Eye Injuries
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Paramedic National EMS Education Standard
NORTHWEST COMMUNITY EMERGENCY MEDICAL SERVICES SYSTEM CCCooonnntttiiinnnuuuiiinnnggg EEEddduuucccaaatttiiiooonnn SSSeeepppttteeemmmbbbeeerrr 222000111222 EEyyee && EEaarr DDiissoorrddeerrss && TTrraauummaa Questions/comments are welcome. Please direct to Jen Dyer, RN, EMT-P EMS Educator NWC EMSS Con-Ed Eye and Ear Disorders and Trauma September 2012 – page 1 Paramedic National EMS Education Standard Integrates assessment findings with principles of pathophysiology to formulate a field impression and implement a treatment/disposition plan for patients with eye and ear disorders/trauma. Objectives: Upon completion of the class and review of the independent study materials and post-test question bank, each participant will do the following with a degree of accuracy that meets or exceeds the standards established for their scope of practice: 1. Identify the anatomical structures of the eye and describe the corresponding physiologic function of each. (C) 2. Explain the physiology of normal vision. (C) 3. Identify the anatomic structures of the ear and describe the corresponding physiologic function of each. (C) 4. Explain the physiology of normal hearing. (C) 5. Explain the physiology of equilibrium. (C) 6. Select and discuss maneuvers for assessing eye structures and functions (C) and demonstrate a thorough EMS assessment of ocular structures, visual acuity, pupils and ocular movements. (P) 7. Distinguish abnormal assessment findings/conditions of the eye: blurred vision, diplopia, photophobia, changes in vision, flashing, pupil exam, Adie’s pupil, oculomotor nerve paralysis, Horner’s Syndrome, blindness, deviation/paralytic strabismus, orbit fracture, cataracts, conjunctivitis, color blindness, near sightedness, farsightedness, astigmatism, amblyopia, burns of the eye, corneal abrasions, foreign body, inflammation of the eyelid, glaucoma, hyphema, iritis, orbital cellulitis, macular degeneration and trauma. -

Therapeutic and Inducing Effect of Corneal Crosslinking on Infectious
Differenteffectsofcornealcrosslinkingoninfectiouskeratitis 窑Review窑 Therapeuticandinducingeffectofcornealcrosslinking oninfectiouskeratitis 1DepartmentofOphthalmology,ShandongProvincial thecornealintrinsicbiomechanicalpropertyandthestiffness HospitalAffiliatedtoShandongUniversity,Jinan250000, ofcorneatoresistectasiaofcornea [1].Besidesitsoriginal ShandongProvince,China applicationforthekeratoconusandkeratectasia [2],CXLhas 2DepartmentofOphthalmology,thePeople'sHospitalof beenutilizedontothetreatmentofinfectiouskeratitis [3], Linyi,Linyi276000,ShandongProvince,China nowadays.Althoughthesecondaryinfectiouskeratitisafter 3DepartmentofPediatrics,thePeople'sHospitalofLinyi, CXLisrare,therearesomereportsonsecondarykeratitis Linyi276000,ShandongProvince,China infectedby bacteria,fungi,herpessimplexvirusand Co-firstauthors: Liang-ZhuJiangandShi-YanQiu Acanthamoeba.ThisrarecomplicationofCXLcancause Correspondence to: Guo-YingMu.Departmentof seriousocularmorbidityandhaveasubsequentdamaging Ophthalmology,ShandongProvincialHospitalAffiliatedto effectonthepatient'svision.ThesurgicaltechniqueofCXL ShandongUniversity,Jinan250000,ShandongProvince, involvestheremovalofepitheliumintraoperativelyandthe [email protected] applicationofcontactlenspostoperatively.Thesefactors Received:2015-06-30Accepted:2016-08-09 havebeenassociatedwiththeoccurrenceofinfectious keratitisafterCXL.Inpresentstudy,wesummarizedthe Abstract therapeuticeffectofCXLoninfectiouskeratitisandthe · Thecornealcrosslinking (CXL)withriboflavinand keratitissecondarytocorneaCXLreportedbyprevious -

