Evidence from the P3 Wave and the Lateralized Readiness Potential
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

UC San Diego UC San Diego Electronic Theses and Dissertations
UC San Diego UC San Diego Electronic Theses and Dissertations Title Neurophysiologic correlates to sensory and cognitive processing in altered states of consciousness Permalink https://escholarship.org/uc/item/3gv8j4jk Author Cahn, Baruch Rael Publication Date 2007 Peer reviewed|Thesis/dissertation eScholarship.org Powered by the California Digital Library University of California i UNIVERSITY OF CALIFORNIA, SAN DIEGO Neurophysiologic Correlates to Sensory and Cognitive Processing in Altered States of Consciousness A Dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Neurosciences by Baruch Rael Cahn Committee in charge: Mark Geyer, Chair John Polich, Co-Chair Steve Hillyard Martin Paulus Jaime Pineda Vilayanur Ramachandran Franz Vollenweider 2007 ii Copyright Baruch Rael Cahn, 2007 All Rights Reserved iii The Dissertation of Baruch Rael Cahn is approved, and it is acceptable in quality and form for publication on microfilm: _______________ _______________ _______________ _______________ _______________ _______________ Co-Chair _______________ Chair University of California, San Diego 2007 iii iv DEDICATION I dedicate this thesis in loving memory to my sister Lotus Blossom Cahn who passed away in 2005 from cancer of the thymus. May the love she brought to all those whose lives she touched live on through us and reach out to the world we inhabit. iv v TABLE OF CONTENTS Signature Page ………………………………………………………………..………. iii Dedication ……………….……………………………………………………………. iv Table of Contents ……………………………………………………………..……… -

The Deficit of Multimodal Perception of Congruent and Non-Congruent Fearful Expressions in Patients with Schizophrenia: the ERP Study
brain sciences Article The Deficit of Multimodal Perception of Congruent and Non-Congruent Fearful Expressions in Patients with Schizophrenia: The ERP Study Galina V. Portnova 1,2,*, Aleksandra V. Maslennikova 1,3, Natalya V. Zakharova 3 and Olga V. Martynova 1,4 1 Institute of Higher Nervous Activity and Neurophysiology of RAS, 117485 Moscow, Russia; [email protected] (A.V.M.); [email protected] (O.V.M.) 2 The Pushkin State Russian Language Institute, 117485 Moscow, Russia 3 Psychiatric Clinical Hospital No. 1 Named after ON. Alekseeva of the Moscow City Health Department, 117152 Moscow, Russia; [email protected] 4 Centre for Cognition and Decision Making, Institute for Cognitive Neuroscience, National Research University Higher School of Economics, 109548 Moscow, Russia * Correspondence: [email protected] Abstract: Emotional dysfunction, including flat affect and emotional perception deficits, is a specific symptom of schizophrenia disorder. We used a modified multimodal odd-ball paradigm with fearful facial expressions accompanied by congruent and non-congruent emotional vocalizations (sounds of women screaming and laughing) to investigate the impairment of emotional perception and reactions to other people’s emotions in schizophrenia. We compared subjective ratings of emotional state and event-related potentials (EPPs) in response to congruent and non-congruent stimuli in patients with schizophrenia and healthy controls. The results showed the altered multimodal perception of fearful stimuli in patients with schizophrenia. The amplitude of N50 was significantly higher for non-congruent stimuli than congruent ones in the control group and did not differ in patients. The Citation: Portnova, G.V.; P100 and N200 amplitudes were higher in response to non-congruent stimuli in patients than in Maslennikova, A.V.; Zakharova, N.V.; controls, implying impaired sensory gating in schizophrenia. -

A Critical Review of the Deviance Detection Theory of Mismatch Negativity
Review A Critical Review of the Deviance Detection Theory of Mismatch Negativity Jamie A. O’Reilly 1,* and Amonrat O’Reilly 2 1 College of Biomedical Engineering, Rangsit University, Pathumthani 12000, Thailand 2 Thailand Institute for Science and Technological Research, Pathumthani 12120, Thailand; [email protected] * Correspondence: [email protected] Abstract: Mismatch negativity (MMN) is a component of the difference waveform derived from passive auditory oddball stimulation. Since its inception in 1978, this has become one of the most popular event-related potential techniques, with over two-thousand published studies using this method. This is a testament to the ingenuity and commitment of generations of researchers engaging in basic, clinical and animal research. Despite this intensive effort, high-level descriptions of the mechanisms theorized to underpin mismatch negativity have scarcely changed over the past four decades. The prevailing deviance detection theory posits that MMN reflects inattentive detection of difference between repetitive standard and infrequent deviant stimuli due to a mismatch between the unexpected deviant and a memory representation of the standard. Evidence for these mechanisms is inconclusive, and a plausible alternative sensory processing theory considers fundamental principles of sensory neurophysiology to be the primary source of differences between standard and deviant responses evoked during passive oddball stimulation. By frequently being restated without appropri- ate methods to exclude alternatives, the potentially flawed deviance detection theory has remained largely dominant, which could lead some researchers and clinicians to assume its veracity implicitly. Citation: O’Reilly, J.A.; O’Reilly, A. It is important to have a more comprehensive understanding of the source(s) of MMN generation A Critical Review of the Deviance before its widespread application as a clinical biomarker. -

