Weekly Bulletin on Outbreaks
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses
ARIZONA ARBOVIRAL HANDBOOK FOR CHIKUNGUNYA, DENGUE, AND ZIKA VIRUSES 7/31/2017 Arizona Department of Health Services | P a g e 1 Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses Arizona Arboviral Handbook for Chikungunya, Dengue, and Zika Viruses OBJECTIVES .............................................................................................................. 4 I: CHIKUNGUNYA ..................................................................................................... 5 Chikungunya Ecology and Transmission ....................................... 6 Chikungunya Clinical Disease and Case Management ............... 7 Chikungunya Laboratory Testing .................................................. 8 Chikungunya Case Definitions ...................................................... 9 Chikungunya Case Classification Algorithm ............................... 11 II: DENGUE .............................................................................................................. 12 Dengue Ecology and Transmission .............................................. 14 Dengue Clinical Disease and Case Management ...................... 14 Dengue Laboratory Testing ......................................................... 17 Dengue Case Definitions ............................................................ 19 Dengue Case Classification Algorithm ....................................... 23 III: ZIKA .................................................................................................................. -

Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin
Seasonal Malaria Chemoprevention in Guinea Maya Zhang, Stacy Attah-Poku, Noura Al-Jizawi, Jordan Imahori, Stanley Zlotkin April 2021 This research was made possible through the Reach Alliance, a partnership between the University of Toronto’s Munk School of Global Affairs & Public Policy and the Mastercard Center for Inclusive Growth. Research was also funded by the Ralph and Roz Halbert Professorship of Innovation at the Munk School of Global Affairs & Public Policy. We express our gratitude and appreciation to those we met and interviewed. This research would not have been possible without the help of Dr. Paul Milligan from the London School of Hygiene and Tropical Medicine, ACCESS-SMC, Catholic Relief Services, the Government of Guinea and other individuals and organizations in providing and publishing data and resources. We are also grateful to Dr. Kovana Marcel Loua, director general of the National Institute of Public Health in Guinea and professor at the Gamal Abdel Nasser University of Conakry, Guinea. Dr. Loua was instrumental in the development of this research — advising on key topics, facilitating ethics board approval in Guinea and providing data and resources. This research was vetted by and received approval from the Ethics Review Board at the University of Toronto. Research was conducted during the COVID-19 pandemic in compliance with local public health measures. MASTERCARD CENTER FOR INCLUSIVE GROWTH The Center for Inclusive Growth advances sustainable and equitable economic growth and financial inclusion around the world. Established as an independent subsidiary of Mastercard, we activate the company’s core assets to catalyze action on inclusive growth through research, data philanthropy, programs, and engagement. -
GUINEE - PREFECTURE DE NZEREKORE Carte De La Population Et Des Structures Sanitaires 10 Mars 2021
GUINEE - PREFECTURE DE NZEREKORE Carte de la population et des structures sanitaires 10 mars 2021 BEYLA KOUANKAN BOOLA Boola Kognea Maghana Lomou Ouinzou Kogbata FOUMBADOU SEREDOU Boma Nord Gbana KOROPARA Lomou Gounangalaye Saouro Kpamou Koni Koropara Lokooua Alaminata Foozou Nyema Nord Kabieta Bassa´ta Koroh Keleta Ouleouon WOMEY Pampara Suobaya Bowe Nord NZEBELA Keorah Womey kerezaghaye Zenemouta Beneouli Selo MACENTA Loula Yomata Koule Komata KOULE Pale Yalakpala Tokpata Goueke Voumou LAINE Tamoe Niaragbaleye Kpoulo Pouro Kolata Maoun Wouyene PALE Zogbeanta GOUECKE Dapore Soulouta SOULOUTA Konipara Gouh Nona Banzou Tamoe Kola Kpagalaye Nyenh Koronta Youa Gbouo Kelemanda Zogotta Mahouor Koloda KOBELA KOYAMAH Kpaya Souhoule Kelouenta Poe KOKOTA Filikoele Koola Yleouena Batoata Gbadiou Niambara LOLA SAMOE Niema Komou Niarakpale Gbamba Banota Kpaya YALENZOU Boma Samoe Moata Kounala LOLA CTRE Koule Sud Boma Sud Horoya BOWE NZEREKORE CTRE Dorota Nyalakpale Bangoueta Gonia Nyen Commercial Toulemou Nzerekore Konia Kotozou Wessoua Aviation Mohomuo YOMOU Gbottoye Yalenzou Secteur zaapa Zao Yalenzou Kerema Gbenemou Lomou Centre centre Toulemou POPULATION PAR SOUS-PREFECTURE NZOO Gbenedapah SOUS-PREFECTURE POPULATION 2021 Foromopa BOSSOU Teyeouon Bounouma 27 605 Bounouma Kankore Gouecke 24 056 centre DISTANCES DES DISTRICTS SANITAIRES DE NZEREKORE Kobela 19 080 Centre de santé Distance N’Zérékoré_CS Poste de santé Distance CS_PS Koropara 23 898 KOULE SUD 9KM NYEMA 10 KM Sehipa Koule 23 756 C S SAMOE 12 KM NYAMPARA PELA 9 KM BOUNOUMA Thuo centre -