Week of July 27, 2015 – Eye Injuries Protecting Your Eyes from Injury Is
Week of July 27, 2015 – Eye Injuries Protecting your eyes from injury is one of the most basic things you can do to keep your vision healthy throughout your life. And the most basic step a person can take to protect his/her eyes is wearing the proper protective eyewear. According to a national survey by the American Academy of Ophthalmology, only 35 percent of respondents said they always wear protective eyewear when performing home repairs or maintenance; even fewer do so while playing sports. Eye emergencies include: cuts, scratches, getting objects in the eye, burns, chemical exposures, and blunt injuries to the eye or eyelid. Certain eye infections and other medical conditions, such as blood clots or glaucoma, also represent serious conditions. Since the eye is easily damaged, any of these conditions can lead to vision loss. A black eye is a bruise and usually caused by direct trauma to the eye or face. The bruise is caused by bleeding under the skin. The tissue around the eye turns black and blue, gradually, over a few days, it changes to purple, green, and yellow. The abnormal color disappears within 2 weeks. Swelling of the eyelid and tissue around the eye may also occur. Certain types of skull fractures may also result in bruising around the eyes, even without direct injury to the eye. Sometimes, serious damage to the eye itself occurs from the pressure of a swollen eyelid or face and can result is a hyphema; which is blood in the front area of the eye. Trauma is a common cause of the condition and is often due to a direct hit to the eye from a ball. -

Chapter 32 FOREIGN BODIES of the HEAD, NECK, and SKULL BASE
Foreign Bodies of the Head, Neck, and Skull Base Chapter 32 FOREIGN BODIES OF THE HEAD, NECK, AND SKULL BASE RICHARD J. BARNETT, MD* INTRODUCTION PENETRATING NECK TRAUMA Anatomy Emergency Management Clinical Examination Investigations OPERATIVE VERSUS NONOPERATIVE MANAGEMENT Factors in the Deployed Setting Operative Management Postoperative Care PEDIATRIC INJURIES ORBITAL FOREIGN BODIES SUMMARY CASE PRESENTATIONS Case Study 32-1 Case Study 32-2 Case Study 32-3 Case Study 32-4 Case Study 32-5 Case Study 32-6 *Lieutenant Colonel, Medical Corps, US Air Force; Chief of Facial Plastic Surgery/Otolaryngology, Eglin Air Force Base Department of ENT, 307 Boatner Road, Suite 114, Eglin Air Force Base, Florida 32542-9998 423 Otolaryngology/Head and Neck Combat Casualty Care INTRODUCTION The mechanism and extent of war injuries are sig- other military conflicts. In a study done in Croatia with nificantly different from civilian trauma. Many of the 117 patients who sustained penetrating neck injuries, wounds encountered are unique and not experienced about a quarter of the wounds were from gunshots even at Role 1 trauma centers throughout the United while the rest were from shell or bomb shrapnel.1 The States. Deployed head and neck surgeons must be injury patterns resulting from these mechanisms can skilled at performing an array of evaluations and op- vary widely, and treating each injury requires thought- erations that in many cases they have not performed in ful planning to achieve a successful outcome. a prior setting. During a 6-month tour in Afghanistan, This chapter will address penetrating neck injuries all subspecialties of otolaryngology were encountered: in general, followed specifically by foreign body inju- head and neck (15%), facial plastic/reconstructive ries of the head, face, neck, and skull base. -

