Allergies, Hives, and Rashes, 509K
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Contact Vitiligo Following Allergic Contact Dermatitis *Ricardo Ruiz-Villaverde, Francisco J Navarro-Triviño
SUBMITTED 19 JAN 21 REVISION REQ. 17 MAR 21; REVISION 5 APR 21 ACCEPTED 21 APR 21 ONLINE-FIRST: MAY 2021 DOI: https://doi.org/10.18295/squmj.5.2021.078 Contact Vitiligo Following Allergic Contact Dermatitis *Ricardo Ruiz-Villaverde, Francisco J Navarro-Triviño Department of Dermatology, Hospital Universitario San Cecilio, Granada, Spain *Corresponding Author’s e-mail: [email protected] Introduction A 45-year-old man, construction worker, with no personal history of psoriasis, atopic dermatitis, and vitiligo, was referred to our Contact Eczema Department with a chronic hand eczema and skin depigmentation over a period of 12 months. Skin depigmentation appeared few months later regarding the primary eczema. The patient reported the use of rubber gloves for many years. He had noticed itching and mild erythema over both hands. Currently, he wears nitrile gloves at work. Physical examination showed symmetric erythematous-squamous, hyperkeratotic and fissured plaques on both hands (Fig. 1A), and ventral aspect of wrists (Fig. 1B). Skin depigmentation areas showed irregular edges (Fig. 1C). Wood´s lamp examination accentuated the depigmentation areas overlap the eczema (Fig. 2A-B), without vitiligo pattern. No other anatomical sites were involved. Blood test showed no significant alterations, including data from autoimmune thyroiditis, celiac disease, and pernicious anaemia. Patch tests were performed with the European Comprehensive Baseline Series (Chemotechnique Diagnostics, Vellinge, Sweden), rubber additives series (Chemotechnique Diagnostics), and hydroquinone monobenzylether 1% pet (Shoe series, Chemotechnique Diagnosis). The results were interpreted according to the criteria of the International Contact Dermatitis Research Group. Patch tests were read on day (D) 2 and D4. -

Autoimmune Associations of Alopecia Areata in Pediatric Population - a Study in Tertiary Care Centre
IP Indian Journal of Clinical and Experimental Dermatology 2020;6(1):41–44 Content available at: iponlinejournal.com IP Indian Journal of Clinical and Experimental Dermatology Journal homepage: www.innovativepublication.com Original Research Article Autoimmune associations of alopecia areata in pediatric population - A study in tertiary care centre Sagar Nawani1, Teki Satyasri1,*, G. Narasimharao Netha1, G Rammohan1, Bhumesh Kumar1 1Dept. of Dermatology, Venereology & Leprosy, Gandhi Medical College, Secunderabad, Telangana, India ARTICLEINFO ABSTRACT Article history: Alopecia areata (AA) is second most common disease leading to non scarring alopecia . It occurs in Received 21-01-2020 many patterns and can occur on any hair bearing site of the body. Many factors like family history, Accepted 24-02-2020 autoimmune conditions and environment play a major role in its etio-pathogenesis. Histopathology shows Available online 29-04-2020 bulbar lymphocytes surrounding either terminal hair or vellus hair resembling ”swarm of bees” appearance depending on chronicity of alopecia areata. Alopecia areata in children is frequently seen. Pediatric AA has been associated with atopy, thyroid abnormalities and a positive family history. We have done a study to Keywords: find out if there is any association between alopecia areata and other auto immune diseases in children. This Alopecia areata study is an observational study conducted in 100 children with AA to determine any associated autoimmune Auto immunity conditions in them. SALT score helps to assess severity of alopecia areata. Severity of alopecia areata was Pediatric population assessed by SALT score-1. S1- less than 25% of hairloss, 2. S2- 25-49% of hairloss, 3. 3.S3- 50-74% of hairloss. -