Uveal Involvement in Marburg Virus Disease B
Br J Ophthalmol: first published as 10.1136/bjo.61.4.265 on 1 April 1977. Downloaded from British Journal of Ophthalmology, 1977, 61, 265-266 Uveal involvement in Marburg virus disease B. S. KUMING AND N. KOKORIS From the Department of Ophthalmology, Johannesburg General Hospital and University of the Witwatersrand SUMMARY The first reported case of uveal involvement in Marburg virus disease is described. 'Ex Africa semper aliquid novi'. Two outbreaks of Marburg virus disease have been Rhodesia and had also been constantly at his documented. The first occurred in Marburg and bedside till his death. Lassa fever was suspected and Frankfurt, West Germany, in 1967 (Martini, 1969) she was given a unit of Lassa fever convalescent and the second in Johannesburg in 1975 (Gear, serum when she became desperately ill on the fifth 1975). This case report describes the third patient day. She also developed acute pancreatitis. Within in the Johannesburg outbreak, who developed an 52 hours she made a dramatic and uneventful anterior uveitis. The cause of the uveitis was proved recovery. Her illness mainly affected the haema- to be the Marburg virus by identiying it in a tissue topoietic, hepatic, and pancreatic systems. culture of her aqueous fluid. The subject of this report was a nurse who had helped to nurse patients 1 and 2. Nine days after the Case report death ofthe first patient she presented with lower back pain and high fever. She developed hepatitis, a mild Before describing the case history of the patient the disseminated intravascular coagulation syndrome, events leading to her contracting the disease must successfully treated with heparin, and the classical be briefly described. -

Guinea : Reference Map of N’Zérékoré Region (As of 17 Fev 2015)
Guinea : Reference Map of N’Zérékoré Region (as of 17 Fev 2015) Banian SENEGAL Albadariah Mamouroudou MALI Djimissala Kobala Centre GUINEA-BISSAU Mognoumadou Morifindou GUINEA Karala Sangardo Linko Sessè Baladou Hérémakono Tininkoro Sirana De Beyla Manfran Silakoro Samala Soromaya Gbodou Sokowoulendou Kabadou Kankoro Tanantou Kerouane Koffra Bokodou Togobala Centre Gbangbadou Koroukorono Korobikoro Koro Benbèya Centre Gbenkoro SIERRA LEONE Kobikoro Firawa Sassèdou Korokoro Frawanidou Sokourala Vassiadou Waro Samarami Worocia Bakokoro Boukorodou Kamala Fassousso Kissidougou Banankoro Bablaro Bagnala Sananko Sorola Famorodou Fermessadou Pompo Damaro Koumandou Samana Deila Diassodou Mangbala Nerewa LIBERIA Beindou Kalidou Fassianso Vaboudou Binemoridou Faïdou Yaradou Bonin Melikonbo Banama Thièwa DjénédouKivia Feredou Yombiro M'Balia Gonkoroma Kemosso Tombadou Bardou Gberékan Sabouya Tèrèdou Bokoni Bolnin Boninfé Soumanso Beindou Bondodou Sasadou Mama Koussankoro Filadou Gnagbèdou Douala Sincy Faréma Sogboro Kobiramadou Nyadou Tinah Sibiribaro Ouyé Allamadou Fouala Regional Capital Bolodou Béindou Touradala Koïko Daway Fodou 1 Dandou Baïdou 1 Kayla Kama Sagnola Dabadou Blassana Kamian Laye Kondiadou Tignèko Kovila Komende Kassadou Solomana Bengoua Poveni Malla Angola Sokodou Niansoumandou Diani District Capital Kokouma Nongoa Koïko Frandou Sinko Ferela Bolodou Famoîla Mandou Moya Koya Nafadji Domba Koberno Mano Kama Baïzéa Vassala Madina Sèmèkoura Bagbé Yendemillimo Kambadou Mohomè Foomè Sondou Diaboîdou Malondou Dabadou Otol Beindou Koindou -