Integration of EEG-FMRI in an Auditory Oddball Paradigm Using Joint Independent Component Analysis Jain Mangalathu Arumana Marquette University
Marquette University e-Publications@Marquette Dissertations (2009 -) Dissertations, Theses, and Professional Projects Integration of EEG-FMRI in an Auditory Oddball Paradigm Using Joint Independent Component Analysis Jain Mangalathu Arumana Marquette University Recommended Citation Mangalathu Arumana, Jain, "Integration of EEG-FMRI in an Auditory Oddball Paradigm Using Joint Independent Component Analysis" (2012). Dissertations (2009 -). Paper 210. http://epublications.marquette.edu/dissertations_mu/210 INTEGRATION OF EEG-FMRI IN AN AUDITORY ODDBALL PARADIGM USING JOINT INDEPENDENT COMPONENT ANALYSIS by Jain Mangalathu Arumana, B.Sc., M.Sc. A dissertation submitted to the Faculty of the Graduate School, Marquette University, in Partial Fulfillment of the Requirements for the Degree of Doctor Philosophy Milwaukee, Wisconsin August 2012 ABSTRACT INTEGRATION OF EEG-FMRI IN AN AUDITORY ODDBALL PARADIGM USING JOINT INDEPENDENT COMPONENT ANALYSIS Jain Mangalathu Arumana, B.Sc., M.Sc. Marquette University, 2012 The integration of event-related potential (ERP) and functional magnetic resonance imaging (fMRI) can contribute to characterizing neural networks with high temporal and spatial resolution. The overall objective of this dissertation is to determine the sensitivity and limitations of joint independent component analysis (jICA) within- subject for integration of ERP and fMRI data collected simultaneously in a parametric auditory oddball paradigm. The main experimental finding in this work is that jICA revealed significantly stronger and more extensive activity in brain regions associated with the auditory P300 ERP than a P300 linear regression analysis, both at the group level and within-subject. The results suggest that, with the incorporation of spatial and temporal information from both imaging modalities, jICA is more sensitive to neural sources commonly observed with ERP and fMRI compared to a linear regression analysis. -

Auditory P3a and P3b Neural Generators in Schizophrenia: an Adaptive Sloreta P300 Localization Approach
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by UPCommons. Portal del coneixement obert de la UPC This is an author-edited version of the accepted manuscript published in Schizophrenia Research. The final publication is available at Elsevier via http://dx.doi.org/10.1016/j.schres.2015.09.028 Auditory P3a and P3b neural generators in schizophrenia: An adaptive sLORETA P300 localization approach Alejandro Bachiller1, Sergio Romero2,3, Vicente Molina4,5, Joan F. Alonso2,3, Miguel A. Mañanas2,3, Jesús Poza1,5,6 and Roberto Hornero1,6 1 Biomedical Engineering Group, E.T.S. Ingenieros de Telecomunicación, Universidad de Valladolid, 47011 Valladolid, Spain. {[email protected]; [email protected]; [email protected]} 2 Department of Automatic Control (ESAII), Biomedical Engineering Research Center (CREB), Universitat Politècnica de Catalunya (UPC), 08028 Barcelona, Spain. {[email protected]; [email protected]; [email protected]} 3 CIBER de Bioingeniería, Biomateriales y Nanomedicina (CIBER-BBN) 4 Psychiatry Department, Hospital Clínico Universitario, Facultad de Medicina, Universidad de Valladolid, 47005 Valladolid, Spain {[email protected]} 5 INCYL, Instituto de Neurociencias de Castilla y León, Universidad de Salamanca, 37007 Salamanca, Spain 6 IMUVA, Instituto de Investigación en Matemáticas, Universidad de Valladolid, 47011 Valladolid, Spain Corresponding author. Alejandro Bachiller, Biomedical Engineering Group, E.T.S. Ingenieros de Telecomunicación, Universidad de Valladolid, 47011 Valladolid, Spain Tel: +34 983423000 ext. 5589; fax: +34 983423667; Email address: [email protected] Abstract The present study investigates the neural substrates underlying cognitive processing in schizophrenia (Sz) patients. -

