Basic Dermatologic Presentations
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Hyperhidrosis: Sweating out the Details
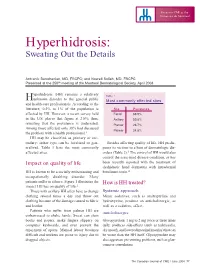
Focus on CME at the Université de Montréal Hyperhidrosis: Sweating Out the Details Antranik Benohanian, MD, FRCPC; and Nowell Solish, MD, FRCPC Presented at the 250th meeting of the Montreal Dermatological Society, April 2003 yperhidrosis (HH) remains a relatively Table 1 Hunknown disorder to the general public Most commonly affected sites and health-care professionals. According to the literature, 0.5% to 1% of the population is Site Prevalence affected by HH. However, a recent survey held Facial 68.9% in the U.S. places that figure at 2.8%; thus, Axillary 50.8% revealing that the prevalence is underrated. Plantar 28.7% Among those affected, only 38% had discussed Palmar 24.8% the problem with a health professional.1 HH may be classified as primary or sec- ondary; either type can be localized or gen- Besides affecting quality of life, HH predis- eralized. Table 1 lists the most commonly poses its victims to a host of dermatologic dis- affected sites. orders (Table 2).3 The control of HH would also control the associated disease condition, as has Impact on quality of life been recently reported with the treatment of dyshidrotic hand dermatitis with intradermal HH is known to be a socially embarrassing and botulinum toxin.4 occupationally disabling disorder. Many patients suffer in silence. Figure 1 illustrates the How is HH treated? impact HH has on quality of life.2 Those with axillary HH often have to change Systemic approach clothing several times a day and throw out Minor sedatives, such as amitriptyline and clothing because of the damage caused to fabric hydroxyzine, produce an anticholinergic, as and leather. -

Skin Manifestation of SARS-Cov-2: the Italian Experience
Journal of Clinical Medicine Article Skin Manifestation of SARS-CoV-2: The Italian Experience Gerardo Cazzato 1 , Caterina Foti 2, Anna Colagrande 1, Antonietta Cimmino 1, Sara Scarcella 1, Gerolamo Cicco 1, Sara Sablone 3, Francesca Arezzo 4, Paolo Romita 2, Teresa Lettini 1 , Leonardo Resta 1 and Giuseppe Ingravallo 1,* 1 Section of Pathology, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] (G.C.); [email protected] (A.C.); [email protected] (A.C.); [email protected] (S.S.); [email protected] (G.C.); [email protected] (T.L.); [email protected] (L.R.) 2 Section of Dermatology and Venereology, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] (C.F.); [email protected] (P.R.) 3 Section of Forensic Medicine, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] 4 Section of Gynecologic and Obstetrics Clinic, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] * Correspondence: [email protected] Abstract: At the end of December 2019, a new coronavirus denominated Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) was identified in Wuhan, Hubei province, China. Less than three months later, the World Health Organization (WHO) declared coronavirus disease-19 (COVID-19) to be a global pandemic. Growing numbers of clinical, histopathological, and molecular findings were subsequently reported, among which a particular interest in skin manifestations during the course of the disease was evinced. Today, about one year after the development of the first major infectious foci in Italy, various large case series of patients with COVID-19-related skin Citation: Cazzato, G.; Foti, C.; manifestations have focused on skin specimens. -

