Scapula, Shoulder,& Humerus
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Body Mechanics As the Rotator Cuff Gether in a Cuff-Shape Across the Greater and Lesser Tubercles the on Head of the Humerus
EXPerT CONTENT Body Mechanics by Joseph E. Muscolino | Artwork Giovanni Rimasti | Photography Yanik Chauvin Rotator Cuff Injury www.amtamassage.org/mtj WORKING WITH CLieNTS AFFecTED BY THIS COmmON CONDITION ROTATOR CUFF GROUP as the rotator cuff group because their distal tendons blend and attach to- The four rotator cuff muscles are gether in a cuff-shape across the greater and lesser tubercles on the head of the supraspinatus, infraspinatus, the humerus. Although all four rotator cuff muscles have specific concen- teres minor, and subscapularis (Fig- tric mover actions at the glenohumeral (GH) joint, their primary functional ure 1). These muscles are described importance is to contract isometrically for GH joint stabilization. Because 17 Before practicing any new modality or technique, check with your state’s or province’s massage therapy regulatory authority to ensure that it is within the defined scope of practice for massage therapy. the rotator cuff group has both mover and stabilization roles, it is extremely functionally active and therefore often physically stressed and injured. In fact, after neck and low back conditions, the shoulder is the most com- Supraspinatus monly injured joint of the human body. ROTATOR CUFF PATHOLOGY The three most common types of rotator cuff pathology are tendinitis, tendinosus, and tearing. Excessive physi- cal stress placed on the rotator cuff tendon can cause ir- ritation and inflammation of the tendon, in other words, tendinitis. If the physical stress is chronic, the inflam- matory process often subsides and degeneration of the fascial tendinous tissue occurs; this is referred to as tendinosus. The degeneration of tendinosus results in weakness of the tendon’s structure, and with continued Teres minor physical stress, whether it is overuse microtrauma or a macrotrauma, a rotator cuff tendon tear might occur. -

Elbow Checklist
Workbook Musculoskeletal Ultrasound September 26, 2013 Shoulder Checklist Long biceps tendon Patient position: Facing the examiner Shoulder in slight medial rotation; elbow in flexion and supination Plane/ region: Transverse (axial): from a) intraarticular portion to b) myotendinous junction (at level of the pectoralis major tendon). What you will see: Long head of the biceps tendon Supraspinatus tendon Transverse humeral ligament Subscapularis tendon Lesser tuberosity Greater tuberosity Short head of the biceps Long head of the biceps (musculotendinous junction) Humeral shaft Pectoralis major tendon Plane/ region: Logitudinal (sagittal): What you will see: Long head of biceps; fibrillar structure Lesser tuberosity Long head of the biceps tendon Notes: Subscapularis muscle and tendon Patient position: Facing the examiner Shoulder in lateral rotation; elbow in flexion/ supination Plane/ region: longitudinal (axial): full vertical width of tendon. What you will see: Subscapularis muscle, tendon, and insertion Supraspinatus tendon Coracoid process Deltoid Greater tuberosity Lesser tuberosity Notes: Do passive medial/ lateral rotation while examining Plane/ region: Transverse (sagittal): What you will see: Lesser tuberosity Fascicles of subscapularis tendon Supraspinatus tendon Patient position: Lateral to examiner Shoulder in extension and medial rotation Hand on ipsilateral buttock Plane/ region: Longitudinal (oblique sagittal) Identify the intra-articular portion of biceps LH in the transverse plane; then -

Scapular Motion Tracking Using Acromion Skin Marker Cluster: in Vitro Accuracy Assessment
Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti, Claudio Rosso, Ara Nazarian, Joseph P. DeAngelis, Arun J. Ramappa & Ugo Della Croce Journal of Medical and Biological Engineering ISSN 1609-0985 J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 1 23 Your article is protected by copyright and all rights are held exclusively by Taiwanese Society of Biomedical Engineering. This e- offprint is for personal use only and shall not be self-archived in electronic repositories. If you wish to self-archive your article, please use the accepted manuscript version for posting on your own website. You may further deposit the accepted manuscript version in any repository, provided it is only made publicly available 12 months after official publication or later and provided acknowledgement is given to the original source of publication and a link is inserted to the published article on Springer's website. The link must be accompanied by the following text: "The final publication is available at link.springer.com”. 1 23 Author's personal copy J. Med. Biol. Eng. DOI 10.1007/s40846-015-0010-2 ORIGINAL ARTICLE Scapular Motion Tracking Using Acromion Skin Marker Cluster: In Vitro Accuracy Assessment Andrea Cereatti • Claudio Rosso • Ara Nazarian • Joseph P. DeAngelis • Arun J. Ramappa • Ugo Della Croce Received: 11 October 2013 / Accepted: 20 March 2014 Ó Taiwanese Society of Biomedical Engineering 2015 Abstract Several studies have recently investigated how estimated using an AMC combined with a single anatom- the implementations of acromion marker clusters (AMCs) ical calibration, the accuracy was highly dependent on the method and stereo-photogrammetry affect the estimates of specimen and the type of motion (maximum errors between scapula kinematics. -