Chikungunya Fever: Epidemiology, Clinical Syndrome, Pathogenesis
Antiviral Research 99 (2013) 345–370 Contents lists available at SciVerse ScienceDirect Antiviral Research journal homepage: www.elsevier.com/locate/antiviral Review Chikungunya fever: Epidemiology, clinical syndrome, pathogenesis and therapy ⇑ Simon-Djamel Thiberville a,b, , Nanikaly Moyen a,b, Laurence Dupuis-Maguiraga c,d, Antoine Nougairede a,b, Ernest A. Gould a,b, Pierre Roques c,d, Xavier de Lamballerie a,b a UMR_D 190 ‘‘Emergence des Pathologies Virales’’ (Aix-Marseille Univ. IRD French Institute of Research for Development EHESP French School of Public Health), Marseille, France b University Hospital Institute for Infectious Disease and Tropical Medicine, Marseille, France c CEA, Division of Immuno-Virologie, Institute of Emerging Diseases and Innovative Therapies, Fontenay-aux-Roses, France d UMR E1, University Paris Sud 11, Orsay, France article info abstract Article history: Chikungunya virus (CHIKV) is the aetiological agent of the mosquito-borne disease chikungunya fever, a Received 7 April 2013 debilitating arthritic disease that, during the past 7 years, has caused immeasurable morbidity and some Revised 21 May 2013 mortality in humans, including newborn babies, following its emergence and dispersal out of Africa to the Accepted 18 June 2013 Indian Ocean islands and Asia. Since the first reports of its existence in Africa in the 1950s, more than Available online 28 June 2013 1500 scientific publications on the different aspects of the disease and its causative agent have been pro- duced. Analysis of these publications shows that, following a number of studies in the 1960s and 1970s, Keywords: and in the absence of autochthonous cases in developed countries, the interest of the scientific commu- Chikungunya virus nity remained low. -

Dengue Fever and Dengue Hemorrhagic Fever (Dhf)
DENGUE FEVER AND DENGUE HEMORRHAGIC FEVER (DHF) What are DENGUE and DHF? Dengue and DHF are viral diseases transmitted by mosquitoes in tropical and subtropical regions of the world. Cases of dengue and DHF are confirmed every year in travelers returning to the United States after visits to regions such as the South Pacific, Asia, the Caribbean, the Americas and Africa. How is dengue fever spread? Dengue virus is transmitted to people by the bite of an infected mosquito. Dengue cannot be spread directly from person to person. What are the symptoms of dengue fever? The most common symptoms of dengue are high fever for 2–7 days, severe headache, backache, joint pains, nausea and vomiting, eye pain and rash. The rash is frequently not visible in dark-skinned people. Young children typically have a milder illness than older children and adults. Most patients report a non-specific flu-like illness. Many patients infected with dengue will not show any symptoms. DHF is a more severe form of dengue. Initial symptoms are the same as dengue but are followed by bleeding problems such as easy bruising, skin hemorrhages, bleeding from the nose or gums, and possible bleeding of the internal organs. DHF is very rare. How soon after exposure do symptoms appear? Symptoms of dengue can occur from 3-14 days, commonly 4-7 days, after the bite of an infected mosquito. What is the treatment for dengue fever? There is no specific treatment for dengue. Treatment usually involves treating symptoms such as managing fever, general aches and pains. Persons who have traveled to a tropical or sub-tropical region should consult their physician if they develop symptoms. -