Shingles (Herpes Zoster) Hives (Urticaria) Psoriasis
Shingles (Herpes Zoster) Shingles starts with burning, tingling, or very sensitive skin. A rash of raised dots develops into painful blisters that last about two weeks. Shingles often occurs on the trunk and buttocks, but can appear anywhere. Most people recover, but pain, numbness, and itching linger for many -- and may last for months, years, or the rest of their lives. Treatment with antiviral drugs, steroids, antidepressants, and topical agents can help. Hives (Urticaria) A common allergic reaction that looks like welts, hives are often itchy, and sometimes stinging or burning. Hives vary in size and may join together to form larger areas. They may appear anywhere and last minutes or days. Medications, foods, food additives, temperature extremes, and infections like strep throat are some causes of hives. Antihistamines can provide relief. Psoriasis A non-contagious rash of thick red plaques covered with white or silvery scales, psoriasis usually affects the scalp, elbows, knees, and lower back. The rash can heal and recur throughout life. The cause of psoriasis is unknown, but the immune system triggers new skin cells to develop too quickly. Treatments include medications applied to the skin, light therapy, and medications taken by mouth, injection or infusion. Eczema Eczema describes several non-contagious conditions where skin is inflamed, red, dry, and itchy. Stress, irritants (like soaps), allergens, and climate can trigger flare-ups though they're not eczema's exact cause, which is unknown. In adults, eczema often occurs on the elbows and hands, and in "bending" areas, such as inside the elbows. Treatments include topical or oral medications and shots. -

BETA Betamethasone Valerate Cream 0.1% W/W Betamethasone Valerate Ointment 0.1% W/W
NEW ZEALAND CONSUMER MEDICINE INFORMATION BETA Betamethasone valerate cream 0.1% w/w Betamethasone valerate ointment 0.1% w/w discoid lupus Some of the symptoms of an What is in this leaflet erythematosus (recurring allergic reaction may include: scaly rash) shortness of breath; wheezing or This leaflet answers some common prickly heat skin reaction difficulty breathing; swelling of the questions about BETA Cream and insect bite reactions face, lips, tongue or other parts of Ointment. prurigo nodularis (an itching the body; rash, itching or hives on and thickening of the skin the skin. It does not contain all the available with lumps or nodules) information. It does not take the contact sensitivity reactions Do not use BETA Cream or place of talking to your doctor or an additional treatment for Ointment to treat any of the pharmacist. an intense widespread following skin problems as it reddening and inflammation could make them worse: All medicines have risks and of the skin, infected skin (unless the benefits. Your doctor has weighed when milder topical corticosteroids infection is being treated the risks of you using BETA Cream cannot treat the skin condition with an anti-infective or Ointment against the benefits effectively. medicine at the same time) they expect it will have for you. acne BETA Cream is usually used to rosacea (a facial skin If you have any concerns about treat skin conditions on moist condition where the nose, taking this medicine, ask your surfaces; BETA Ointment is usually cheeks, chin, forehead or doctor or pharmacist. used to treat skin conditions on dry, entire face are unusually scaly skin. -
![Nonbacterial Pus-Forming Diseases of the Skin Robert Jackson,* M.D., F.R.C.P[C], Ottawa, Ont](https://docslib.b-cdn.net/cover/6901/nonbacterial-pus-forming-diseases-of-the-skin-robert-jackson-m-d-f-r-c-p-c-ottawa-ont-246901.webp)
Nonbacterial Pus-Forming Diseases of the Skin Robert Jackson,* M.D., F.R.C.P[C], Ottawa, Ont
Nonbacterial pus-forming diseases of the skin Robert Jackson,* m.d., f.r.c.p[c], Ottawa, Ont. Summary: The formation of pus as a Things are not always what they seem Fungus result of an inflammatory response Phaedrus to a bacterial infection is well known. North American blastomycosis, so- Not so well appreciated, however, The purpose of this article is to clarify called deep mycosis, can present with a is the fact that many other nonbacterial the clinical significance of the forma¬ verrucous proliferating and papilloma- agents such as certain fungi, viruses tion of pus in various skin diseases. tous plaque in which can be seen, par- and parasites may provoke pus Usually the presence of pus in or on formation in the skin. Also heat, the skin indicates a bacterial infection. Table I.Causes of nonbacterial topical applications, systemically However, by no means is this always pus-forming skin diseases administered drugs and some injected true. From a diagnostic and therapeutic Fungus materials can do likewise. Numerous point of view it is important that physi¬ skin diseases of unknown etiology cians be aware of the nonbacterial such as pustular acne vulgaris, causes of pus-forming skin diseases. North American blastomycosis pustular psoriasis and pustular A few definitions are required. Pus dermatitis herpetiformis can have is a yellowish [green]-white, opaque, lymphangitic sporotrichosis bacteriologically sterile pustules. The somewhat viscid matter (S.O.E.D.). Pus- cervicofacial actinomycosis importance of considering nonbacterial forming diseases are those in which Intermediate causes of pus-forming conditions of pus can be seen macroscopicaily. -