Structure of the Human Body
STRUCTURE OF THE HUMAN BODY Vertebral Levels 2011 - 2012 Landmarks and internal structures found at various vertebral levels. Vertebral Landmark Internal Significance Level • Bifurcation of common carotid artery. C3 Hyoid bone Superior border of thyroid C4 cartilage • Larynx ends; trachea begins • Pharynx ends; esophagus begins • Inferior thyroid A crosses posterior to carotid sheath. • Middle cervical sympathetic ganglion C6 Cricoid cartilage behind inf. thyroid a. • Inferior laryngeal nerve enters the larynx. • Vertebral a. enters the transverse. Foramen of C 6. • Thoracic duct reaches its greatest height C7 Vertebra prominens • Isthmus of thyroid gland Sternoclavicular joint (it is a • Highest point of apex of lung. T1 finger's breadth below the bismuth of the thyroid gland T1-2 Superior angle of the scapula T2 Jugular notch T3 Base of spine of scapula • Division between superior and inferior mediastinum • Ascending aorta ends T4 Sternal angle (of Louis) • Arch of aorta begins & ends. • Trachea ends; primary bronchi begin • Heart T5-9 Body of sternum T7 Inferior angle of scapula • Inferior vena cava passes through T8 diaphragm T9 Xiphisternal junction • Costal slips of diaphragm T9-L3 Costal margin • Esophagus through diaphragm T10 • Aorta through diaphragm • Thoracic duct through diaphragm T12 • Azygos V. through diaphragm • Pyloris of stomach immediately above and to the right of the midline. • Duodenojejunal flexure to the left of midline and immediately below it Tran pyloric plane: Found at the • Pancreas on a line with it L1 midpoint between the jugular • Origin of Superior Mesenteric artery notch and the pubic symphysis • Hilum of kidneys: left is above and right is below. • Celiac a. -

Bone Limb Upper
Shoulder Pectoral girdle (shoulder girdle) Scapula Acromioclavicular joint proximal end of Humerus Clavicle Sternoclavicular joint Bone: Upper limb - 1 Scapula Coracoid proc. 3 angles Superior Inferior Lateral 3 borders Lateral angle Medial Lateral Superior 2 surfaces 3 processes Posterior view: Acromion Right Scapula Spine Coracoid Bone: Upper limb - 2 Scapula 2 surfaces: Costal (Anterior), Posterior Posterior view: Costal (Anterior) view: Right Scapula Right Scapula Bone: Upper limb - 3 Scapula Glenoid cavity: Glenohumeral joint Lateral view: Infraglenoid tubercle Right Scapula Supraglenoid tubercle posterior anterior Bone: Upper limb - 4 Scapula Supraglenoid tubercle: long head of biceps Anterior view: brachii Right Scapula Bone: Upper limb - 5 Scapula Infraglenoid tubercle: long head of triceps brachii Anterior view: Right Scapula (with biceps brachii removed) Bone: Upper limb - 6 Posterior surface of Scapula, Right Acromion; Spine; Spinoglenoid notch Suprspinatous fossa, Infraspinatous fossa Bone: Upper limb - 7 Costal (Anterior) surface of Scapula, Right Subscapular fossa: Shallow concave surface for subscapularis Bone: Upper limb - 8 Superior border Coracoid process Suprascapular notch Suprascapular nerve Posterior view: Right Scapula Bone: Upper limb - 9 Acromial Clavicle end Sternal end S-shaped Acromial end: smaller, oval facet Sternal end: larger,quadrangular facet, with manubrium, 1st rib Conoid tubercle Trapezoid line Right Clavicle Bone: Upper limb - 10 Clavicle Conoid tubercle: inferior -

