Iccm in Mozambique Inscale Stakeholder Analysis Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

PCBG) Quarter 2 2020: January 1, 2020 – March 31, 2020, Submitted to USAID/Mozambique
Parceria Cívica para Boa Governação Program (PCBG) Quarter 2 2020: January 1, 2020 – March 31, 2020, Submitted to USAID/Mozambique PCBG Agreement No. AID-656-A-16-00003 FY20 Quarterly Report Reporting Period: January 1 to March 31, 2020 Parceria Cívica para Boa Governação Program (PCBG) Crown Prince of Norway Haakon Magnus (left) shaking hands with TV Surdo’s Executive Director Felismina Banze (right), upon his arrival at TV Surdo. Submission Date: April 30, 2020 Agreement Number: Cooperative Agreement AID-656-A-16-00003 Submitted to: Jason Smith, USAID AOR Mozambique Submitted by: Charlotte Cerf Chief of Party Counterpart International, Mozambique Email: [email protected] This document was produced for review by the United States Agency for International Development, Mozambique (USAID/Mozambique). It was prepared by Counterpart International. Parceria Cívica para Boa Governação Program (PCBG) Quarter 2 2020: January 1, 2020 – March 31, 2020, Submitted to USAID/Mozambique Table of Contents ACRONYMS AND ABBREVIATIONS ................................................................................................................ 3 EXECUTIVE SUMMARY .................................................................................................................................. 4 PROGRAM DESCRIPTION............................................................................................................................... 6 Project Overview ......................................................................................................................................................... -

Terms of Reference Conducting Viability Assessment And
Terms of Reference for Conducting viability assessment and design implementation for sustainable livelihood opportunity interventions for seven coastal fishing communities in Massinga, Vilankulo and Govuro districts, Inhambane Province 1. BACKGROUND World Wide Fund for Nature - Mozambique Country Office’s (WWF-MCO) vision is that “natural capital is well maintained and thriving, ensuring sustainable and equitable development for the wellbeing of the people of Mozambique.” This vision is intended to be achieved through four conservation goals on Governance, the Rovuma landscape, the Zambezi landscape, and the Mozambique seascape. The Mozambique seascape sub-strategy goal is that by 2020, priority coastal and marine habitats and species populations are at least maintained at 2015 levels or recovering. Three main sub- strategies are identified to achieve this, namely: (a) reducing the negative impacts from commercial and artisanal fisheries; (b) ensuring that priority habitats and coastal communities are resilient and better adapted to climate change impacts; and (c) building civil society capacity and knowledge to apply the precautionary approach to extractive industry development in marine and coastal areas. The scope for the sub strategy includes 4 specific geographical areas of focus, namely Quirimbas Archipelago (including Quirimbas National Park (QNP)) and Primeiras and Segundas Environmental Protected Area (PSEPA) in the north, the Sofala Bank fishing grounds in the center, and the Inhambane Seascape in the south. Prevailing militant insurgency in Cabo Delgado province led to WWF Mozambique taking the decision to close its operations in the area and in agreement with the primary donor, to relocate the national component of the Improving Governance, Livelihoods and Ecosystem program (SEWOH Fisheries program) to Inhambane province in 2020. -

MCHIP Leader with Associate Award GHS-A
MCHIP Leader with Associate Award GHS-A- 00-08-00002-00, Cooperative Agreement No. 656-A-00-11 -00097-00 FY2014 3rd Year of the Project Quarterly Report: April 1 to June 30, 2014 1. Project Duration: July 431, years 2014 1 2. Starting Date: April 12, 2011 3. Life of project funding: $29,835,179; will increase to $32,835,179 once Modification 6 of the Cooperative Agreement is fully executed. 4. Geographic Focus: National 5. Program/Project Objectives The goal of the MCHIP/Mozambique Associate Award is to reduce maternal, newborn and child mortality in Mozambique through the scale-up of high-impact interventions and increased use of MNCH, FP/RH, and HIV services. The project has eight objectives: • Objective 1: Work with the MOH and all USG partners to create an enabling environment at national level to provide high-impact interventions for integrated MNCH / RH / FP services in the community and Health Facilities • Objective 2: Support efforts of the MOH to increase national coverage of high impact interventions for MNCH through the expansion of the MMI, in collaboration with USG partners in all provinces • Objective 3: Support the MOH to strengthen the development of human resources for the provision of basic health services and comprehensive Emergency Obstetric and Neonatal Care and RH • Objective 4: Support the expansion of activities for prevention of cervical and breast cancer using the single-visit approach and assisting in the implementation of "Action Plan for the Strengthening of and Expansion of Services for Control of Cervical -
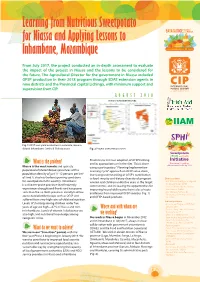
Learning from Nutritious Sweetpotato for Niassa and Applying Lessons to Inhambane, Mozambique
Learning from Nutritious Sweetpotato for Niassa and Applying Lessons to Inhambane, Mozambique From July 2017, the project conducted an in-depth assessment to evaluate the impact of the project in Niassa and the lessons to be considered for the future. The Agricultural Director for the government in Niassa included OFSP production in their 2018 program through SDAE extension agents in nine districts and the Provincial capital Lichinga, with minimum support and supervision from CIP. AUGUST 2018 PROJECT INTERVENTION ZONE Fig. 1 OFSP root yield evaluation in Colonato, Govuro district Inhambane. Credit: B. Rakotoarisoa Fig. 2 Project intervention zones Provinces to increase adoption of OFSP farming What is the problem? and its appropriate use in the diet. This is done Niassa is the most remote and sparsely using a participatory “Planning-Implemention- populated of Mozambique’s provinces with a Learning Cycle” approach on OFSP value chain¸ 2 population density of just 11-12 persons per km increasing understanding of OFSP’s contribution of land. It also has the best growing conditions to food security and dietary diversity of pregnant Direct partners for sweetpotato in the country. Inhambane women and children under five years in the target • Instituto de Investigação Agraria is a disaster-prone province that frequently de Mozambique (IIAM) communities; and increasing the opportunities for • Serviço Distrital de Actividade experiences drought and floods and has poorer improving household income from sales of roots Economicas (SDAE) soils than Niassa. Both provinces initially had low and leaves from improved OFSP varieties (Fig. 1) • Secretariado Tecnico de access to biofortified crops such as OFSP and Sugurança Alimentar e Nutrição and OFSP-based products. -