The Tumor Necrosis Factor Superfamily Molecule LIGHT Promotes Keratinocyte Activity and Skin Fibrosis Rana Herro1, Ricardo Da S
ORIGINAL ARTICLE The Tumor Necrosis Factor Superfamily Molecule LIGHT Promotes Keratinocyte Activity and Skin Fibrosis Rana Herro1, Ricardo Da S. Antunes1, Amelia R. Aguilera1, Koji Tamada2 and Michael Croft1 Several inflammatory diseases including scleroderma and atopic dermatitis display dermal thickening, epidermal hypertrophy, or excessive accumulation of collagen. Factors that might promote these features are of interest for clinical therapy. We previously reported that LIGHT, a TNF superfamily molecule, mediated collagen deposition in the lungs in response to allergen. We therefore tested whether LIGHT might similarly promote collagen accumulation and features of skin fibrosis. Strikingly, injection of recombinant soluble LIGHT into naive mice, either subcutaneously or systemically, promoted collagen deposition in the skin and dermal and epidermal thickening. This replicated the activity of bleomycin, an antibiotic that has been previously used in models of scleroderma in mice. Moreover skin fibrosis induced by bleomycin was dependent on endogenous LIGHT activity. The action of LIGHT in vivo was mediated via both of its receptors, HVEM and LTβR, and was dependent on the innate cytokine TSLP and TGF-β. Furthermore, we found that HVEM and LTβR were expressed on human epidermal keratinocytes and that LIGHT could directly promote TSLP expression in these cells. We reveal an unappreciated activity of LIGHT on keratinocytes and suggest that LIGHT may be an important mediator of skin inflammation and fibrosis in diseases such as scleroderma -

Genital Lichen Simplex Chronicus (Eczema, Neurodermatitis, Dermatitis) !
Libby Edwards, MD Genital Lichen Simplex Chronicus (eczema, neurodermatitis, dermatitis) ! Lichen simplex chronicus (LSC), or eczema, is a common skin condition that is very itchy. Although not dangerous in any way, both the itching, and the pain from rubbing and scratching, can be miserable. Eczema/LSC of the genital area most often affects the scrotum of men, the vulva of women, or the rectal skin of both. Many people with eczema/LSC have had sensitive skin or eczema/LSC on other areas of the skin at some point, and many have a tendency towards allergies, especially hay fever or asthma. ! The skin usually appears red or dark, and thick from rubbing and scratching, sometimes with sores from scratching. ! The cause of eczema/LSC is not entirely clear. However, eczema/LSC starts with irritation that triggers itching. Often, at the office visit with the health care provider, the original infection or other initial cause of irritation is no longer present. Common triggers include a yeast or fungus infection, an irritating medication, moisturizer or lubricant, a wet bathing suit, anxiety or depression, over-washing, panty liners, sweat, heat, urine, a contraceptive jelly, an irritating condom, or any other activity or substance that can irritate the skin and start the itching. ! Although rubbing and scratching often feel good at first, rubbing irritates the skin and ultimately makes itching even worse, so that there is more scratching, then more itching, then more scratching. This is called the “itch-scratch cycle.” Treatment is very effective and requires clearing any infection and avoiding irritants as well as using a strong cortisone. -