ERP Peaks Review 1 LINKING BRAINWAVES to the BRAIN
ERP Peaks Review 1 LINKING BRAINWAVES TO THE BRAIN: AN ERP PRIMER Alexandra P. Fonaryova Key, Guy O. Dove, and Mandy J. Maguire Psychological and Brain Sciences University of Louisville Louisville, Kentucky Short title: ERPs Peak Review. Key Words: ERP, peak, latency, brain activity source, electrophysiology. Please address all correspondence to: Alexandra P. Fonaryova Key, Ph.D. Department of Psychological and Brain Sciences 317 Life Sciences, University of Louisville Louisville, KY 40292-0001. [email protected] ERP Peaks Review 2 Linking Brainwaves To The Brain: An ERP Primer Alexandra Fonaryova Key, Guy O. Dove, and Mandy J. Maguire Abstract This paper reviews literature on the characteristics and possible interpretations of the event- related potential (ERP) peaks commonly identified in research. The description of each peak includes typical latencies, cortical distributions, and possible brain sources of observed activity as well as the evoking paradigms and underlying psychological processes. The review is intended to serve as a tutorial for general readers interested in neuropsychological research and a references source for researchers using ERP techniques. ERP Peaks Review 3 Linking Brainwaves To The Brain: An ERP Primer Alexandra P. Fonaryova Key, Guy O. Dove, and Mandy J. Maguire Over the latter portion of the past century recordings of brain electrical activity such as the continuous electroencephalogram (EEG) and the stimulus-relevant event-related potentials (ERPs) became frequent tools of choice for investigating the brain’s role in the cognitive processing in different populations. These electrophysiological recording techniques are generally non-invasive, relatively inexpensive, and do not require participants to provide a motor or verbal response. -

Reconfiguration of Brain Network Between Resting-State and Oddball Paradigm
Reconfiguration of Brain Network between Resting-state and Oddball Paradigm Fali Li1, Chanlin Yi1, Yuanyuan Liao1, Yuanling Jiang1, Yajing Si1, Limeng Song1, Tao Zhang1, Dezhong Yao1,2, Yangsong Zhang1,2, 3, Zehong Cao4 and Peng Xu1,2 1The Clinical Hospital of Chengdu Brain Science Institute, MOE Key Lab for NeuroInformation, University of Electronic Science and Technology of China, Chengdu, 611731, China 2School of Life Science and Technology, Center for Information in Medicine, University of Electronic Science and Technology of China, Chengdu, 611731, China 3School of Computer Science and Technology, Southwest University of Science and Technology, Mianyang, 621010, China 4Centre for Artificial Intelligence, Faculty of Engineering and IT, University of Technology Sydney, NSW, Australia Corresponding author: Yangsong Zhang ([email protected]), Peng Xu ([email protected]). This work was supported by the National Key Research and Development Plan of China (#2017YFB1002501), the National Natural Science Foundation of China (#61522105, #61603344, #81401484, and #81330032), the Open Foundation of Henan Key Laboratory of Brain Science and Brain-Computer Interface Technology (No. HNBBL17001), and the Longshan academic talent research supporting program of SWUST (#17LZX692). ABSTRACT The oddball paradigm is widely applied to the investigation of multiple cognitive functions. Prior studies have explored the cortical oscillation and power spectral differing from the resting-state conduction to oddball paradigm, but whether brain networks -