Erythema Annulare Centrifugum ▪ Erythema Gyratum Repens ▪ Exfoliative Erythroderma Urticaria ▪ COMMON: 15% All Americans
Cutaneous Signs of Internal Malignancy Ted Rosen, MD Professor of Dermatology Baylor College of Medicine Disclosure/Conflict of Interest ▪ No relevant disclosures ▪ No conflicts of interest Objectives ▪ Recognize common disorders associated with internal malignancy ▪ Manage cutaneous disorders in the context of associated internal malignancy ▪ Differentiate cutaneous signs of leukemia and lymphoma ▪ Understand spidemiology of cutaneous metastases Cutaneous Signs of Internal Malignancy ▪ General physical examination ▪ Pallor (anemia) ▪ Jaundice (hepatic or cholestatic disease) ▪ Fixed erythema or flushing (carcinoid) ▪ Alopecia (diffuse metastatic disease) ▪ Itching (excoriations) Anemia: Conjunctival pallor and Pale skin Jaundice 1-12% of hepatocellular, biliary tree or pancreatic cancer PRESENT with jaundice, but up to 40-60% eventually develop it World J Gastroenterol 2003;9:385-91 For comparison CAN YOU TELL JAUNDICE FROM NORMAL SKIN? JAUNDICE Alopecia Neoplastica Most common report w/ breast CA Lung, cervix, desmoplastic mm Hair loss w/ underlying induration Biopsy = dermis effaced by tumor Ann Dermatol 26:624, 2014 South Med J 102:385, 2009 Int J Dermatol 46:188, 2007 Acta Derm Venereol 87:93, 2007 J Eur Acad Derm Venereol 18:708, 2004 Gastric Adenocarcinoma: Alopecia Ann Dermatol 2014; 26: 624–627 Pruritus: Excoriation ▪ Overall risk internal malignancy presenting as itch LOW. OR =1.14 ▪ CTCL, Hodgkin’s & NHL, Polycythemia vera ▪ Biliary tree carcinoma Eur J Pain 20:19-23, 2016 Br J Dermatol 171:839-46, 2014 J Am Acad Dermatol 70:651-8, 2014 Non-specific (Paraneoplastic) Specific (Metastatic Disease) Paraneoplastic Signs “Curth’s Postulates” ▪ Concurrent onset (temporal proximity) ▪ Parallel course ▪ Uniform site or type of neoplasm ▪ Statistical association ▪ Genetic linkage (syndromal) Curth HO. -

Sexually Transmitted Diseases
Sexually Transmitted Diseases by John H. Dirckx, M.D. significant proportion of the modern practice of adult using condoms and avoiding high-risk behaviors such as anal gynecology and urology is devoted to the prevention, intercourse—and by limiting the number of sex partners. Adiagnosis, and treatment of sexually transmitted dis- The overall incidence of sexually transmitted infections eases (STDs), because of both the high prevalence of these has increased substantially during the past generation, and diseases and their almost exclusive involvement of the repro- some diseases have shown a marked increase. Several factors ductive systems in both sexes. have contributed to these changing statistics. The discovery in A sexually transmitted disease is any infectious disease the 1940s that penicillin could cure syphilis and gonorrhea and that is transmitted from one person to another through sexual the development during the 1950s of safe and effective oral contact, taking that phrase in its broadest sense. Venereal dis- contraceptives paved the way for the sexual revolution of the ease (VD), a synonymous term, has now largely fallen out of 1960s. Against a background of civil unrest, widespread drug use, as has the euphemism social disease. It is worth empha- abuse, and radical feminism, that revolution led to social sizing that the only thing all STDs have in common is their acceptance of sexual promiscuity, popularization of oral and mode of transmission. In other respects they vary widely anal sex, and definition of overt homosexuality as normal among themselves. The common tendency to lump them all behavior. together yields a biologically invalid concept that invites con- Other factors favoring sexual promiscuity have been the fusion and misunderstanding. -

