Maine Methamphetamine Prevention Toolkit
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2018 Ibangs Meeting: the 20Th Annual Genes, Brain & Behavior Meeting
5/25/2018 Program for Thursday, May 17th 2018 IBANGS MEETING: THE 20TH ANNUAL GENES, BRAIN & BEHAVIOR MEETING WELCOME PROGRAM INDEXES PROGRAM FOR THURSDAY, MAY 17TH Days: next day all days View: session overview talk overview 08:30-16:00 Session FV: Pre-IBANGS Satellite Meeting, Functional Validation for Neurogenetics Location: Phillips Hall in the Siebens building room 1-11. The Siebens building is located at the Downtown Mayo Clinic Campus (not the Mayo Civic Center). Description:The transformative nature of next generation sequencing has changed how neuroscientists approach genomic sequence variation. Highly multiplexed molecular testing is providing an expanded level of information from which to make informed phenotypic predictions. The importance of this is reflected in the unprecedented expansion of genomic testing to determine the basis of neurologic conditions. Genomic testing results in many instances provide a definitive basis of a neurologic condition. However, in almost a high proportion of cases, the genomic sequencing results are confounded by the ambiguity of variants with uncertain clinical significance. Herein lies the key with which institutions will lead in the area of genomic medicine. There exists a critical need to provide a mechanism by which uncertain findings can be functionally characterized and translated into clinically actionable results. It is within thisr ealm that academic societies such as IBANGS can have a substantial and informative role on the future of clinical research and practice. This symposium will introduce the challenges and opportunities that exist in the field of human clinical neurogenetics and follow this with presentations of active work in the field of functional genetic finding validation for neurogenetics with a look to the future of genomic neurogenetics. -

Signs and Symptoms, Biology, and Awareness in This Section
Section 3: Facts about Methamphetamine Signs and Symptoms, Biology, and Awareness In This Section: Basic Facts about Methamphetamine, Source: This information was accessed in 2011 from www.methresources.gov which now redirects to the ONDCP website (2012). Signs and Symptoms of Methamphetamine, Source: This information was accessed in 2011 from NIDA InfoFacts: Methamphetamine which is no longer available on the NIDA website. Anatomy of a Meth User, www.kci.org Methamphetamine Abuse and Addiction, National Institute on Drug Abuse (NIDA) Research Report Series http://www.nida.nih.gov/PDF/RRMetham.pdf Methamphetamine and Teens, Source: This information was accessed in 2011 from www.theantidrug.com which now redirects to www.drugfree.org. Biology, Behavior and the Brain: Methamphetamine Addiction, Source: This information was accessed in 2011 from www.nationalmethcenter.org, a website which is now disabled. Links: Frontline: The Meth Epidemic, www.pbs.org/wgbh/pages/frontline/meth/ (video) NIDA Drug Facts: Methamphetamine, www.drugabuse.gov/drugs-abuse/methamphetamine NIDA Drug of Abuse: Methamphetamine, www.drugabuse.gov/publications/drugfacts/methamphetamine Source: National Institute on Drug Abuse (NIDA) Methamphetamine Use and Risk for HIV/AIDS, Centers for Disease Control (CDC) HIV/AIDS Fact Sheet www.cdc.gov/hiv/resources/factsheets/meth.htm Technical Support Document: Toxicology/Clandestine Drug Labs: Methamphetamine, California Office of Environmental Health Hazard Assessment, Volume 1, Number 8 http://oehha.ca.gov/public_info/pdf/TSD%20Methamphetamine%20Meth%20La bs%2010'8'03.pdf Basic Facts about Methamphetamine Methamphetamine is an addictive stimulant drug that strongly activates certain systems in the brain. Methamphetamine is closely related chemically to amphetamine, but the central nervous system effects of methamphetamine are greater. -

