Read Ebook {PDF EPUB} Pseudo by Dysonrules
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2014/134709 Al 12 September 2014 (12.09.2014) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/05 (2006.01) A61P 31/02 (2006.01) kind of national protection available): AE, AG, AL, AM, AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, (21) International Application Number: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, PCT/CA20 14/000 174 DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (22) International Filing Date: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, 4 March 2014 (04.03.2014) KZ, LA, LC, LK, LR, LS, LT, LU, LY, MA, MD, ME, MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, (25) Filing Language: English OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, (26) Publication Language: English SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (30) Priority Data: ZW. 13/790,91 1 8 March 2013 (08.03.2013) US (84) Designated States (unless otherwise indicated, for every (71) Applicant: LABORATOIRE M2 [CA/CA]; 4005-A, rue kind of regional protection available): ARIPO (BW, GH, de la Garlock, Sherbrooke, Quebec J1L 1W9 (CA). GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, (72) Inventors: LEMIRE, Gaetan; 6505, rue de la fougere, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, DK, Sherbrooke, Quebec JIN 3W3 (CA). -

Pseudomonas Skin Infection Clinical Features, Epidemiology, and Management
Am J Clin Dermatol 2011; 12 (3): 157-169 THERAPY IN PRACTICE 1175-0561/11/0003-0157/$49.95/0 ª 2011 Adis Data Information BV. All rights reserved. Pseudomonas Skin Infection Clinical Features, Epidemiology, and Management Douglas C. Wu,1 Wilson W. Chan,2 Andrei I. Metelitsa,1 Loretta Fiorillo1 and Andrew N. Lin1 1 Division of Dermatology, University of Alberta, Edmonton, Alberta, Canada 2 Department of Laboratory Medicine, Medical Microbiology, University of Alberta, Edmonton, Alberta, Canada Contents Abstract........................................................................................................... 158 1. Introduction . 158 1.1 Microbiology . 158 1.2 Pathogenesis . 158 1.3 Epidemiology: The Rise of Pseudomonas aeruginosa ............................................................. 158 2. Cutaneous Manifestations of P. aeruginosa Infection. 159 2.1 Primary P. aeruginosa Infections of the Skin . 159 2.1.1 Green Nail Syndrome. 159 2.1.2 Interdigital Infections . 159 2.1.3 Folliculitis . 159 2.1.4 Infections of the Ear . 160 2.2 P. aeruginosa Bacteremia . 160 2.2.1 Subcutaneous Nodules as a Sign of P. aeruginosa Bacteremia . 161 2.2.2 Ecthyma Gangrenosum . 161 2.2.3 Severe Skin and Soft Tissue Infection (SSTI): Gangrenous Cellulitis and Necrotizing Fasciitis. 161 2.2.4 Burn Wounds . 162 2.2.5 AIDS................................................................................................. 162 2.3 Other Cutaneous Manifestations . 162 3. Antimicrobial Therapy: General Principles . 163 3.1 The Development of Antibacterial Resistance . 163 3.2 Anti-Pseudomonal Agents . 163 3.3 Monotherapy versus Combination Therapy . 164 4. Antimicrobial Therapy: Specific Syndromes . 164 4.1 Primary P. aeruginosa Infections of the Skin . 164 4.1.1 Green Nail Syndrome. 164 4.1.2 Interdigital Infections . 165 4.1.3 Folliculitis . -

| Oa Tai Ei Rama Telut Literatur
|OA TAI EI US009750245B2RAMA TELUT LITERATUR (12 ) United States Patent ( 10 ) Patent No. : US 9 ,750 ,245 B2 Lemire et al. ( 45 ) Date of Patent : Sep . 5 , 2017 ( 54 ) TOPICAL USE OF AN ANTIMICROBIAL 2003 /0225003 A1 * 12 / 2003 Ninkov . .. .. 514 / 23 FORMULATION 2009 /0258098 A 10 /2009 Rolling et al. 2009 /0269394 Al 10 /2009 Baker, Jr . et al . 2010 / 0034907 A1 * 2 / 2010 Daigle et al. 424 / 736 (71 ) Applicant : Laboratoire M2, Sherbrooke (CA ) 2010 /0137451 A1 * 6 / 2010 DeMarco et al. .. .. .. 514 / 705 2010 /0272818 Al 10 /2010 Franklin et al . (72 ) Inventors : Gaetan Lemire , Sherbrooke (CA ) ; 2011 / 0206790 AL 8 / 2011 Weiss Ulysse Desranleau Dandurand , 2011 /0223114 AL 9 / 2011 Chakrabortty et al . Sherbrooke (CA ) ; Sylvain Quessy , 2013 /0034618 A1 * 2 / 2013 Swenholt . .. .. 