CAUSES, COMPLICATIONS &TREATMENT of A“RED EYE”
CAUSES, COMPLICATIONS & TREATMENT of a “RED EYE” 8 Most cases of “red eye” seen in general practice are likely to be conjunctivitis or a superficial corneal injury, however, red eye can also indicate a serious eye condition such as acute angle glaucoma, iritis, keratitis or scleritis. Features such as significant pain, photophobia, reduced visual acuity and a unilateral presentation are “red flags” that a sight-threatening condition may be present. In the absence of specialised eye examination equipment, such as a slit lamp, General Practitioners must rely on identifying these key features to know which patients require referral to an Ophthalmologist for further assessment. Is it conjunctivitis or is it something more Iritis is also known as anterior uveitis; posterior uveitis is serious? inflammation of the choroid (choroiditis). Complications include glaucoma, cataract and macular oedema. The most likely cause of a red eye in patients who present to 4. Scleritis is inflammation of the sclera. This is a very rare general practice is conjunctivitis. However, red eye can also be presentation, usually associated with autoimmune a feature of a more serious eye condition, in which a delay in disease, e.g. rheumatoid arthritis. treatment due to a missed diagnosis can result in permanent 5. Penetrating eye injury or embedded foreign body; red visual loss. In addition, the inappropriate use of antibacterial eye is not always a feature topical eye preparations contributes to antimicrobial 6. Acid or alkali burn to the eye resistance. The patient history will usually identify a penetrating eye injury Most general practice clinics will not have access to specialised or chemical burn to the eye, but further assessment may be equipment for eye examination, e.g. -

Diagnosis and Treatment of Neurotrophic Keratopathy
An Evidence-based Approach to the Diagnosis and Treatment of Neurotrophic Keratopathy ACTIVITY DIRECTOR A CME MONOGRAPH Esen K. Akpek, MD This monograph was published by Johns Hopkins School of Medicine in partnership Wilmer Eye Institute with Catalyst Medical Education, LLC. It is Johns Hopkins School of Medicine not affiliated with JAMA medical research Baltimore, Maryland publishing. Visit catalystmeded.com/NK for online testing to earn your CME credit. FACULTY Natalie Afshari, MD Mina Massaro-Giordano, MD Shiley Eye Institute University of Pennsylvania School of Medicine University of California, San Diego Philadelphia, Pennsylvania La Jolla, California Nakul Shekhawat, MD, MPH Sumayya Ahmad, MD Wilmer Eye Institute Mount Sinai School of Medicine Johns Hopkins School of Medicine New York, New York Baltimore, Maryland Pedram Hamrah, MD, FRCS, FARVO Christopher E. Starr, MD Tufts University School of Medicine Weill Cornell Medical College Boston, Massachusetts New York, New York ACTIVITY DIRECTOR FACULTY Esen K. Akpek, MD Natalie Afshari, MD Mina Massaro-Giordano, MD Professor of Ophthalmology Professor of Ophthalmology Professor of Clinical Ophthalmology Director, Ocular Surface Diseases Chief of Cornea and Refractive Surgery University of Pennsylvania School and Dry Eye Clinic Vice Chair of Education of Medicine Wilmer Eye Institute Fellowship Program Director of Cornea Philadelphia, Pennsylvania Johns Hopkins School of Medicine and Refractive Surgery Baltimore, Maryland Shiley Eye Institute Nakul Shekhawat, MD, MPH University of California, -

Herpetic Corneal Infections
FocalPoints Clinical Modules for Ophthalmologists VOLUME XXVI, NUMBER 8 SEPTEMBER 2008 (MODULE 2 OF 3) Herpetic Corneal Infections Sonal S. Tuli, MD Reviewers and Contributing Editors Consultants George A. Stern, MD, Editor for Cornea & External Disease James Chodosh, MD, MPH Kristin M. Hammersmith, MD, Basic and Clinical Science Course Faculty, Section 8 Kirk R. Wilhelmus, MD, PhD Christie Morse, MD, Practicing Ophthalmologists Advisory Committee for Education Focal Points Editorial Review Board George A. Stern, MD, Missoula, MT Claiming CME Credit Editor in Chief, Cornea & External Disease Thomas L. Beardsley, MD, Asheville, NC Academy members: To claim Focal Points CME cred- Cataract its, visit the Academy web site and access CME Central (http://www.aao.org/education/cme) to view and print William S. Clifford, MD, Garden City, KS Glaucoma Surgery; Liaison for Practicing Ophthalmologists Advisory your Academy transcript and report CME credit you Committee for Education have earned. You can claim up to two AMA PRA Cate- gory 1 Credits™ per module. This will give you a maxi- Bradley S. Foster, MD, Springfield, MA Retina & Vitreous mum of 24 credits for the 2008 subscription year. CME credit may be claimed for up to three (3) years from Anil D. Patel, MD, Oklahoma City, OK date of issue. Non-Academy members: For assistance Neuro-Ophthalmology please send an e-mail to [email protected] or a Eric P. Purdy, MD, Fort Wayne, IN fax to (415) 561-8575. Oculoplastic, Lacrimal, & Orbital Surgery Steven I. Rosenfeld, MD, FACS, Delray Beach, FL Refractive Surgery, Optics & Refraction C. Gail Summers, MD, Minneapolis, MN Focal Points (ISSN 0891-8260) is published quarterly by the American Academy of Ophthalmology at 655 Beach St., San Francisco, CA 94109-1336. -