Trapezius Origin: Occipital Bone, Ligamentum Nuchae & Spinous Processes of Thoracic Vertebrae Insertion: Clavicle and Scapul
Origin: occipital bone, ligamentum nuchae & spinous processes of thoracic vertebrae Insertion: clavicle and scapula (acromion Trapezius and scapular spine) Action: elevate, retract, depress, or rotate scapula upward and/or elevate clavicle; extend neck Origin: spinous process of vertebrae C7-T1 Rhomboideus Insertion: vertebral border of scapula Minor Action: adducts & performs downward rotation of scapula Origin: spinous process of superior thoracic vertebrae Rhomboideus Insertion: vertebral border of scapula from Major spine to inferior angle Action: adducts and downward rotation of scapula Origin: transverse precesses of C1-C4 vertebrae Levator Scapulae Insertion: vertebral border of scapula near superior angle Action: elevates scapula Origin: anterior and superior margins of ribs 1-8 or 1-9 Insertion: anterior surface of vertebral Serratus Anterior border of scapula Action: protracts shoulder: rotates scapula so glenoid cavity moves upward rotation Origin: anterior surfaces and superior margins of ribs 3-5 Insertion: coracoid process of scapula Pectoralis Minor Action: depresses & protracts shoulder, rotates scapula (glenoid cavity rotates downward), elevates ribs Origin: supraspinous fossa of scapula Supraspinatus Insertion: greater tuberacle of humerus Action: abduction at the shoulder Origin: infraspinous fossa of scapula Infraspinatus Insertion: greater tubercle of humerus Action: lateral rotation at shoulder Origin: clavicle and scapula (acromion and adjacent scapular spine) Insertion: deltoid tuberosity of humerus Deltoid Action: -

Parts of the Body 1) Head – Caput, Capitus 2) Skull- Cranium Cephalic- Toward the Skull Caudal- Toward the Tail Rostral- Toward the Nose 3) Collum (Pl
BIO 3330 Advanced Human Cadaver Anatomy Instructor: Dr. Jeff Simpson Department of Biology Metropolitan State College of Denver 1 PARTS OF THE BODY 1) HEAD – CAPUT, CAPITUS 2) SKULL- CRANIUM CEPHALIC- TOWARD THE SKULL CAUDAL- TOWARD THE TAIL ROSTRAL- TOWARD THE NOSE 3) COLLUM (PL. COLLI), CERVIX 4) TRUNK- THORAX, CHEST 5) ABDOMEN- AREA BETWEEN THE DIAPHRAGM AND THE HIP BONES 6) PELVIS- AREA BETWEEN OS COXAS EXTREMITIES -UPPER 1) SHOULDER GIRDLE - SCAPULA, CLAVICLE 2) BRACHIUM - ARM 3) ANTEBRACHIUM -FOREARM 4) CUBITAL FOSSA 6) METACARPALS 7) PHALANGES 2 Lower Extremities Pelvis Os Coxae (2) Inominant Bones Sacrum Coccyx Terms of Position and Direction Anatomical Position Body Erect, head, eyes and toes facing forward. Limbs at side, palms facing forward Anterior-ventral Posterior-dorsal Superficial Deep Internal/external Vertical & horizontal- refer to the body in the standing position Lateral/ medial Superior/inferior Ipsilateral Contralateral Planes of the Body Median-cuts the body into left and right halves Sagittal- parallel to median Frontal (Coronal)- divides the body into front and back halves 3 Horizontal(transverse)- cuts the body into upper and lower portions Positions of the Body Proximal Distal Limbs Radial Ulnar Tibial Fibular Foot Dorsum Plantar Hallicus HAND Dorsum- back of hand Palmar (volar)- palm side Pollicus Index finger Middle finger Ring finger Pinky finger TERMS OF MOVEMENT 1) FLEXION: DECREASE ANGLE BETWEEN TWO BONES OF A JOINT 2) EXTENSION: INCREASE ANGLE BETWEEN TWO BONES OF A JOINT 3) ADDUCTION: TOWARDS MIDLINE -