424 /665 Ste - Anne -de - Sorel (CA ) ; Ann Letellier , Massueville (CA ) FOREIGN PATENT DOCUMENTS ( 73 ) Assignee : LABORATOIRE M2, Sherbrooke, AU 2009235913 10 /2009 CA 2567333 12 / 2005 Quebec (CA ) EP 1178736 * 2 / 2004 A23K 1 / 16 WO WO0069277 11 /2000 ( * ) Notice : Subject to any disclaimer, the term of this WO WO 2009132343 10 / 2009 patent is extended or adjusted under 35 WO WO 2010010320 1 / 2010 U . S . C . 154 ( b ) by 37 days . (21 ) Appl. No. : 13 /790 ,911 OTHER PUBLICATIONS Definition of “ Subject ,” Oxford Dictionary - American English , (22 ) Filed : Mar. 8 , 2013 Accessed Dec . 6 , 2013 , pp . 1 - 2 . * Inouye et al , “ Combined Effect of Heat , Essential Oils and Salt on (65 ) Prior Publication Data the Fungicidal Activity against Trichophyton mentagrophytes in US 2014 /0256826 A1 Sep . 11, 2014 Foot Bath ,” Jpn . -
Dermatology in the ER
DRUG ERUPTIONS and OTHER DISORDERS Lloyd J. Cleaver D.O. , F.A.O.C.D, F.A.A.D. Professor of Dermatology ATSU-Kirksville College of Osteopathic Medicine INTERNAL MEDICINE BOARD REVIEW COURSE I Disclosures No Relevant Financial Relationships DRUG ERUPTIONS Drug Reactions 3 things you need to know 1. Type of drug reaction 2. Statistics What drugs are most likely to cause that type of reaction? 3. Timing How long after the drug was started did the reaction begin? Clinical Pearls Drug eruptions are extremely common Tend to be generalized/symmetric Maculopapular/morbilliform are most common Best Intervention: Stop the Drug! Do not dose reduce Completely remove the exposure How to spot the culprit? Drug started within days to a week prior to rash Can be difficult and take time Tip: can generally exclude all drugs started after onset of rash Drug eruptions can continue for 1-2 weeks after stopping culprit drug LITT’s drug eruption database Drug Eruptions Skin is one of the most common targets for drug reactions Antibiotics and anticonvulsants are most common 1-5% of patients 2% of all drug eruptions are “serious” TEN, DRESS More common in adult females and boys < 3 y/o Not all drugs cause eruptions at same rate: Aminopenicillins: 1.2-8% of exposures TMP-SMX: 2.8-3.7% NSAIDs: 1 in 200 Lamotrigine: 10% Drug Eruptions Three basic rules 1. Stop any unnecessary medications 2. Ask about non-prescription medications Eye drops, suppositories, implants, injections, patches, vitamin and health supplements, friend’s medications -

Localized Whirlpool Folliculitis in a Football Player Justin J
Localized Whirlpool Folliculitis in a Football Player Justin J. Green, MD, Camden, New Jersey Pseudomonas aeruginosa folliculitis occurs in pa- lege football player, sustained a left ankle inversion tients exposed to contaminated water. Most out- sprain 2 days previously. Examination revealed mul- breaks are associated with whirlpools. The infec- tiple, 2- to 6-mm erythematous papules and pustules. tion is characterized by follicular, erythematous The pustules had a distinct light green hue with a cir- papules and pustules located on immersed body cumferential border of intense erythema (Figure 1). surfaces. Most reported cases are the result of Many of the papules and pustules were folliculo- recreational water use, occur in a diffuse pattern, centric. The eruption was clustered in two areas, and are devoid of green pustular pigment changes. separated by a few centimeters, on the medial aspect The case described occurred in a football player of the left leg. The area was tender, but without after whirlpool treatment for an ankle strain. Green edema, and the base of surrounding skin was non- pustules and a localized affected area are unusual erythematous. There was no associated lym- aspects of this case. phadenopathy. Further questioning revealed that the patient received a 20-minute hot whirlpool seudomonas aeruginosa is an aerobic, motile, treatment exclusively to the left leg (distal to the gram-negative rod that inhabits areas of mois- knee), approximately 24 hours prior to the eruption. P ture. The organism can live in sinks, jet fuel, Treatment with 250 mg ciprofloxacin orally twice antiseptic solutions, soil, sewage, flowers, vegetables, daily for 7 days was initiated, but follow-up revealed insects, and warm- and cold-blooded animals.1,2 It can that the patient took just one dose. -