Pediatric Pharmacology and Pathology
7/31/2017 In the next 2 hours……. Pediatric Pharmacology and Pathology . Ocular Medications and Children The content of th is COPE Accredited CE activity was prepared independently by Valerie M. Kattouf O.D. without input from members of the optometric community . Brief review of examination techniques/modifications for children The content and format of this course is presented without commercial bias and does not claim superiority of any commercial product or service . Common Presentations of Pediatric Pathology Valerie M. Kattouf O.D., F.A.A.O. Illinois College of Optometry Chief, Pediatric Binocular Vision Service Associate Professor Ocular Medications & Children Ocular Medications & Children . Pediatric systems differ in: . The rules: – drug excretion – birth 2 years old = 1/2 dose kidney is the main site of drug excretion – 2-3 years old = 2/3 dose diminished 2° renal immaturity – > 3 years old = adult dose – biotransformation liver is organ for drug metabolism Impaired 2° enzyme immaturity . If only 50 % is absorbed may be 10x maximum dosage Punctal Occlusion for 3-4 minutes ↓ systemic absorption by 40% Ocular Medications & Children Ocular Medications & Children . Systemic absorption occurs through….. Ocular Meds with strongest potential for pediatric SE : – Mucous membrane of Nasolacrimal Duct 80% of each gtt passing through NLD system is available for rapid systemic absorption by the nasal mucosa – 10 % Phenylephrine – Conjunctiva – Oropharynx – 2 % Epinephrine – Digestive system (if swallowed) Modified by variation in Gastric pH, delayed gastric emptying & intestinal mobility – 1 % Atropine – Skin (2° overflow from conjunctival sac) Greatest in infants – 2 % Cyclopentalate Blood volume of neonate 1/20 adult Therefore absorbed meds are more concentrated at this age – 1 % Prednisone 1 7/31/2017 Ocular Medications & Children Ocular Medications & Children . -