Evaluation of Humeral and Glenoid Bone Deformity in Glenohumeral Arthritis 5
Evaluation of Humeral and Glenoid Bone Deformity 1 in Glenohumeral Arthritis Brian F. Grogan and Charles M. Jobin Introduction glenoid bone wear helps the surgeon formulate a successful treatment plan and surgical goals Glenohumeral arthritis is the sequela of a vari- to address the pathoanatomy and improve the ety of pathologic shoulder processes, most durability of shoulder arthroplasty. The evalu- commonly degenerative osteoarthritis, but may ation of humeral and glenoid bone deformity also be secondary to post-traumatic conditions, in glenohumeral arthritis has profound surgical inflammatory arthritis, rotator cuff tear arthrop- implications and is fundamental to successful athy, and postsurgical conditions most com- shoulder arthroplasty. monly post-capsulorrhaphy arthritis. Patients with glenohumeral arthritis commonly demon- strate patterns of bony deformity on the glenoid Glenoid Deformity in Osteoarthritis and humerus that are caused by the etiology of the arthritis. For example, osteoarthritis com- Glenoid deformity and glenohumeral subluxation monly presents with posterior glenoid wear, are commonly seen in the setting of primary osteo- secondary glenoid retroversion, and posterior arthritis of the glenohumeral joint. The glenoid humeral head subluxation, while inflammatory wear tends to occur posteriorly and may be best arthritis routinely causes concentric glenoid viewed on axial radiographs or computed tomog- wear with central glenoid erosion. A thorough raphy (CT) axial images. Glenoid erosion, as first history and physical, as well as laboratory and characterized by Walch, is noted to be either central radiographic workup, are keys to understanding or posterior, with varying degrees of wear and pos- the etiology of arthritis and understanding the terior subluxation of the humerus [1, 2] (Fig. -

Integrating the Shoulder Complex to the Body As a Whole: Practical Applications for the Dancer
RESOURCE PAPER FOR TEACHERS INTEGRATING THE SHOULDER COMPLEX TO THE BODY AS A WHOLE: PRACTICAL APPLICATIONS FOR THE DANCER LISA DONEGAN SHOAF, DPT, PHD AND JUDITH STEEL MA, CMA WITH THE IADMS DANCE EDUCATORS’ COMMITTEE, 2018. TABLE OF CONTENTS 1. Introduction 2 2. Anatomy and Movements of the Shoulder Complex 3 3. Force Couples: Muscle Connections of the Scapula and Upper Extremity 12 4. The Shoulder Joint and Rotator Cuff Muscles 17 5. Integration of the Shoulder Girdle to the Trunk, Pelvis and Lower Extremities 20 6. Common Dancer Issues in the Upper Extremity 22 7. Summary 25 8. Illustration Credits 26 9. Recommended Reading 27 10. The Authors 28 1. INTRODUCTION Figure 1: Ease and elegance in the shoulder complex The focus in many forms of dance training is often on the movements of the lower body- the legs and feet. Movement of the upper body- trunk, shoulders, and arms, is often introduced later. Because so much emphasis is placed on function of the trunk and legs, and since most injuries for dancers occur in the lower body regions, it is easy to overlook the importance of optimal function of the shoulder and arms. The shoulder complex (defined as the humerus, clavicle, sternum, and scapula bones that form a girdle or shawl over the rib cage) in combination with its connection to the trunk and, ultimately, the lower body, has many components. There are three important concepts (listed below) that, when understood and experienced, can help dance educators and dancers better make the important connections to merge maximal range of motion with well aligned and supported movements that create full body artistic expressiveness. -