Cambridge University Press 978-1-107-03891-2 - Clinical Infectious Disease Edited by David Schlossberg Index More Information
Cambridge University Press 978-1-107-03891-2 - Clinical Infectious Disease Edited by David Schlossberg Index More information Index Page references in bold indicate tables; those in italic indicate figures. abacavir (ABC), 650 otitis media, 49 PCP pneumonia, 1151–1152, abdominal infections. See intra- pregnant patients, 618 See also Pneumocystis jirovecii abdominal infections viral hemorrhagic fevers, 1246 pneumonia (PCP) Abiotrophia spp., 1042 Achromobacter spp., 1046 pregnant patients, 616 A. defectiva, 247 A. denitrificans, 1046 progressive multifocal abscess A. xylosoxidans, 1046 leukoencephalopathy abdominal, 367–369 clinical syndromes, 1046 association, 529–531 diagnosis, 367 epidemiology, 1046 treatment, 533–534 treatment, 367–369, 380 Acinetobacter baumannii, 1045–1046 splenic abscess, 372 brain. See brain abscess multidrug resistance, 1046 toxoplasmic encephalitis, 1279–1280 breast, 620 nosocomial infections, 1045 Acrobacter, 810 coccidioidomycosis, 1144 pneumonia, 222 acrodermatitis chronica atropicans, cranial epidural, 500–501, 501 Acinetobacter spp., 1044–1046, See also 1062 dental, 64,66 Acinetobacter baumannii Actinomyces spp. (actinomycosis), 829 HACEK organism-associated, 904, catheter-related infections, 721, 723 clinical presentation, 829–830 906 epidemiology, 1045 abdominal disease, 830–831 iliopsoas. See iliopsoas abscess (IPA) meningitis, 477 CNS disease, 831 intraperitoneal, 366, 375, 380 post-transplant infection, 576 disseminated disease, 831 lacrimal sac, 116 sepsis, 15 musculoskeletal disease, 831 liver. See liver -
September 2011\Protocol Book\Program-Speaker Page
Chicago Dermatological Society Monthly Educational Conference Program Information CME Certification and Case Presentations Wednesday, September 21, 2011 Conference Location & Host: Department of Dermatology Feinberg School of Medicine Northwestern University Chicago, Illinois Program Committees & Registration 8:00 a.m. - 9:00 a.m. CDS Plans & Policies Committee Program Activities 9:00 a.m. Clinic Registration Opens Dermatology Clinic; 676 N. St. Clair, Suite 1600 9:30 a.m. - 11:00 a.m. Clinical Rounds -- Patient, poster & slide viewing Dermatology Clinic 10:15 a.m. Conference Registration Opens Lurie Building; 303 E. Superior, 1st Floor Outside the Hughes Auditorium 10:15 - 11:15 a.m. Coffee with the Exhibitors Ryan Family Atrium, Lurie Building 11:15 a.m. - 12:15 p.m. Luncheon – Ryan Family Atrium 12:15 p.m. - 1:15 p.m. General Session - Hughes Auditorium BLUEFARB LECTURE – "Skin Signs of Systemic Disorders" Dirk M. Elston, MD 1:15 p.m. - 3:15 p.m. Case Discussions – Hughes Auditorium 3:15 p.m. Meeting adjourns Mark the Date! Next CDS monthly meeting – Wednesday, October 12, 2011 The University of Illinois at Chicago Samuel T. Hwang, MD, Medical College of Wisconsin Watch for details on the CDS website: www.ChicagoDerm.org Northwestern University Medical School Robert H. Lurie Medical Research Center Hughes Auditorium 303 E. Superior Street - First Floor Chicago, Illinois 60611 Registration: outside the Hughes Auditorium Lunch, General Session & Case Discussions Dermatology Clinic 676 N. Saint Clair Street, Suite 1600 Chicago, Illinois 60611 Patient/slide viewing & posters Parking Garage Locations At Saint Clair and Huron; enter from Huron (westbound) or Superior (eastbound). -

Vasodilator for Use to Treat Microbial Infections