The Neurocircuitry of Illicit Psychostimulant Addiction: Acute and Chronic Effects in Humans
Substance Abuse and Rehabilitation Dovepress open access to scientific and medical research Open Access Full Text Article R E V IEW The neurocircuitry of illicit psychostimulant addiction: acute and chronic effects in humans Sara B Taylor1 Abstract: Illicit psychostimulant addiction remains a significant problem worldwide, despite Candace R Lewis1 decades of research into the neural underpinnings and various treatment approaches. The purpose M Foster Olive1,2 of this review is to provide a succinct overview of the neurocircuitry involved in drug addiction, as well as the acute and chronic effects of cocaine and amphetamines within this circuitry in 1Program in Behavioral Neuroscience, 2Interdisciplinary Graduate Program humans. Investigational pharmacological treatments for illicit psychostimulant addiction are in Neuroscience, Arizona State also reviewed. Our current knowledge base clearly demonstrates that illicit psychostimulants University, Tempe, AZ, USA produce lasting adaptive neural and behavioral changes that contribute to the progression and maintenance of addiction. However, attempts at generating pharmacological treatments for psychostimulant addiction have historically focused on intervening at the level of the acute effects of these drugs. The lack of approved pharmacological treatments for psychostimulant addiction highlights the need for new treatment strategies, especially those that prevent or ameliorate the adaptive neural, cognitive, and behavioral changes caused by chronic use of this class of illicit drugs. Keywords: -

CPDD 77Th Annual Meeting • Arizona Biltmore, Phoenix, Arizona
CPDD 77th Annual Meeting • Arizona Biltmore, Phoenix, Arizona 1 2 EFFECT OF HEMISPHERIC DOMINANT VERSUS NON- SEX, DRUGS, AND VIOLENCE: AN ANALYSIS OF WOMEN IN DOMINANT INSULAR DAMAGE ON SMOKING BEHAVIORS. DRUG COURT. Amir Abdolahi1,2, Geoffrey Williams2, Curtis Benesch2, Henry Wang2, Eric Abenaa Acheampong2, Catherine W Striley3, David O Fakunle1, Linda Cottler3; Spitzer3, Bryan Scott3, Robert Block2, Edwin van Wijngaarden2; 1Philips 1Mental Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Research, Briarcliff Manor, NY, 2University of Rochester, Rochester, NY, MD, 2University of Florida, Gainesville, FL, 3Epidemiology, University of 3Rochester General Health System, Rochester, NY Florida, Gainesville, FL Aims: Recent evidence suggests that damage to the insular cortex (IC), the cere- Aims: This analysis examines exposure to violence and substance use disorders bral cortex beneath the sylvian fissure, disrupts nicotine-induced cravings and is among women in drug court who are: current sex traders (CST), former sex associated with a greater likelihood of cessation relative to non-IC damage. The traders (FST), or women who have never traded sex. role hemispheric dominance may play in regulating these changes, however, has Methods: Data comes from 319 women recruited from a Municipal Drug Court not yet been explored. We hypothesized that current smokers with damage to System in the Midwest. Women were interviewed about sex trading, violence, their dominant IC would experience less withdrawal and cravings and be more and drug use. Women who traded sex in the past 4 months for drugs, alcohol, likely to quit than those with non-dominant IC damage. or other resources were classified as CST, while women who previously traded Methods: A total of 37 smokers with unilateral IC strokes (17 dominant and 20 sex but not in the past 4 months were classified as FST. -

The Effects of Stimulant Medication on the Social Behavior of Children with ADHD During Times of Play Robert, Jr
Louisiana State University LSU Digital Commons LSU Doctoral Dissertations Graduate School 2002 The effects of stimulant medication on the social behavior of children with ADHD during times of play Robert, Jr. H. LaRue Louisiana State University and Agricultural and Mechanical College, [email protected] Follow this and additional works at: https://digitalcommons.lsu.edu/gradschool_dissertations Part of the Psychology Commons Recommended Citation LaRue, Robert, Jr. H., "The effects of stimulant medication on the social behavior of children with ADHD during times of play" (2002). LSU Doctoral Dissertations. 2403. https://digitalcommons.lsu.edu/gradschool_dissertations/2403 This Dissertation is brought to you for free and open access by the Graduate School at LSU Digital Commons. It has been accepted for inclusion in LSU Doctoral Dissertations by an authorized graduate school editor of LSU Digital Commons. For more information, please [email protected]. THE EFFECTS OF STIMULANT MEDICATION ON THE SOCIAL BEHAVIOR OF CHILDREN WITH ADHD DURING TIMES OF PLAY A Dissertation Submitted to the Graduate Faculty of the Louisiana State University and Agricultural and Mechanical College In partial fulfillment of the Requirements for the degree of Doctor of Philosophy in The Department of Psychology by Robert H. LaRue Jr. B.A., Rutgers University, 1995 M.A., Louisiana State University, 2000 December 2002 TABLE OF CONTENTS LIST OF TABLES . iv ABSTRACT . v CHAPTER 1 INTRODUCTION . 1 Overview of the Literature. 1 The Developmental Significance of Play. 6 The Effects of Stimulants on Play and Related Social Behavior - Basic Research. 8 The Effects of Stimulants on Related Social Behavior in Rats and Non-Human Primates. -