Weekly Bulletin on Outbreaks and Other Emergencies
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 28: 05 - 11 July 2021 Data as reported by: 17:00; 11 July 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 1 117 106 12 New event Ongoing events Outbreaks Humanitarian crises 146 082 3 836 Algeria ¤ 1 034 0 6 328 185 Mauritania 1 313 74 14 463 528 48 0 110 0 46 175 1 194 Niger 21 672 489 6 284 29 Mali 21 0 9 0 Cape Verde 6 471 16 4 954 174 Chad Eritrea Senegal 5 538 194 Gambia 66 0 33 006 289 1 414 8 Guinea-Bissau 847 17 Burkina Faso 2 060 56 277 071 4 343 168 552 2 124 Guinea 13 509 168 13 0 3 947 70 2 2 Benin 198 0 Nigeria 1 286 4 61 0 30 0 Ethiopia 13 2 6 995 50 556 5 872 15 Sierra Leone Togo 626 0 80 858 1 324 Ghana 7 142 98 Côte d'Ivoire 10 879 117 19 000 304 81 0 45 0 Liberia 17 0 South Sudan Central African Republic 1 313 2 0 25 0 50 14 0 97 585 801 6 738 221 Cameroon 24 117 299 3 0 48 776 318 35 339 197 7 0 58 0 199 2 1 411 30 9 1 620 1 188 754 3 722 2 0 168 0 1 1 6 031 112 14 270 133 8 790 122 Equatorial Guinea Uganda 867 2 827 9 Sao Tome and Principe 4 0 5 215 144 716 494 198 87 277 2 104 Kenya Gabon Legend Congo 3 516 93 305 26 Rwanda 8 199 104 2 392 37 48 244 560 25 164 162 Democratic Republic of the Congo 12 790 167 Burundi Measles Humanitarian crisis 5 686 8 Seychelles 44 139 980 436 0 693 57 Monkeypox Yellow fever United Republic of Tanzania 197 0 16 957 68 Meningitis Lassa fever 509 21 241 1 6 257 229 Leishmaniasis Cholera 39 958 935 175 729 2 822 Comoros Plague 304 3 cVDPV2 Angola Malawi Diarrhoeal disease in children under five years 36 926 1 250 -

Your Child Or Family Member May Have Dengue Fever According to Their Clinical History and Physical Examination
Your child or family member may have dengue fever according to their clinical history and physical examination. If it is dengue, serious complications of the disease can develop. If the complications are recognized early, and a doctor is consulted, it may save the patient’s life. Your doctor can order more tests to see if the patient needs to be hospitalized. The doctor can also order specific tests for dengue, but those tests will take longer than a week for the results to come back. How to Care for the Patient While They Have a Fever: Bed rest. Let patient rest as much as possible. Control the fever. Give acetaminophen or paracetamol (Tylenol) every 6 hours (maximum 4 doses per day). Do not give ibuprofen (Motrin, Advil) aspirin, or aspirin containing drugs. Sponge patient’s skin with cool water if fever stays high. Prevent dehydration which occurs when a person loses too much fluid (from high fevers, vomiting, or poor oral intake). Give plenty of fluids and watch for signs of dehydration. Bring patient to clinic or emergency room if any of the following signs develop: Decrease in urination (check number of wet diapers or trips to the bathroom) Few or no tears when child cries Dry mouth, tongue or lips Sunken eyes Listlessness or overly agitated or confused Fast heart beat (more than 100/min) Cold or clammy fingers and toes Sunken fontanel in infant DO WHILE THE PATIENT HAS FEVER DO WHILE THE PATIENT Prevent spread of dengue within your house. Place patient under bed net or use insect repellent on the patient while they have a fever. -
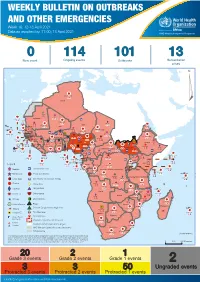
Week 16: 12-18 April 2021
WEEKLY BULLETIN ON OUTBREAKS AND OTHER EMERGENCIES Week 16: 12-18 April 2021 Data as reported by: 17:00; 18 April 2021 REGIONAL OFFICE FOR Africa WHO Health Emergencies Programme 0 114 101 13 New event Ongoing events Outbreaks Humanitarian crises 119 642 3 155 Algeria ¤ 36 13 110 0 5 694 170 Mauritania 7 2 13 070 433 110 0 7 0 Niger 17 129 453 Mali 3 491 10 567 0 6 0 2 079 4 4 706 169 Eritrea Cape Verde 39 782 1 091 Chad Senegal 5 074 189 61 0 Gambia 27 0 3 0 20 466 191 973 5 Guinea-Bissau 847 17 7 0 Burkina Faso 236 49 242 028 3 370 0 164 233 2 061 Guinea 13 129 154 12 38 397 1 3 712 66 1 1 23 12 Benin 30 0 Nigeria 1 873 72 0 Ethiopia 540 2 481 5 6 188 15 Sierra Leone Togo 3 473 296 61 731 919 52 14 Ghana 5 787 75 Côte d'Ivoire 10 473 114 14 484 479 63 0 40 0 Liberia 17 0 South Sudan Central African Republic 916 2 45 0 97 17 25 0 21 612 260 45 560 274 91 709 771 Cameroon 7 0 28 676 137 5 330 13 151 653 2 481 655 2 43 0 119 12 6 1 488 6 4 028 79 12 533 7 259 106 Equatorial Guinea Uganda 542 8 Sao Tome and Principe 32 11 2 066 85 41 378 338 Kenya Legend 7 611 95 Gabon Congo 2 012 73 Rwanda Humanitarian crisis 2 275 35 23 888 325 Measles 21 858 133 Democratic Republic of the Congo 10 084 137 Burundi 3 612 6 Monkeypox Ebola virus disease Seychelles 28 956 745 235 0 420 29 United Republic of Tanzania Lassa fever Skin disease of unknown etiology 190 0 4875 25 509 21 Cholera Yellow fever 1 349 5 6 257 229 24 389 561 cVDPV2 Dengue fever 90 918 1 235 Comoros Angola Malawi COVID-19 Chikungunya 33 941 1 138 862 0 3 815 146 Zambia 133 0 Mozambique -