Bruises- Wounds
Henry Shih OD, MD Medical Director Austin Emergency Center- Anderson Mill 13435 US Highway 183 North Suite 311 Austin, TX 78750 512-614-1200 BRUISES- http://austiner.com/ What are bruises? — Bruises happen when blood vessels under the skin break, but the skin isn’t cut. Blood leaks into the tissues under the skin. Bruises start off red in color, and then turn blue or purple. As they heal, bruises can turn green and yellow. Most bruises heal in 1 to 2 weeks, but some take longer. How are bruises treated? — A bruise will get better on its own. But to feel better and help your bruise heal, you can: o Put a cold gel pack, bag of ice, or bag of frozen vegetables on the injured area every 1 to 2 hours, for 15 minutes each time. Put a thin towel between the ice (or other cold object) and your skin. Use the ice (or other cold object) for at least 6 hours after your injury. Some people find it helpful to ice longer, even up to 2 days after their injury. o Raise the area, if possible – Raising the area above the level of your heart helps to reduce swelling. o Take medicine to reduce the pain and swelling – To treat pain, you can take Tylenol. To treat pain and swelling, you can take ibuprofen (sample brand names: Advil, Motrin). But people who have certain conditions or take certain medicines should not take ibuprofen. If you are unsure, ask your doctor or nurse if you can take ibuprofen. -
Foreign Body Insertions: a Review
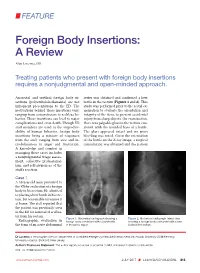
FEATURE Foreign Body Insertions: A Review Alan Lucerna, DO Treating patients who present with foreign body insertions requires a nonjudgmental and open-minded approach. Anorectal and urethral foreign body in- series was obtained and confirmed a beer sertions (polyembolokoilamania) are not bottle in the rectum (Figures 1 and 2). This infrequent presentations to the ED. The study was performed prior to the rectal ex- motivations behind these insertions vary, amination to evaluate the orientation and ranging from autoeroticism to reckless be- integrity of the item, to prevent accidental havior. These insertions can lead to major injury from sharp objects. On examination, complications and even death. Though ED there was palpable glass in the rectum con- staff members are used to the unpredict- sistent with the rounded base of a bottle. ability of human behavior, foreign body The glass appeared intact and no gross insertions bring a mixture of responses bleeding was noted. Given the orientation from the staff, ranging from awe and in- of the bottle on the X-ray image, a surgical credulousness to anger and frustration. consultation was obtained and the patient A knowledge and comfort in managing these cases includes a nonjudgmental triage assess- ment, collective professional- ism, and self-awareness of the staff’s reaction. Case 1 A 58-year-old man presented to the ED for evaluation of a foreign body in his rectum. He admitted to placing a beer bottle in his rec- tum, but was unable to remove it at home. The staff reported that the patient was previously seen in the ED for removal of a vibra- tor from his rectum. -

Foreign Rectal Body – Systematic Review and Meta-Analysis
REVIEW 61 Foreign rectal body – Systematic review and meta-analysis M. Ploner1, A. Gardetto2, F. Ploner3, M. Scharl4, S. Shoap5, H. C. Bäcker5 (1) Department of Anesthesiology and Intensiver Care, Cantonal Spital Lucerne, Lucerne, Switzerland ; (2) Department of Plastic Surgery, Hospital Sterzing, Sterzing, South Tirol, Italy ; (3) Department of Anesthesiology and Emergency Medicine, Hospital Sterzing, South Tirol, Italy ; (4) Department of Gastroenterology and Hepatology, University Hospital Zurich, University of Zurich, Swetzerland ; (5) Department of Orthopaedic Surgery, Columbia University Medical Center, New York, USA. Abstract instrumentation (7). The most common complication is a rectal injury, which can result from a variety of agents and Background : Self-inserted foreign rectal bodies are an objects (8). Often, nonsurgical removal of foreign bodies infrequent occurrence, however they present a serious dilemma to the surgeon, due to the variety of objects, and the difficulty of has been described to be successful – in 11% to 65% – extraction. The purpose of this study is to give a comprehensive (9), however, in many situations, a surgical treatment review of the literature regarding the epidemiology, diagnostic may be essential. There have been a variety of algorithms tools and therapeutic approaches of foreign rectal body insertion. Methods : A comprehensive systematic literature review on introduced for the management of extraction, however, Pubmed/ Medline and Google for ‘foreign bodies’ was performed because of the diversity of foreign bodies, improvisation, on January 14th 2018. A meta-analysis was carried out to evaluate as well creativity of the treating emergency physician the epidemiology, diagnostics and therapeutic techniques. 1,551 abstracts were identified, of which 54 articles were included. -
NEISS Coding Manual January 2018
NNEEIISSSS CCooddiinngg MMaannuuaall JJaannuuaarryy 22001188 NEISS – National Electronic Injury Surveillance System January 2018 Table of Contents Introduction ................................................................................................................................................. 1 General Instructions ................................................................................................................................... 1 General NEISS Reporting Rule .................................................................................................................. 1 Do Report .................................................................................................................................................. 1 Definitions .............................................................................................................................................. 2 Do Not Report ........................................................................................................................................... 3 Specific Coding Instructions ..................................................................................................................... 4 Medical Information Codes ........................................................................................................................ 4 Date of Treatment ..................................................................................................................................... 4 (8 spaces).................................................................................................................................................