Australian Product Information Neupro® (Rotigotine) Transdermal Patches
AUSTRALIAN PRODUCT INFORMATION NEUPRO® (ROTIGOTINE) TRANSDERMAL PATCHES 1 NAME OF THE MEDICINE Rotigotine 2 QUALITATIVE AND QUANTITATIVE COMPOSITION Neupro 1 mg: 5 cm2 patch containing 2.25 mg rotigotine with a nominal release rate of 1 mg rotigotine per 24 hours. Neupro 2 mg: 10 cm2 patch containing 4.5 mg rotigotine with a nominal release rate of 2 mg rotigotine per 24 hours. Neupro 3 mg: 15 cm2 patch containing 6.75 mg rotigotine with a nominal release rate of 3 mg rotigotine per 24 hours. Neupro 4 mg: 20 cm2 patch containing 9.0 mg rotigotine with a nominal release rate of 4 mg rotigotine per 24 hours. Neupro 6 mg: 30 cm2 patch containing 13.5 mg rotigotine with a nominal release rate of 6 mg rotigotine per 24 hours. Neupro 8 mg: 40 cm2 patch containing 18.0 mg rotigotine with a nominal release rate of 8 mg rotigotine per 24 hours. The active ingredient rotigotine is a white to light brownish powder. It is very slightly soluble to freely soluble in organic solvents, sparingly soluble in acidic aqueous solutions and practically insoluble in alkaline aqueous solutions. The formulation contains sodium metabisulfite. For the full list of excipients, see Section 6.1 List of Excipients. 3 PHARMACEUTICAL FORM Neupro is a thin, matrix-type transdermal patch composed of 3 layers: 1. A flexible, tan-colored backfilm that provides structural support and protection of the drug loaded adhesive layer. 2. A self-adhesive drug matrix layer. 3. A clear protective liner which is removed prior to use. -

Neupro, INN-Rotigotine
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 1. NAME OF THE MEDICINAL PRODUCT Neupro 1 mg/24 h transdermal patch Neupro 3 mg/24 h transdermal patch 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Neupro 1 mg/24 h transdermal patch Each patch releases 1 mg of rotigotine per 24 hours. Each patch of 5 cm2 contains 2.25 mg of rotigotine. Neupro 3 mg/24 h transdermal patch Each patch releases 3 mg of rotigotine per 24 hours. Each patch of 15 cm2 contains 6.75 mg of rotigotine. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Transdermal patch. Thin, matrix-type, square-shaped with rounded edges, consisting of three layers. Neupro 1 mg/24 h transdermal patch The outside of the backing layer is tan-coloured and imprinted with ‘Neupro 1 mg/24 h’. Neupro 3 mg/24 h transdermal patch The outside of the backing layer is tan-coloured and imprinted with ‘Neupro 3 mg/24 h’. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Neupro is indicated for the symptomatic treatment of moderate to severe idiopathic Restless Legs Syndrome (RLS) in adults. 4.2 Posology and method of administration Posology The dose recommendations made are in nominal dose. A single daily dose should be initiated at 1 mg/24 h. Depending on the individual patient response, the dose may be increased in weekly increments of 1 mg/24 h to a maximum dose of 3 mg/24 h. The need for treatment continuation should be reconsidered every 6 months. Neupro is applied once a day. -