Cutaneous Manifestations of HIV Infection Carrie L
Chapter Title Cutaneous Manifestations of HIV Infection Carrie L. Kovarik, MD Addy Kekitiinwa, MB, ChB Heidi Schwarzwald, MD, MPH Objectives Table 1. Cutaneous manifestations of HIV 1. Review the most common cutaneous Cause Manifestations manifestations of human immunodeficiency Neoplasia Kaposi sarcoma virus (HIV) infection. Lymphoma 2. Describe the methods of diagnosis and treatment Squamous cell carcinoma for each cutaneous disease. Infectious Herpes zoster Herpes simplex virus infections Superficial fungal infections Key Points Angular cheilitis 1. Cutaneous lesions are often the first Chancroid manifestation of HIV noted by patients and Cryptococcus Histoplasmosis health professionals. Human papillomavirus (verruca vulgaris, 2. Cutaneous lesions occur frequently in both adults verruca plana, condyloma) and children infected with HIV. Impetigo 3. Diagnosis of several mucocutaneous diseases Lymphogranuloma venereum in the setting of HIV will allow appropriate Molluscum contagiosum treatment and prevention of complications. Syphilis Furunculosis 4. Prompt diagnosis and treatment of cutaneous Folliculitis manifestations can prevent complications and Pyomyositis improve quality of life for HIV-infected persons. Other Pruritic papular eruption Seborrheic dermatitis Overview Drug eruption Vasculitis Many people with human immunodeficiency virus Psoriasis (HIV) infection develop cutaneous lesions. The risk of Hyperpigmentation developing cutaneous manifestations increases with Photodermatitis disease progression. As immunosuppression increases, Atopic Dermatitis patients may develop multiple skin diseases at once, Hair changes atypical-appearing skin lesions, or diseases that are refractory to standard treatment. Skin conditions that have been associated with HIV infection are listed in Clinical staging is useful in the initial assessment of a Table 1. patient, at the time the patient enters into long-term HIV care, and for monitoring a patient’s disease progression. -

Chronic Paronychia Refers to a Skin Condition, Which Occurs Around the Nails
Robert E. Kalb, M.D. Buffalo Medical Group, P.C. Phone: (716) 630-1102 Fax: (716) 633-6507 Department of Dermatology 325 Essjay Road Williamsville, New York 14221 PARONYCHIA (CHRONIC) Chronic paronychia refers to a skin condition, which occurs around the nails. The term chronic means that the condition can come and go over time. The word paronychia is a fancy medical term referring to the inflammation, redness and swelling that can occur around the nails. Chronic paronychia occurs most commonly in people whose hands are in a wet environment, for example nurses, bartenders, dishwashers and hairdressers. Repeated cuts and minor trauma of the skin can damage the area around the nail and in the cuticle. This minor damage allows further irritation. There can be overgrowth of various surface germs, which slow the healing process. Symptoms of chronic paronychia include loss of the cuticle, tenderness, redness and swelling. Often the nails can appear changed with rough surfaces or grooves. Sometimes the area around the nail can be colonized with a normal bacteria or yeast on the skin. Because of this, one of the treatments that is often used is a medication, which has antibiotic properties against these types of organisms. In many cases, it is not an actual infection, but simply colonization on the surface of the skin, which impedes the healing. Treatment of chronic paronychia starts by avoiding any chronic irritation or wet environments. Wearing cotton-lined gloves to wash dishes can be helpful if this is an exposure. In most cases, topical medications are used. These often involve two different creams or two different liquids. -

Scalp Eczema Factsheet the Scalp Is an Area of the Body That Can Be Affected by Several Types of Eczema
12 Scalp eczema factsheet The scalp is an area of the body that can be affected by several types of eczema. The scalp may be dry, itchy and scaly in a chronic phase and inflamed (red), weepy and painful in an acute (eczema flare) phase. Aside from eczema, there are a number of reasons why the scalp can become dry and itchy (e.g. psoriasis, fungal infection, ringworm, head lice etc.), so it is wise to get a firm diagnosis if there is uncertainty. Types of eczema • Hair clips and headgear – especially those containing that affect the scalp rubber or nickel. Seborrhoeic eczema (dermatitis) is one of the most See the NES booklet on Contact Dermatitis for more common types of eczema seen on the scalp and hairline. details. It can affect babies (cradle cap), children and adults. The Irritant contact dermatitis is a type of eczema that skin appears red and scaly and there is often dandruff as occurs when the skin’s surface is irritated by a substance well, which can vary in severity. There may also be a rash that causes the skin to become dry, red and itchy. on other parts of the face, such as around the eyebrows, For example, shampoos, mousses, hair gels, hair spray, eyelids and sides of the nose. Seborrhoeic eczema can perm solution and fragrance can all cause irritant contact become infected. See the NES factsheets on Adult dermatitis. See the NES booklet on Contact Dermatitis for Seborrhoeic Dermatitis and Infantile Seborrhoeic more details. Dermatitis and Cradle Cap for more details. -