Drug Eruptions.Pdf
Drug eruptions & reactions What are drug eruptions? Drug reactions are unwanted and unexpected reactions occurring in the skin (and sometimes other organ systems) that may result from taking a medication for the prevention, diagnosis or treatment of a medical problem. They may appear after the correct use of the medication or drug. It may also appear due to overdose (wrong dose is taken), following accumulation of drugs in the body over time, or by interactions with other medications being taken or used by the person. Drug eruptions could be caused by an allergy or hypersensitivity to the drug, by a direct toxic effect of the drug or medication on the skin, or by other mechanisms. Drug eruptions vary in severity – from a minor nuisance to a more severe problem – and may even cause death. Drug eruptions occur in up to 15% of courses of drug prescribed by medical or natural therapy practitioners. What causes drug eruptions? Drug eruptions are caused by medications which are prescribed by your doctor, purchased over-the- counter or purchased as compounded herbal/naturopathic medicines. Drugs taken orally, injected, delivered by patch application, rubbed onto the skin (e.g. creams, ointments and lotions) can all cause reactions. The potential to develop an adverse reaction to a drug is influenced by the age, gender and genetic makeup of the person; the nature of the condition being treated; and the possible interactions with other medications being taken. Some classes of drugs are known to cause drug eruptions more commonly than others. What do drug eruptions look like in the skin? The appearance of drug eruptions varies depending on the mechanism of the drug reaction. -

Herpes: a Patient's Guide
Herpes: A Patient’s Guide Herpes: A Patient’s Guide Introduction Herpes is a very common infection that is passed through HSV-1 and HSV-2: what’s in a name? ....................................................................3 skin-to-skin contact. Canadian studies have estimated that up to 89% of Canadians have been exposed to herpes simplex Herpes symptoms .........................................................................................................4 type 1 (HSV-1), which usually shows up as cold sores on the Herpes transmission: how do you get herpes? ................................................6 mouth. In a British Columbia study, about 15% of people tested positive for herpes simplex type 2 (HSV-2), which Herpes testing: when is it useful? ..........................................................................8 is the type of herpes most commonly thought of as genital herpes. Recently, HSV-1 has been showing up more and Herpes treatment: managing your symptoms ...................................................10 more on the genitals. Some people can have both types of What does herpes mean to you: receiving a new diagnosis ......................12 herpes. Most people have such minor symptoms that they don’t even know they have herpes. What does herpes mean to you: accepting your diagnosis ........................14 While herpes is very common, it also carries a lot of stigma. What does herpes mean to you: dating with herpes ....................................16 This stigma can lead to anxiety, fear and misinformation -

Fundamentals of Dermatology Describing Rashes and Lesions
Dermatology for the Non-Dermatologist May 30 – June 3, 2018 - 1 - Fundamentals of Dermatology Describing Rashes and Lesions History remains ESSENTIAL to establish diagnosis – duration, treatments, prior history of skin conditions, drug use, systemic illness, etc., etc. Historical characteristics of lesions and rashes are also key elements of the description. Painful vs. painless? Pruritic? Burning sensation? Key descriptive elements – 1- definition and morphology of the lesion, 2- location and the extent of the disease. DEFINITIONS: Atrophy: Thinning of the epidermis and/or dermis causing a shiny appearance or fine wrinkling and/or depression of the skin (common causes: steroids, sudden weight gain, “stretch marks”) Bulla: Circumscribed superficial collection of fluid below or within the epidermis > 5mm (if <5mm vesicle), may be formed by the coalescence of vesicles (blister) Burrow: A linear, “threadlike” elevation of the skin, typically a few millimeters long. (scabies) Comedo: A plugged sebaceous follicle, such as closed (whitehead) & open comedones (blackhead) in acne Crust: Dried residue of serum, blood or pus (scab) Cyst: A circumscribed, usually slightly compressible, round, walled lesion, below the epidermis, may be filled with fluid or semi-solid material (sebaceous cyst, cystic acne) Dermatitis: nonspecific term for inflammation of the skin (many possible causes); may be a specific condition, e.g. atopic dermatitis Eczema: a generic term for acute or chronic inflammatory conditions of the skin. Typically appears erythematous, -