P50 Potential-Associated Gamma Band Activity: Modulation by Distraction
Short communication Acta Neurobiol Exp 2012, 72: 102–109 P50 potential-associated gamma band activity: Modulation by distraction Inga Griskova-Bulanova1, 2 *, Osvaldas Ruksenas3, Kastytis Dapsys1, 3, Valentinas Maciulis1, and Sidse M. Arnfred4 1Department of Electrophysiological Treatment and Investigation Methods, Vilnius Republican Psychiatric Hospital, Vilnius, Lithuania, *Email: [email protected]; 2Department of Psychology, Mykolas Romeris University, Vilnius, Lithuania; 3Department of Biochemistry-Biophysics, Vilnius University, Vilnius, Lithuania; 4Psychiatric Center Ballerup, University Hospital of Copenhagen, Copenhagen, Denmark We aimed to evaluate the effect of changing attentional demands towards stimulation in healthy subjects on P50 potential- related high-frequency beta and gamma oscillatory responses, P50 and N100 peak amplitudes and their gating measures. There are no data showing effect of attention on P50 potential-related beta and gamma oscillatory responses and previous results of attention effects on P50 and N100 amplitudes and gating measures are inconclusive. Nevertheless the variation in the level of attention may be a source of variance in the recordings as well as it may provide additional information about the pathology under study. Nine healthy volunteers participated in the study. A standard paired stimuli auditory P50 potential paradigm was applied. Four stimulation conditions were selected: focused attention (stimuli pair counting), unfocused attention (sitting with open eyes), easy distraction (reading a magazine article), and difficult distraction (searching for Landolt rings with appropriate gap orientation). Time-frequency responses to both S1 and S2 were evaluated in slow beta (13–16 Hz, 45–175 ms window); fast beta (20–30 Hz, 45–105 ms window) and gamma (32–46 Hz, 45–65 ms window) ranges. -

Impaired P50 Sensory Gating in Machado-Joseph Disease
Clinical Neurophysiology 115 (2004) 2231–2235 www.elsevier.com/locate/clinph Impaired P50 sensory gating in Machado-Joseph disease Eduardo S. Ghisolfia,c,d,*, Gustavo H.B. Maegawae, Jefferson Beckerf,g, Ana Paula Zanardoa, Ivo M. Strimitzer Jr.a, Alexandre S. Prokopiuka, Maria Luiza Pereiraa,e, Thiago Carvalhoa, Laura B. Jardimb,e, Diogo R. Larad aDepartamento de Bioquı´mica da Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil bDepartamento de Medicina Interna da Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil cDepartamento de Cieˆncia da Sau´de da Universidade Regional Integrada do Alto Uruguai e das Misso˜es, campus de Frederico Westphalen, Frederico Westphalen, Brazil dDepartamento de Cieˆncias Fisiolo´gicas, Faculdade de Biocieˆncias, Pontifı´cia Universidade Cato´lica do Rio Grande do Sul (PUCRS), Av. Ipiranga, 6681, Pre´dio 12A, Caixa Postal 1429, 90619-900 Porto Alegre, RS, Brazil eServic¸o de Gene´tica Me´dica do Hospital de Clı´nicas de Porto Alegre, Porto Alegre, Brazil fServic¸o de Neurologia do Hospital de Clı´nicas de Porto Alegre, Porto Alegre, Brazil gUnidade de Neurofisiologia da Universidade Luterana do Brasil, Canoas, Brazil Accepted 25 April 2004 Available online 25 June 2004 Abstract Objective: Machado-Joseph disease (MJD), an autosomal dominant spinocerebellar degeneration caused by an expanded CAG repeat on chromosome 14q32.1, is a disorder with wide range of neurological findings and brain regions involved. Studies evaluating neurophysiological parameters related to sensory gating in MJD are lacking. Methods: This study intends to investigate P50 suppression, an auditory mid-latency evoked potential in a test-conditioning paradigm, considered as an index of sensory gating function. -