Skin Manifestation of SARS-Cov-2: the Italian Experience
Journal of Clinical Medicine Article Skin Manifestation of SARS-CoV-2: The Italian Experience Gerardo Cazzato 1 , Caterina Foti 2, Anna Colagrande 1, Antonietta Cimmino 1, Sara Scarcella 1, Gerolamo Cicco 1, Sara Sablone 3, Francesca Arezzo 4, Paolo Romita 2, Teresa Lettini 1 , Leonardo Resta 1 and Giuseppe Ingravallo 1,* 1 Section of Pathology, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] (G.C.); [email protected] (A.C.); [email protected] (A.C.); [email protected] (S.S.); [email protected] (G.C.); [email protected] (T.L.); [email protected] (L.R.) 2 Section of Dermatology and Venereology, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] (C.F.); [email protected] (P.R.) 3 Section of Forensic Medicine, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] 4 Section of Gynecologic and Obstetrics Clinic, University of Bari ‘Aldo Moro’, 70121 Bari, Italy; [email protected] * Correspondence: [email protected] Abstract: At the end of December 2019, a new coronavirus denominated Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) was identified in Wuhan, Hubei province, China. Less than three months later, the World Health Organization (WHO) declared coronavirus disease-19 (COVID-19) to be a global pandemic. Growing numbers of clinical, histopathological, and molecular findings were subsequently reported, among which a particular interest in skin manifestations during the course of the disease was evinced. Today, about one year after the development of the first major infectious foci in Italy, various large case series of patients with COVID-19-related skin Citation: Cazzato, G.; Foti, C.; manifestations have focused on skin specimens. -