Skin Disease and Disorders
Sports Dermatology Robert Kiningham, MD, FACSM Department of Family Medicine University of Michigan Health System Disclosures/Conflicts of Interest ◼ None Goals and Objectives ◼ Review skin infections common in athletes ◼ Establish a logical treatment approach to skin infections ◼ Discuss ways to decrease the risk of athlete’s acquiring and spreading skin infections ◼ Discuss disqualification and return-to-play criteria for athletes with skin infections ◼ Recognize and treat non-infectious skin conditions in athletes Skin Infections in Athletes ◼ Bacterial ◼ Herpetic ◼ Fungal Skin Infections in Athletes ◼ Very common – most common cause of practice-loss time in wrestlers ◼ Athletes are susceptible because: – Prone to skin breakdown (abrasions, cuts) – Warm, moist environment – Close contacts Cases 1 -3 ◼ 21 year old male football player with 4 day h/o left axillary pain and tenderness. Two days ago he noticed a tender “bump” that is getting bigger and more tender. ◼ 16 year old football player with 3 day h/o mildly tender lesions on chin. Started as a single lesion, but now has “spread”. Over the past day the lesions have developed a dark yellowish crust. ◼ 19 year old wrestler with a 3 day h/o lesions on right side of face. Noticed “tingling” 4 days ago, small fluid filled lesions then appeared that have now started to crust over. Skin Infections Bacterial Skin Infections ◼ Cellulitis ◼ Erysipelas ◼ Impetigo ◼ Furunculosis ◼ Folliculitis ◼ Paronychea Cellulitis Cellulitis ◼ Diffuse infection of connective tissue with severe inflammation of dermal and subcutaneous layers of the skin – Triad of erythema, edema, and warmth in the absence of underlying foci ◼ S. aureus or S. pyogenes Erysipelas Erysipelas ◼ Superficial infection of the dermis ◼ Distinguished from cellulitis by the intracutaneous edema that produces palpable margins of the skin. -

“The Red Face” and More Clinical Pearls
“The Red Face” and More Clinical Pearls Courtney R. Schadt, MD, FAAD Assistant Professor Residency Program Director University of Louisville Associates in Dermatology I have no disclosures or conflicts of interest Part 1: The Red Face: Objectives • Distinguish and diagnose common eruptions of the face • Recognize those with potential implications for internal disease • Learn basic treatment options Which patient(s) has an increased risk of hypertension and hyperlipidemia? A B C Which patient(s) has an increased risk of hypertension and hyperlipidemia? A Seborrheic Dermatitis B C Psoriasis Seborrheic Dermatitis Goodheart HP. Goodheart's photoguide of common skin disorders, 2nd ed, Lippincott Williams & Wilkins, Philadelphia 2003. Copyright © 2003 Lippincott Williams & Wilkins. Seborrheic Dermatitis • Erythematous scaly eruption • Infants= “Cradle Cap” • Reappear in adolescence or later in life • Chronic, remissions and flares; worse with stress, cold weather • Occurs on areas of body with increased sebaceous glands • Unclear role of Malassezia; could be immune response; no evidence of overgrowth Seborrheic Dermatitis Severe Seb Derm: THINK: • HIV (can also be more diffuse on trunk) • Parkinson’s (seb derm improves with L-dopa therapy) • Other neurologic disorders • Neuroleptic agents • Unclear etiology 5MinuteClinicalConsult Clinical Exam • Erythema/fine scale • Scalp • Ears • Nasolabial folds • Beard/hair bearing areas Goodheart HP. Goodheart's photoguide of common skin disorders, 2nd ed, Lippincott • Ill-defined Williams & Wilkins, Philadelphia