Avulsion Fracture of Brachioradialis Muscle Origin: an Exceedingly Rare Entity: a Case Report
10-039_OA1 8/13/16 5:34 PM Page 50 Malaysian Orthopaedic Journal 2016 Vol 10 No 2 Behera G, et al http://dx.doi.org/10.5704/MOJ.1607.010 Avulsion Fracture of Brachioradialis Muscle Origin: An Exceedingly Rare Entity: A Case Report Behera G, DNB, Balaji G, MS Ortho, Menon J, MRCS (Edin.), Sharma D, MCH, Komuravalli VK, DNB Jawaharlal Institute of Postgraduate Medical Education and Research (JIPMER), Puducherry, India Date of submission: March 2016 Date of acceptance: June 2016 ABSTRACT lateral supracondylar ridge just proximal to the lateral epicondyle. He had restriction of active terminal elbow Avulsion fracture of the brachioradialis origin at its proximal extension by 10 degrees with near normal active elbow attachment on the lateral supracondylar ridge of the distal flexion, pronation and supination. Active flexion and humerus is exceedingly rare, and only two cases have been extension at wrist were painful along with the painful reported in the literature so far. In this article, we present a terminal elbow extension. There was significant pain at the 38 years old patient who sustained a closed avulsion fracture lateral distal humerus when active elbow flexion against of the lateral supracondylar ridge of left humerus at the resistance was performed in the mid-pronated position of the proximal attachment of brachioradialis following a fall forearm. There was no distal neurovascular deficit. backwards on outstretched hand after being struck by a lorry from behind while riding on a two-wheeler (motorcycle). He Antero-posterior (AP) plain radiograph of the left elbow was managed with above elbow plaster for four weeks showed a fracture of the lateral distal humerus at the followed by elbow and wrist mobilization. -
Scapular (Shoulder Blade) Disorders
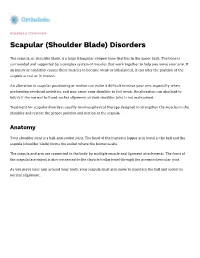
DISEASES & CONDITIONS Scapular (Shoulder Blade) Disorders The scapula, or shoulder blade, is a large triangular-shaped bone that lies in the upper back. The bone is surrounded and supported by a complex system of muscles that work together to help you move your arm. If an injury or condition causes these muscles to become weak or imbalanced, it can alter the position of the scapula at rest or in motion. An alteration in scapular positioning or motion can make it difficult to move your arm, especially when performing overhead activities, and may cause your shoulder to feel weak. An alteration can also lead to injury if the normal ball-and-socket alignment of your shoulder joint is not maintained. Treatment for scapular disorders usually involves physical therapy designed to strengthen the muscles in the shoulder and restore the proper position and motion of the scapula. Anatomy Your shoulder joint is a ball-and-socket joint. The head of the humerus (upper arm bone) is the ball and the scapula (shoulder blade) forms the socket where the humerus sits. The scapula and arm are connected to the body by multiple muscle and ligament attachments. The front of the scapula (acromion) is also connected to the clavicle (collarbone) through the acromioclavicular joint. As you move your arm around your body, your scapula must also move to maintain the ball and socket in normal alignment. (Left) The bones of the shoulder. The scapula serves as a site for the attachment of multiple muscles around the shoulder. (Right) The muscles and soft tissues of the shoulder. -

Shoulder Shoulder
SHOULDER SHOULDER ⦿ Connects arm to thorax ⦿ 3 joints ◼ Glenohumeral joint ◼ Acromioclavicular joint ◼ Sternoclavicular joint ⦿ https://www.youtube.com/watch?v=rRIz6oO A0Vs ⦿ Functional Areas ◼ scapulothoracic ◼ scapulohumeral SHOULDER MOVEMENTS ⦿ Global Shoulder ⦿ Arm (Shoulder Movement Joint) ◼ Elevation ◼ Flexion ◼ Depression ◼ Extension ◼ Abduction ◼ Abduction ◼ Adduction ◼ Adduction ◼ Medial Rotation ◼ Medial Rotation ◼ Lateral Rotation ◼ Lateral Rotation SHOULDER MOVEMENTS ⦿ Movement of shoulder can affect spine and rib cage ◼ Flexion of arm Extension of spine ◼ Extension of arm Flexion of spine ◼ Adduction of arm Ipsilateral sidebending of spine ◼ Abduction of arm Contralateral sidebending of spine ◼ Medial rotation of arm Rotation of spine ◼ Lateral rotation of arm Rotation of spine SHOULDER GIRDLE ⦿ Scapulae ⦿ Clavicles ⦿ Sternum ⦿ Provides mobile base for movement of arms CLAVICLE ⦿ Collarbone ⦿ Elongated S shaped bone ⦿ Articulates with Sternum through Manubrium ⦿ Articulates with Scapula through Acromion STERNOCLAVICULAR JOINT STERNOCLAVICULAR JOINT ⦿ Saddle Joint ◼ Between Manubrium and Clavicle ⦿ Movement ◼ Flexion - move forward ◼ Extension - move backward ◼ Elevation - move upward ◼ Depression - move downward ◼ Rotation ⦿ Usually movement happens with scapula Scapula Scapula ● Flat triangular bone ● 3 borders ○ Superior, Medial, Lateral ● 3 angles ○ Superior, Inferior, Lateral ● Processes and Spine ○ Acromion Process, Coracoid Process, Spine of Scapula ● Fossa ○ Supraspinous, Infraspinous, Subscapularis, Glenoid SCAPULA