acknowledgments In 1806, approximately 10 years after Dr. Edward Jenner conducted the first documented experiment with smallpox vaccination, laying the foundations of modern medicine, President Thomas Jefferson wrote to the English physician and scientist. Jefferson acknowledged the importance of this discovery, extending “a portion of the tribute of gratitude due to you from the whole human family. -

Citizen Medicine Hewish (A
COMMENT BOOKS & ARTS and the lab’s Radio Astronomy Group, MEDICAL RESEARCH led by Martin Ryle, had a series of suc- cesses, most famously the discovery of pulsars by Jocelyn Bell Burnell in 1967, working with her supervisor Antony Citizen medicine Hewish (A. Hewish et al. Nature 217, 709–713; 1968). By this time, the Sally Frampton and Sally Shuttleworth explore a show Cavendish was so large that its director on public involvement in the evolution of vaccination. was not so much a powerful commander- in-chief as chair of a company, as Longair aptly describes it. he introduction of vaccination in Vaccination: centuries, pamphlets The lab’s research had outgrown its the late eighteenth century is often Medicine and the from Britain’s National space: the number working there had viewed as a defining moment, when Masses Anti-Vaccination risen from around a dozen in the 1870s Tmodern medicine began to stem the ravages Hunterian Museum, League and others London. to some 40 times that number. In 1973, of disease. But it has not just been down to Until 17 September played on fears that the the next director, Brian Pippard, moved pioneering doctors: members of the public 2016. procedure poisoned the Cavendish to much larger premises in have been significant in shaping the devel- children’s blood and West Cambridge, the workplace of about opment of vaccination, both as practitioners laid them open to a host of diseases. Resist- 1,000 people. Longair chronicles this move and as critics. Vaccination: Medicine and the ance grew to the British government’s com- and presents the achievements of Pippard Masses, an exhibition at the Royal College of pulsory smallpox-vaccination programme, and his successors as Cavendish Profes- Surgeons’ Hunterian Museum in London, established in 1853. -

Smallpox by FELICIA M
ddiseasesanddisorders sSmallpox BY FELICIA M. WILLIS There has not been a naturally occurring case of smallpox since the 1970s, and in 1980, the World Health Organization declared that smallpox had been eliminated entirely through vaccina- tions. But smallpox has come into the forefront of news headlines because of its potential to be used as an agent in biological war- fare. With its extremely high fatality rate, small- pox represents a serious danger to the civilian population. Feared as one of the most devastating of all the infectious dis- eases, smallpox—also called variola— Micrograph of the smallpox virus, poxvirus variola. is caused by the poxvirus variola and is highly contagious, disfiguring, and it has a stockpile of 15.4 million doses of vaccine. Also, often lethal. antiviral drugs that have been developed since smallpox There are three forms of variola— was eradicated, such as hexadecyloxypropyl-cidofivir major, minor, and varioloid. Variola (HDP-CDV), are now being tested to see whether they are major (classic smallpox) is the most effective against the smallpox virus. These drugs carry molec- severe form of the disease and kills 30% ular disguises that allow them to be absorbed in the intestine Ali Maow Maalin, a Somal- of people who are unvaccinated, become ian, had the last known so that they can be given orally. A team at the U.S. Army infected, and do not receive treatment; case of endemic smallpox Medical Research Institute of Infectious Diseases conducted stud- 3% of those who are vaccinated die. in 1977. ies with HDP-CDV and found that just five oral doses given to Variola minor is considered a milder cowpox-virus-infected mice prevented their death, while form of the disease and kills 1–2% of people who are unvaccinated untreated mice died in nine days. -
PP Pandemics-And-IGJ
Foundation for the Rights of Future Generations Has the world responded to the coronavirus pandemic in an intergenerationally just manner? Three aspects are relevant to intergenerational justice: the number of dead and ill (medical dimension), the economic downturn (economic dimension), and the additional national debt (dimension of financial sustainability). The goal must be to protect future societies from the cumulative damage that pandemic may cause. Against this background, a new vaccination strategy for humanity – and this includes the individual national states – turns out to be the most important element. Such a strategy would help to ease the diseases we can ease and eradicate the diseases we can eradicate. And this not only in the rich countries, but worldwide. This is not only necessary for social and/or developmental reasons, but also serves the self-protection of the richer countries in an interconnected world. We need more government funding for prophylactic vaccine research. This would lead to the typical development time of a vaccine – 10-12 years on average – being shortened. The rapid development of vaccines against SARS-CoV-2 shows that a reduction to 1-2 years is possible if the necessary resources are made available. The testing of vaccine candidates for each infectious disease, however, comes with the cost of at least in the high three-digit million euro range. Profit-oriented companies cannot reasonably be expected to produce vaccines that may never be needed at their own expense in advance. In the future, vaccines must therefore be treated as "global public goods", whose development and production are primarily the responsibility of states. -