(19) TZZ¥ ¥__T (11) EP 3 228 314 A1 (12) EUROPEAN PATENT APPLICATION (43) Date of publication: (51) Int Cl.: 11.10.2017 Bulletin 2017/41 A61K 31/4458 (2006.01) A61K 31/4422 (2006.01) A61K 31/145 (2006.01) A61P 31/04 (2006.01) (2006.01) (21) Application number: 17166322.2 A61P 33/00 (22) Date of filing: 09.09.2011 (84) Designated Contracting States: (72) Inventors: AL AT BE BG CH CY CZ DE DK EE ES FI FR GB • HU, Yanmin GR HR HU IE IS IT LI LT LU LV MC MK MT NL NO London, SW17 0RE (GB) PL PT RO RS SE SI SK SM TR • COATES, Anthony RM London, SW17 0RE (GB) (30) Priority: 10.09.2010 GB 201015079 (74) Representative: D Young & Co LLP (62) Document number(s) of the earlier application(s) in 120 Holborn accordance with Art. 76 EPC: London EC1N 2DY (GB) 11758257.7 / 2 613 774 Remarks: (71) Applicant: Helperby Therapeutics Limited This application was filed on 12-04-2107 as a London W1U 0RE (GB) divisional application to the application mentioned under INID code 62. (54) VASODILATOR FOR USE TO TREAT MICROBIAL INFECTIONS (57) The present invention relates to the use of one an antioxidant, a vasodilator and/or a vitamin, or a phar- or more compounds selected from the following classes maceutically acceptable derivative thereof, for use in the of biologically active agents: an α-adrenergic antagonist, treatment of a microbial infection and in particular for kill- an anthelmintic agent, an antifungal agent, an antimalar- ing multiplying, non-multiplying and/or clinically latent mi- ial agent,an antineoplastic agent, an antipsychoticagent, croorganisms associated with such an infection. -

A Literature Review of Pseudomonas Aeruginosa Infection and the Appropriate Regimen of Antibiotics Whether Combination Antibiotic Therapy Or Monotherapy
NORTHERN OHIO FOOT& ANKLE FOUNDATION ! The!Northern!Ohio!Foot!and!Ankle!Journal!!! ! ! ! !!!!!!!!!Official!Publication!of!the!NOFA!Foundation! ! A literature review of Pseudomonas aeruginosa infection and the appropriate regimen of antibiotics whether Combination antibiotic therapy or monotherapy. by Hazim Ibrahim DPM 1 The Northern Ohio Foot and Ankle Journal Abstract: Pseudomonas aeruginosa is a common cause of gram-negative infection, especially in patients with compromised host defense mechanisms. It is the most common pathogen isolated from patients who have been hospitalized longer than 1 week, and it is a frequent cause of nosocomial infections. Pseudomonas infections are complicated and can be life-threatening. The choice of antibiotic monotherapy or combination therapy to treat Pseudomonas aeruginosa bacteremia is controversial. The aim of this review is to discuss the infection by pseudomonas with its characteristics and to compare both types of therapy to determine which delivers the best outcome for P. aeruginosa bacteremia. Neither combination therapy nor monotherapy treatment appears to have a significant effect on mortality rates in patients with P. aeruginosa bacteremia. Further studies evaluating the effects of combination therapy or monotherapy in more specialized cases, such as when encountering a multidrug-resistant organism, are necessary. Key words: Pseudomonas aeruginosa, Drug resistance, monotherapy, gram negative infection Accepted: April, 2016 Published: May, 2016 This is an Open Access article distributed under the terms of the Creative Commons Attribution License. It permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. ©The Northern Ohio Foot and Ankle Foundation Journal. (www.nofafoundation.org) 2016. All rights reserved. -
General Bacteriology
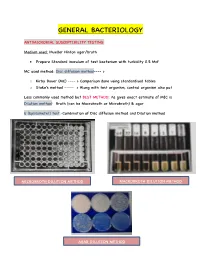
GENERAL BACTERIOLOGY ANTIMICROBIAL SUSCEPTIBILITY TESTING: Medium used: Mueller Hinton agar/broth Prepare Standard inoculum of test bacterium with turbidity 0.5 McF MC used method: Disc diffusion method---- > o Kirby Bauer (MC) ---- > Comparison done using standardised tables o Stoke's method ----- > Along with test organism, control organism also put Less commonly used method but BEST METHOD: As gives exact estimate of MIC is Dilution method: Broth (can be Macrobroth or Microbroth) & agar E (Epsilometer) test:-Combination of Disc diffusion method and Dilution method MICROBROTH DILUTION METHOD MACROBROTH DILUTION METHOD AGAR DILUTION METHOD KIRBY BAUER METHOD STOKE’S METHOD EPSILOMETER TEST BACTERIAL GROWTH CURVE: LAG PHASE: o Stage of adaptation o No replication takes place o Metabolically active LOG PHASE: o Stage of active replication o Increase in viable count o Metabolically most active STATIONARY PHASE: o Gradual depletion of nutrients o Bacteria multiplying = Bacteria dying o Exotoxins formed o Spores formed DECLINE PHASE: o Viable count decreasing o Total count constant BACTERIAL CELL: o Capsule/slime may or may not be formed o Cell wall contains peptidoglycan/ muramic acid o CM doesn’t contain sterols o 70S ribosomes o Mesosomes--- Invaginations of plasma membrane Respiratory chain enzymes present o Pili helps in adhesion o Flagella helps in motility o Unique amino acid in bacterial cell wall----- > Diaminopimelic acid o Polymers of NAG and NAM o Linked by peptides o Teichoic acid present of 2 types GRAM POSITIVE CELL WALL o -