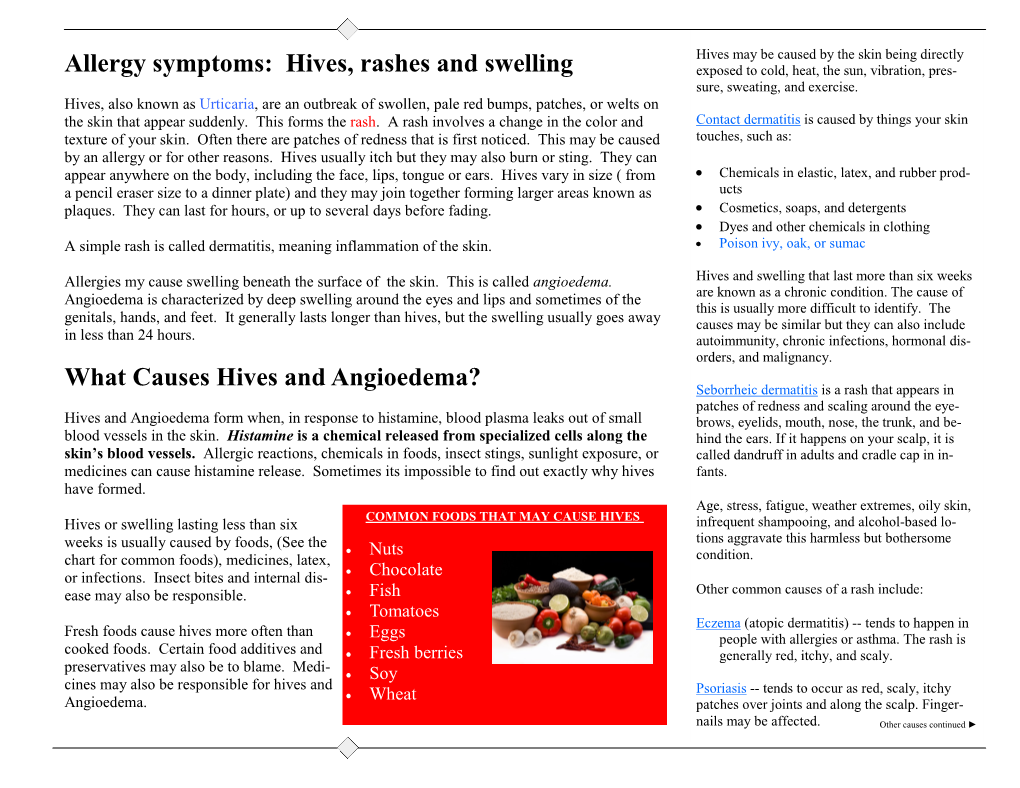
Shingles (Herpes Zoster) Hives (Urticaria) Psoriasis
Shingles (Herpes Zoster) Shingles starts with burning, tingling, or very sensitive skin. A rash of raised dots develops into painful blisters that last about two weeks. Shingles often occurs on the trunk and buttocks, but can appear anywhere. Most people recover, but pain, numbness, and itching linger for many -- and may last for months, years, or the rest of their lives. Treatment with antiviral drugs, steroids, antidepressants, and topical agents can help. Hives (Urticaria) A common allergic reaction that looks like welts, hives are often itchy, and sometimes stinging or burning. Hives vary in size and may join together to form larger areas. They may appear anywhere and last minutes or days. Medications, foods, food additives, temperature extremes, and infections like strep throat are some causes of hives. Antihistamines can provide relief. Psoriasis A non-contagious rash of thick red plaques covered with white or silvery scales, psoriasis usually affects the scalp, elbows, knees, and lower back. The rash can heal and recur throughout life. The cause of psoriasis is unknown, but the immune system triggers new skin cells to develop too quickly. Treatments include medications applied to the skin, light therapy, and medications taken by mouth, injection or infusion. Eczema Eczema describes several non-contagious conditions where skin is inflamed, red, dry, and itchy. Stress, irritants (like soaps), allergens, and climate can trigger flare-ups though they're not eczema's exact cause, which is unknown. In adults, eczema often occurs on the elbows and hands, and in "bending" areas, such as inside the elbows. Treatments include topical or oral medications and shots. -

Concurrent Beau Lines, Onychomadesis, and Retronychia Following Scurvy
CASE REPORT Concurrent Beau Lines, Onychomadesis, and Retronychia Following Scurvy Dayoung Ko, BS; Shari R. Lipner, MD, PhD the proximal nail plate from the distal nail plate leading to shedding of the nail. It occurs due to a complete growth PRACTICE POINTS arrest in the nail matrix and is thought to be on a con- • Beau lines, onychomadesis, and retronychia are nail tinuum with Beau lines. The etiologies of these 2 condi- conditions with distinct clinical findings. tions overlap and include trauma, inflammatory diseases, • Beau lines and onychomadesis may be seen 1-5 concurrently following trauma, inflammatory dis- systemic illnesses, hereditary conditions, and infections. eases, systemic illnesses, hereditary conditions, In almost all cases of both conditions, normal nail plate and infections. production ensues upon identification and removal of the 3,4,6 • Retronychia shares a common pathophysiology inciting agent or recuperation from the causal illness. with Beau lines and onychomadesis, and all reflect Beau lines will move distally as the nail grows out and slowing or cessation of nail plate production. can be clipped. In onychomadesis, the affected nails will be shed with time. Resolution of these nail defects can be estimated from average nail growth rates (1 mm/mo for fingernails and 2–3 mm/mo for toenails).7 Beau lines, onychomadesis, and retronychia are nail conditions with Retronychia is defined as a proximal ingrowing of their own characteristic clinical findings. It has been hypothesized the nail plate into the ventral surface of the proximal nail that these 3 disorders may share a common pathophysiologic fold.4,6 It is thought to occur via vertical progression of mechanism of slowing and/or halting nail plate production at the the nail plate into the proximal nail fold, repetitive nail nail matrix. -