Pramipexole in Psychiatry: a Systematic Review of the Literature
Systematic Review of Pramipexole in Psychiatry Pramipexole in Psychiatry: A Systematic Review of the Literature Chris B. Aiken, M.D. ramipexole, a dopamine agonist approved for the Ptreatment of Parkinson’s disease and restless legs syndrome, has unique properties that offer therapeutic Objective: To assess the risks and benefits potential in psychiatry. It possesses both dopaminergic of pramipexole in psychiatric populations. and neuroprotective effects, making it a promising candi- Data Sources: A PubMed search was date for bipolar depression. Recent clinical studies have performed using the keywords pramipexole 1 and ropinirole, which identified 500 articles. earned it a place as a stage-5 treatment in the Texas and 2 Study Selection: All clinical studies in psychi- Canadian algorithms for bipolar I depression. Concur- atric populations were included in the primary rently, case reports from Parkinson’s disease clinics have review (24 articles). Studies involving other raised concerns about the potential for compulsive behav- populations were then reviewed to evaluate iors and sudden sleep attacks to arise during treatment potential risks and benefits not identified in the psychiatric studies. with the drug. To investigate these promises and perils, Data Extraction: Effect sizes were calculated the neurologic and psychiatric studies of pramipexole from controlled studies. Rates of intolerable side were systematically reviewed. effects and manic switching were estimated by pooled analysis of controlled and uncontrolled studies. METHOD Data Synthesis: Pramipexole has a large effect size (0.6–1.1) in the treatment of both bipolar and A PubMed literature search was performed using the unipolar depression with a low short-term rate of keywords pramipexole and ropinirole. -
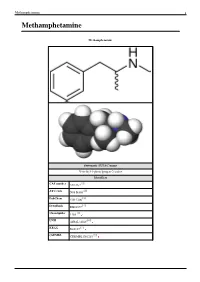
Methamphetamine 1 Methamphetamine
Methamphetamine 1 Methamphetamine Methamphetamine Systematic (IUPAC) name N-methyl-1-phenylpropan-2-amine Identifiers [1] CAS number 537-46-2 [2] ATC code N06 BA03 [3] PubChem CID 1206 [4] DrugBank DB01577 [5] ChemSpider 1169 [6] UNII 44RAL3456C [7] KEGG D08187 [8] ChEMBL CHEMBL1201201 Methamphetamine 2 Synonyms Desoxyephedrine Pervitin Anadrex Methedrine Methylamphetamine Syndrox Desoxyn Chemical data Formula C H N 10 15 Mol. mass 149.233 g/mol [9] [10] SMILES eMolecules & PubChem Pharmacokinetic data Bioavailability 62.7% oral; 79% nasal; 90.3% smoked; 99% rectally; 100% IV Metabolism Hepatic [11] Half-life 9–12 hours Excretion Renal Therapeutic considerations Pregnancy cat. C(US) Legal status Controlled (S8) (AU) Schedule I (CA) Schedule II (US) Class A(NZ) Schedule 5(SA) Injectable:Class A, Oral: A(UK) Routes Medical: Oral Recreational: Oral, I.V., I.M., Insufflation, Inhalation, Rectal [12] (what is this?) (verify) [13] Methamphetamine (pronounced /ˌmɛθæmˈfɛtəmiːn/ listen ), also known as metamfetamine (INN for the (+) form), methylamphetamine, N-methylamphetamine, desoxyephedrine, and colloquially as "meth" or "crystal meth", is a psychostimulant of the phenethylamine and amphetamine class of drugs. It increases alertness, concentration, energy, and in high doses, can induce euphoria, enhance self-esteem, and increase libido.[14] [15] Methamphetamine has high potential for abuse and addiction by activating the psychological reward system via triggering a cascading release of dopamine, norepinephrine and serotonin in the brain. Methamphetamine is FDA approved for the treatment of ADHD and exogenous obesity, marketed in the USA under the trademark name Desoxyn.[16] Methamphetamine is illicitly synthesized and then sold in a crystalline form resembling small shards of odorless, bitter-tasting crystals; leading to the colloquial nickname "crystal meth". -