Viral Hemorrhagic Fevers and Bioterrorism
What you need to know about . Viral Hemorrhagic Fevers and Bioterrorism What are viral hemorrhagic fevers? How are viral hemorrhagic fevers Viral hemorrhagic fevers (VHFs) are a spread? group of illnesses caused by several distinct In nature, viruses causing hemorrhagic fever families of viruses. In general the term typically are passed from mice, rats, fleas “viral hemorrhagic fever” describes severe and ticks to humans. People can be infected problems affecting several organ systems when they come in contact with urine, fecal in the body. Typically, the entire system of ma�er, saliva or other body fluids from blood vessels is damaged, and the body has infected rodents. Fleas and ticks transmit the problems regulating itself. Symptoms o�en viruses when they bite a person or when a include bleeding, but the bleeding itself is person crushes a tick. Hosts for some viruses rarely life-threatening. VHFs are caused by such as Ebola and Marburg are not known. viruses of four families: Some viruses such as Ebola, Marburg and Lassa can be spread from person to person • Arenavirus including Lassa fever and by direct contact with infected blood or Argentine, Bolivian, Brazilian and organs or indirectly through contact with Venezuelan hemorrhagic fevers; objects such as syringes or needles that are • Filovirus including Ebola and Marburg; contaminated with infected body fluids. • Bunyavirus including Hantavirus and Ri� Valley Fever; What are the symptoms? • Flavivirus including yellow fever and Symptoms vary with the different virus dengue fever. families, but first signs o�en include sudden fever, weakness, muscle pain, tiredness, Can viral hemorrhagic fevers be used headache and sore throat. -

A Methodology for Complex Agricultural Development Projects
Systemic Impact Evaluation: A Methodology for Complex Agricultural Development Projects. The Case of a Contract Farming Project in Guinea Jocelyne Delarue, Hubert Cochet To cite this version: Jocelyne Delarue, Hubert Cochet. Systemic Impact Evaluation: A Methodology for Complex Agri- cultural Development Projects. The Case of a Contract Farming Project in Guinea. The European Journal of Development Research, 2013, 25 (5), p.778-796. 10.1057/ejdr.2013.15. halshs-01374496 HAL Id: halshs-01374496 https://halshs.archives-ouvertes.fr/halshs-01374496 Submitted on 7 May 2020 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Original Article Systemic Impact Evaluation: A Methodology for Complex Agricultural Development Projects. The Case of a Contract Farming Project in Guinea Jocelyne Delaruea and Hubert Cochetb aAgence Française de Développement, Evaluation and Capitalization Unit, Paris, France. E-mail: [email protected] bAgro Paris Tech, Comparative Agriculture and Agricultural Development Research Unit, Paris, France. E-mail: [email protected] Abstract This article presents a mixed-method approach used to analyse the impact of a complex agricultural development project, the SOGUIPAH (Guinean Oil Palms and Rubber Company) project designed to promote oil palm and rubber cultivation in Guinea.