Allergy and Immunology Milestones
Allergy and Immunology Milestones The Accreditation Council for Graduate Medical Education Second Revision: August 2019 First Revision: August 2013 Allergy and Immunology Milestones The Milestones are designed only for use in evaluation of residents in the context of their participation in ACGME-accredited residency or fellowship programs. The Milestones provide a framework for the assessment of the development of the resident in key dimensions of the elements of physician competency in a specialty or subspecialty. They neither represent the entirety of the dimensions of the six domains of physician competency, nor are they designed to be relevant in any other context. i Allergy and Immunology Milestones Work Group Amal Assa’ad, MD Evelyn Lomasney, MD Taylor Atchley, MD Aidan Long, MD T. Prescott Atkinson, MD, PhD Mike Nelson, MD Laura Edgar, EdD, CAE Princess Ogbogu, MD Beverly Huckman, BA* Kelly Stone, MD, PhD Bruce Lanser, MD The ACGME would like to thank the following organizations for their continued support in the development of the Milestones: American Board of Allergy and Immunology American Academy of Allergy, Asthma, and Immunology Review Committee for Allergy and Immunology *Acknowledgments: The Work Group and the ACGME would like to honor Beverly Huckman, for her contributions as the non-physician member of the milestones work group. She will be greatly missed. ii Understanding Milestone Levels and Reporting This document presents the Milestones, which programs use in a semi-annual review of resident performance, and then report to the ACGME. Milestones are knowledge, skills, attitudes, and other attributes for each of the ACGME Competencies organized in a developmental framework. -

Effectiveness of Medium-Dose Ultraviolet A1 Phototherapy in Localized Scleroderma
Pharmacology and therapeutics Effectiveness of medium-dose ultraviolet A1 phototherapy in localized scleroderma Ozlem Su1, MD, Nahide Onsun1, MD, Hulya Kapran Onay2, MD, Yeliz Erdemoglu1, MD, Dilek Biyik Ozkaya1, MD, Filiz Cebeci1, MD, and Adnan Somay3, MD 1Department of Dermatology, Abstract Bezmialem Vakif University, Faculty of Background Recently, ultraviolet (UV) A1 phototherapy has been suggested as an effec- 2 Medicine, Neoson Imaging Center, tive treatment for localized scleroderma (LS); however, the optimal dose of UVA1 still has Radiology, and 3Department of not been determined. Pathology, Vakif Gureba Teaching and 2 Research Hospital, Istanbul, Turkey Objective We aimed to evaluate the therapeutic effectiveness of medium-dose (30 J/cm ) UVA1 phototherapy and to show that 13 MHz ultrasound is a valuable tool for assessing Correspondence the results of UVA1 phototherapy in LS. Ozlem Su, MD Methods Thirty-five patients with LS were treated with medium-dose (30 J/cm2) UVA1. Sıgırtmac Sok. No. 21 B blok d. 7 In total, 30–45 treatments and 900–1350 J/cm2 cumulative UVA1 doses were evaluated by Osmaniye Bakirkoy clinical scoring in all patients. In 14 patients, skin thickness was also determined by Istanbul 13 MHz ultrasound examination. Turkey Results In all patients, medium-dose UVA1 therapy softened sclerotic plaques, and E-mail: [email protected] marked clinical improvement was observed in 29 of 35 (82. 85%) patients. Ultrasound mea- surements showed that skin thickness was significantly reduced. No side effects were Conflicts of interest: None. observed during or after treatment. Conclusion Medium-dose UVA1 phototherapy is a highly effective, safe, and well-tolerated therapeutic modality for treatment of all types of LS.