Monday Scientific Session Listing:261–437
MONDAY SCIENTIFIC SESSION LISTING:261–437 Washington, DC Nov. 11–15 Complete Session Listing Monday AM LECTURE Walter E. Washington Convention Center SYMPOSIUM Walter E. Washington Convention Center 261. Neural Circuits Controlling the Selection and 263. ● Assembly and Maintenance of the Peripheral Nerve Persistence of Sensory Information — CME Node of Ranvier in Development, Health, and Disease — CME Mon. 8:30 AM - 9:40 AM — Hall D Speaker: T. MOORE, Stanford Univ. and Howard Hughes Mon. 8:30 AM - 11:00 AM — 146A Med. Inst. Chair: H. J. WILLISON The processing and retention of sensory input is influenced Co-Chair: P. J. BROPHY by a number of endogenous factors, such as arousal, Nodes of Ranvier are the sites of saltatory conduction, motivation, and cognitive control. These factors appear to a fundamental adaption of myelinated axons. Our constrain the sensory information guiding adaptive behavior. understanding of the molecular organization of the nodal AM Mon. This lecture will discuss recent evidence on the neural region has rapidly advanced. Many components have been circuits involved in the modulation, filtering, and persistence identified, as have the interactions among the axonal and of sensory information and their relation to basic cognitive glial molecules, accounting for the specialized features of functions such as attention and working memory. The lecture nodal, paranodal, and juxtaparanodal domains. Human will include evidence from a range of model systems and autoimmune neuropathies are diseases that target glial approaches, as well as a discussion on the relevance to and axonal nodal proteins and glycolipids, leading to mental disorders. nodal disruption and conduction block. -

Breaking the Ice: Inquiry Into 'Ice' Use in the Northern Territory
LEGISLATIVE ASSEMBLY OF THE NORTHERN TERRITORY ‘Ice’ Select Committee Breaking the Ice Inquiry into ‘ice’ use in the Northern Territory November 2015 National Library of Australia Cataloguing-in-Publication Data Author: ‘Ice’ Select Committee Title: Breaking the Ice: inquiry into ‘ice’ use in the Northern Territory ISBN: 9780992589141 (paperback) Subjects: Ice (Drug)—Northern Territory. Drug abuse—Northern Territory. Other Authors/Contributors: Northern Territory. Legislative Assembly. ‘Ice’ Select Committee. Dewey Decimal Classification Notation: 362.299099429 Contents Contents Committee Members ................................................................................................................5 Committee Secretariat .............................................................................................................6 Acknowledgments ....................................................................................................................6 Acronyms and Abbreviations .................................................................................................7 Terms of Reference ..................................................................................................................9 Executive Summary .............................................................................................................. 10 Recommendations ................................................................................................................ 13 1 Introduction ...................................................................................................... -

Methamphetamine and Violence in Illinois
METHAMPHETAMINE AND VIOLENCE IN ILLINOIS Final Report Submitted To Illinois Criminal Justice Information Authority 300 West Adams, Suite 700 Chicago, Illinois 60606 Investigator Initiated Research by Dr. Ralph A. Weisheit, Distinguished Professor Department of Criminal Justice Sciences Illinois State University Normal, Illinois 61790-5250 Phone: 309-438-3849 Fax: 309-438-7289 e-mail: [email protected] Table of Contents I. Executive Summary .…………………………………………………………… 3 II. Review of the Relevant Literature ……………………………………………... 7 A. A Brief History of Amphetamine and Methamphetamine ……………... 8 B. Physiological Effects of Amphetamine …………………………………10 C. Current Trends in Methamphetamine ………………………………….. 14 D. Methamphetamine in Rural Areas …………………………………….. 16 E. Methamphetamine Production in the Midwest ……………………….. 18 F. Methamphetamine and Violence ………………………………………. 20 III. Research Design ……………………………………………………………….. 22 A. Locating and Interviewing Subjects …………………………………… 24 IV. Findings of the Study ………………………………………………………….. 27 A. Psychopharmacological Violence: Violence from Methamphetamine’s Effects on the User ……………… 29 B. Systemic Violence: Violence and the Business of Methamphetamine ……………………... 36 C. Economic Compulsive Violence: Violence to Obtain Money to Buy Drugs...……………………………..39 D. Violence and the Drug Subculture …………………………………….. 40 V. Addressing Limitations of the Method ………………………………………... 48 VI. Implications for Policy and Practice ………………………………………….. 48 VII. References …………………………………………………………………….. 54 VII. Appendix A …………………………………………………………………... 64 VIII. Appendix B ………………………………………………………………….. 76 This project was supported by Grant #04-DB-BX-0043, awarded by the Bureau of Justice Assistance, Office of Justice Programs, U.S. Department of Justice, through the Illinois Criminal Justice Information Authority. Points of view or opinions contained within this document are those of the authors and do not necessarily represent the official position or policies of the U.S. Department of Justice, or the Illinois Criminal Justice Information Authority.