Distribution of Pseudomonas Aeruginosa in Navigation Pool No
DISTRIBUTION OF PSEUDOMONAS AERUGINOSA IN NAVIGATION POOL NO. 8 OF THE UPPER MISSISSIPPI RIVER A Thesis Submitted to the Faculty of University of Wisconsin - La Crosse La Crosse, Wisconsin 54601 Shahaireen Madramootoo-Pell€tt In Partial Fulfillment of the Requirements for the Degree of Master of Science in Biology May 1977 [1\,1 71 r UNIVERSITY OF WISCONSIN - LA CROSSE La Crosse, Wisconsin 54601 COLLEGE OF ARTS, LETTERS, AND SCIENCES Candidate: Shahaireen Madramootoo-Pellett We recommend acceptance of this thesis to the College of Arts, Letters, and Sciences in partial fulfillment of this candidate 1 S requirements for the degree Master of Science in Biology. The candidate has completed her oral defense of the thesis. r- (). sis Committee Chairperson 7£Y21Thesis Committee2 ~ Member Date ~ a . ·~ommitt~ Date 31 ]/]] Date This thesis is approved for the College of Arts, Letters, and Sciences Date 77 11590 - ii ABSTRACT The distribution of Pseudomonas aeruginosa in Navigation Pool No. 8 of the Upper Mississippi River has been investigated. Serological and pyocin typing was performed on 152 isolates, and serological type 1 was found to be the most prevalent (34.2%). Pyocin typing was found to be the most efficient method of differentiation, although serological typing was more practical. A comparison of the total number of positive ~· aeruginosa samples fran each sample type showed that this pseudomonad was most commonly isolated fran sediment samples. Comparisons of each sample source indicated that recovery of f. aeruginosa was more frequent from the surface slime than from the feces of 52 fishes, and from plant parts below rather than above the water surface. -

Yellow Nail Syndrome: a Review Stéphane Vignes1* and Robert Baran2
Vignes and Baran Orphanet Journal of Rare Diseases (2017) 12:42 DOI 10.1186/s13023-017-0594-4 REVIEW Open Access Yellow nail syndrome: a review Stéphane Vignes1* and Robert Baran2 Abstract Yellow nail syndrome (YNS; OMIM 153300, ORPHA662) is a very rare disorder that almost always occurs after 50 years of age but a juvenile or familial form has also been observed. YNS is diagnosed based on a triad associating yellow nail discoloration, pulmonary manifestations (chronic cough, bronchiectasia, pleural effusion) and lower limb lymphedema. Chronic sinusitis is frequently associated with the triad. YNS etiology remains unknown but a role of lymphatic impairment is usually evoked. YNS is more frequently isolated but may be associated in rare cases with autoimmune diseases, other clinical manifestations implicating lymphatic functions or cancer and, hence, is also considered a paraneoplastic syndrome. YNS management is symptomatic and not codified. YNS can resolve spontaneously. Oral vitamin E alone or even better when associated with triazole antifungals may achieve partial or total disappearance of nail discoloration. Pleural effusion can be treated surgically, with decortication/pleurectomy or pleurodesis. Antibiotic prophylaxis is prescribed for bronchiectasia with chronic sputum production. Lymphedema treatment is based on low-stretch bandages and the wearing of elastic compression garments combined with skin care, exercises and, as needed, manual lymph drainage. Keywords: Yellow nail syndrome, Respiratory manifestations, Sinusitis, Lymphedema, Review Background Methodology The first case of yellow nail syndrome (YNS; OMIM The literature search of the PubMed database used the 153300, ORPHA662) was probably reported by Heller words “yellow nail syndrome” for articles written in in 1927 [1], but Samman & White described the first English or French.