Validating a Novel Oddball Paradigm in Virtual Reality
bioRxiv preprint doi: https://doi.org/10.1101/749192; this version posted March 23, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. Running head: NOVEL ODDBALL PARADIGM IN VIRTUAL REALITY Real brains in virtual worlds: Validating a novel oddball paradigm in virtual reality Jonathan W. P. Kuziek a, Abdel R. Tayema, Jennifer I. Burrella, Eden X. Redman a, Jeff Murrayc, Jenna Reinenc, Aldis Sipolinsc, Kyle E. Mathewsona,b a Department of Psychology, Faculty of Science, University of Alberta, b Neuroscience and Mental Health Institute, Faculty of Medicine and Dentistry, University of Alberta c IBM Research: Education & Cognitive Sciences Type of article: Full length research paper Number of text pages: 30 (including references) Number of figures: 7 Number of tables: 5 Corresponding Author: Kyle E. Mathewson, Ph.D. Assistant Professor of Cognitive Neuroscience Department of Psychology P-455 Biological Sciences University of Alberta Edmonton, AB, Canada, T6G 2E9 [email protected] bioRxiv preprint doi: https://doi.org/10.1101/749192; this version posted March 23, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder. All rights reserved. No reuse allowed without permission. NOVEL ODDBALL PARADIGM IN VIRTUAL REALITY 1 1 Electroencephalography (EEG) research is typically conducted in controlled laboratory settings. This 2 limits the generalizability to real-world situations. Virtual reality (VR) sits as a transitional tool that 3 provides tight experimental control with more realistic stimuli. To test the validity of using VR for event- 4 related potential (ERP) research we used a well-established paradigm, the oddball task. -
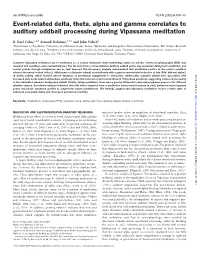
Event-Related Delta, Theta, Alpha and Gamma Correlates to Auditory Oddball Processing During Vipassana Meditation
doi:10.1093/scan/nss060 SCAN (2013) 8,100^111 Event-related delta, theta, alpha and gamma correlates to auditory oddball processing during Vipassana meditation B. Rael Cahn,1,2,3 Arnaud Delorme,3,4,5 and John Polich2 1Department of Psychiatry, University of California, Irvine, Irvine, 2Molecular and Integrative Neurosciences Department, The Scripps Research Institute, La Jolla, CA,USA, 3Meditation Research Institute, Rishikesh, Uttarakhand, India, 4Institute of Neural Computation, University of California, San Diego, La Jolla, CA, USA 5CERCO, CNRS, Universite´ Paul Sabatier, Toulouse, France Long-term Vipassana meditators sat in meditation vs. a control (instructed mind wandering) states for 25 min, electroencephalography (EEG) was recorded and condition order counterbalanced. For the last 4 min, a three-stimulus auditory oddball series was presented during both meditation and control periods through headphones and no task imposed. Time-frequency analysis demonstrated that meditation relative to the control condition evinced decreased evoked delta (2–4 Hz) power to distracter stimuli concomitantly with a greater event-related reduction of late (500–900 ms) alpha-1 (8–10 Hz) activity, which indexed altered dynamics of attentional engagement to distracters. Additionally, standard stimuli were associated with Downloaded from increased early event-related alpha phase synchrony (inter-trial coherence) and evoked theta (4–8 Hz) phase synchrony, suggesting enhanced processing of the habituated standard background stimuli. Finally, during meditation, there was a greater differential early-evoked gamma power to the different stimulus classes. Correlation analysis indicated that this effect stemmed from a meditation state-related increase in early distracter-evoked gamma power and phase synchrony specific to longer-term expert practitioners. -

Auditory P300 and N100 Components As Intermediate Phenotypes for Psychotic Disorder: Familial Liability and Reliability ⇑ Claudia J.P
Clinical Neurophysiology 122 (2011) 1984–1990 Contents lists available at ScienceDirect Clinical Neurophysiology journal homepage: www.elsevier.com/locate/clinph Auditory P300 and N100 components as intermediate phenotypes for psychotic disorder: Familial liability and reliability ⇑ Claudia J.P. Simons a,b, , Anke Sambeth c, Lydia Krabbendam a,e, Stefanie Pfeifer a, Jim van Os a,d, Wim J. Riedel c a Department of Psychiatry and Neuropsychology, Maastricht University, European Graduate School of Neuroscience, SEARCH, P.O. Box 616, 6200 MD Maastricht, The Netherlands b GGzE, Institute of Mental Health Care Eindhoven en de Kempen, P.O. Box 909, 5600 AX Eindhoven, The Netherlands c Department of Neuropsychology and Psychopharmacology, Faculty of Psychology and Neuroscience, Maastricht University, P.O. Box 616, 6200 MD Maastricht, The Netherlands d Visiting Professor of Psychiatric Epidemiology, King’s College London, King’s Health Partners, Department of Psychosis Studies, Institute of Psychiatry, UK e Centre Brain and Learning, Department of Psychology and Education, VU University Amsterdam, van der Boechorststraat 1, 1081 BT Amsterdam, The Netherlands article info highlights Article history: A reliable N100 latency delay was found in unaffected siblings of patients with a psychotic disorder. Accepted 28 February 2011 P300 amplitude and latency were not found to be affected in siblings. Available online 1 April 2011 Short-term test–retest reliability of N100 and P300 components were sound across patients, siblings and controls, with the main exception of N100 latency in patients. Keywords: Electroencephalography Event-related potentials abstract Psychoses Schizophrenia Objective: Abnormalities of the auditory P300 are a robust finding in patients with psychosis. The pur- Test–retest poses of this study were to determine whether patients with a psychotic disorder and their unaffected Relatives siblings show abnormalities in P300 and N100 and to establish test–retest reliabilities for these ERP com- ponents.