WH-1987-Aug-Sep-Eng.Pdf
Cover: For ten years the world has been spared such a sight~a baby suffering from smallpox. Photo WHO IX ISSN 0043-8502 World Health is the officia l il lu strated magazine of the World Hea lth Organization Editor: John Bland Deputy Editor: Christiane Viedma Art Editor: Peter Davies News Page Editor: Peter Ozorio World Health appears ten trmes a year in English, French, Portuguese, Russian and Spanish, and four times a year in Arabic and Farsi. The German edition is obtainable from · German Green Cross, Schuhmarkt 4, 3550 Marburg, FRG. Articles and photographs not copyrighted may be reproduced provided credit is given to the World Health Organization. Signed articles do not necess arily reflect WHO's views. World Health, WHO, Av. Appia, 1211 Geneva 27, Switzerland. Contents Ten years of freedom from an ancient scourge Smallpox: never again ! by Halfdan Mahler . 3 In the aftermath of "target zero" byZdenekJezek . 4 The lessons learnt by Donald A. Henderson . 8 Progress in the right direction by lsao Arita. 12 The poorest had most to gain by Jarl Tranaeus. 14 A world freed the threat of smallpox. 16-17 Can smallpox return? by Frank Fenner. 18 Surveillance and research by Svetlana Marennikova . 22 Getting your money's worth by John F. Wickett . 24 Spin-off from space travel by Silvia Michanie and Frank L. Bryan . 26 • Department Health Manpower Development Meeting health needs by Abdul Rahman AI-Awadi 28 News Page ... 30-31 2 ·rEN YEARS OF FREEDOM FROM AN ANCIENT SCOURGE Smallpox: never agai1n! by Dr 'Halfdan Mahler Director-General of the World Health Organization en years have now elapsed since pull together in a venture that will the world's last case of endemic benefit not only our generation but that Usmallpox was detected, in of our children and our children's chil Somalia. -

Enhancing the Work of the HHS National Vaccine Program in Global Immunizations
Enhancing the work of the HHS National Vaccine Program in Global Immunizations Presentation of Draft Report and Draft Recommendations National Vaccine Advisory Committee Global Immunizations Working Group 11 September 2013 Phil LaRussa, MD Amy Pisani, MS Global Immunizations – the Ground Truth • Global immunizations are one of the most cost-effective, evidence-based public health measure there is to reduce morbidity and mortality from infectious diseases • Yet, a child still dies from a vaccine-preventable disease every 20 seconds • Better access to routine and new, and underutilized vaccines have the potential to save 23 million lives between 2011-2020 • The U.S. directly benefits from strong, effective global immunization systems • Reduce the risk of disease importations, • Strengthen global surveillance for infectious diseases • Contribute to overall global economic growth and stability • HHS contributions of technical assistance and scientific expertise should be leveraged to enhance global efforts such as the Decade of Vaccines Charge to NVAC – Feb 2012 • To review the role of HHS in global immunizations • To review the effects of global immunizations on global populations and the effects of global immunizations on US populations • To recommend how HHS can best continue to contribute to these efforts, consistent with its newly established Global Health Strategy and Goal 5 of the National Vaccine Plan • To recommend how to best communicate this information to decision makers and the general public to ensure continued sufficient resources -
Smallpox, Genetic Engineering, and Bio-Terrorism David A
Maryland Law Review Volume 62 | Issue 3 Article 4 That Wonderful Year: Smallpox, Genetic Engineering, and Bio-terrorism David A. Koplow Follow this and additional works at: http://digitalcommons.law.umaryland.edu/mlr Part of the National Security Commons Recommended Citation David A. Koplow, That Wonderful Year: Smallpox, Genetic Engineering, and Bio-terrorism, 62 Md. L. Rev. 417 (2003) Available at: http://digitalcommons.law.umaryland.edu/mlr/vol62/iss3/4 This Article is brought to you for free and open access by the Academic Journals at DigitalCommons@UM Carey Law. It has been accepted for inclusion in Maryland Law Review by an authorized administrator of DigitalCommons@UM Carey Law. For more information, please contact [email protected]. THAT WONDERFUL YEAR: SMALLPOX, GENETIC ENGINEERING, AND BIO-TERRORISM DAVID A. KoPLOW* In retrospect, 1973 was a most remarkable year. In January, the Miami Dolphins won Super Bowl VII, capping the only undefeated season in National Football League history;1 through the spring, Sec- retariat, perhaps the greatest thoroughbred ever, swept horse racing's Triple Crown;2 and in September, Billy Jean King whipped Bobby Riggs in tennis's much-hyped "Battle of the Sexes."' More seriously, 1973 was the year of the Supreme Court's famous Roe v. Wade4 deci- sion on abortion; Chile's President Salvador Allende Gossens was ousted and assassinated in a military coup d'etat,5 the disastrous Yom Kippur war erupted between Israel and its neighbors;6 and a cease fire agreement brought U.S. disengagement from -

'The Speckled Monster' (1960S-‐70S)
Making a Difference: Milestones in Public Health & Biotechnology: Canadian Connec@ons -- Lecture #7 – Smallpox: Eradica@ng ‘The Speckled Monster’ (1960s-70s) By Christopher J. Ru1y, Ph.D. Professional Medical Historian Health Heritage Research Services h2p://healthheritageresearch.com & Adjunct Lecturer, Dalla Lana School of Public Health, University of Toronto Living and Learning in ReGrement, Course E Class #2, October 27, 2017 Previous lecture slides available via: Glendon College, York U., Room A002 h2p://healthheritageresearch.com/clients/LLiR/ Introduc@on • Although smallpox was brought under control in Canada by the 1940s, it remained a major threat in many parts of the world into the 1960s and 1970s • Connaught Labs played a decisive role in a sophisGcated global smallpox eradicaon program that began in 1967 • Connaught scienGsts were criGcal in establishing a standard vaccine producGon method for the WHO and in assisGng local producers meet it • 40 years ago yesterday, on October 26, 1977, the last smallpox case in the world was reported – it was a man in Somalia – and smallpox was officially declared dead on December 9, 1979 C.J. Ru2y, This is Public Health: A Canadian History (Canadian Public Health Associaon eBook, 2010) - h2ps://www.cpha.ca/history-e-book Ru;y, C.J - “Making a Difference: Milestones in Public Health & Biotechnology – Canadian Connecons” – Lecture #7 – Smallpox: EradicaHng The Speckled Monster (1960s-70s) 2 Smallpox Eradica@on in North America • To set the scene in North America, Canada’s last naturally occurring (endemic) smallpox cases were reported in 1943, with several imported cases in 1945-46 • The last endemic cases in the U.S.