An Assessment of the Distribution and Conservation Status of Endemic and Near Endemic Plant Species in Maputaland
AN ASSESSMENT OF THE DISTRIBUTION AND CONSERVATION STATUS OF ENDEMIC AND NEAR ENDEMIC PLANT SPECIES IN MAPUTALAND Hermenegildo Alfredo Matimele Supervised by: Domitilla Raimondo, Timm Hoffman, Jonathan Timberlake, Mervyn Lötter and John Burrows Submitted in partial fulfillment of the requirements for the degree of Masters of Science in Conservation Biology Percy FitzPatrick Institute of African Ornithology University of Cape Town Rondebosch, 7701 South Africa February 2016 I PLAGIARISM DECLARATION I know that plagiarism is wrong and declare that all documents that contributed to this study have been cited and referenced. I have used the Journal of Conservation Biology as the convention for citation and referencing. Signed: Date: 15 January 2016 II ACKNOWLEDGMENTS I am sincerely grateful to all the following people who directly or indirectly contributed significantly to the success of this project. Firstly, are my supervisors: Domitilla Raimondo, for assisting me to access funding, and aiding with assessing the conservation status of the study plants; Timm Hoffman, for being a very easy going person, available at any time I needed assistance, and encouraging me through his expertise to overcome difficulties; Mervyn Lotter, for expert assistance in species distribution modeling, and in manipulating GIS for all analysis needed; John and Sandie Burrows for botanical assistance including access to their home library and herbarium, as well as the extra care when I stayed on their property; and finally to Jonathan Timberlake, for his company -

World Bank Document
The World Bank Report No: ISR16913 Implementation Status & Results Mozambique National Decentralized Planning and Finance Program (P107311) Operation Name: National Decentralized Planning and Finance Program Project Stage: Implementation Seq.No: 9 Status: ARCHIVED Archive Date: 01-Dec-2014 (P107311) Public Disclosure Authorized Country: Mozambique Approval FY: 2010 Product Line:IBRD/IDA Region: AFRICA Lending Instrument: Technical Assistance Loan Implementing Agency(ies): Key Dates Public Disclosure Copy Board Approval Date 30-Mar-2010 Original Closing Date 30-Jun-2015 Planned Mid Term Review Date 30-Jun-2013 Last Archived ISR Date 12-Jul-2014 Effectiveness Date 30-Aug-2010 Revised Closing Date 30-Jun-2015 Actual Mid Term Review Date 18-Sep-2013 Project Development Objectives Project Development Objective (from Project Appraisal Document) The Project Development Objective is to improve the capacity of local government to manage public financial resources for district development in a participatory and transparent manner. Has the Project Development Objective been changed since Board Approval of the Project? Public Disclosure Authorized Yes No Component(s) Component Name Component Cost Improving National Systems 3.20 Strengthening Participatory Planning and Budgeting 10.40 Enhancing Management and Implementation Capacity 9.20 Strengthening Oversight and Accountability 0.30 Knowledge Management 0.40 Effective Project Management and Coordination 3.90 Non-Common-Fund Activities 0.00 Public Disclosure Authorized Overall Ratings Previous Rating -

MOZAMBIQUE Food Security Outlook February to September 2017 Crisis
MOZAMBIQUE Food Security Outlook February to September 2017 Crisis outcomes expected through at least March due to drought, floods, and cyclone effects KEY MESSAGES The number of people facing Crisis (IPC Phase 3) or worse is expected to Current food security outcomes, reach about 2.3 million between now and March 2017, including potentially February 2017 300,000 flood and cyclone affected people. Household food stocks are exhausted, and poor households are relying on limited market access, wild foods, and humanitarian assistance, where available, to try to cover their food gaps. In January, food assistance covered approximately 900,000 people, representing only 45 percent of the 2 million assessed needs, and these levels are likely to continue through March 2017. Tropical Cyclone Dineo hit coastal Inhambane Province on February 15, and according to preliminary estimates, the category 3 cyclone affected nearly 551,000 people and destroyed 27,000 hectares of crops. The most vulnerable households, who already faced Crisis (IPC Phase 3) due to drought-related food gaps, are likely to face acute food shortages until at least the end of March, requiring urgent food assistance as well as seeds. Due to largely favorable rainfall, a near-average harvest is expected across southern and central areas, beginning in March, despite some areas that needed to replant due to localized flooding or faced seed access challenges. However, below-average production is likely in coastal areas of Nampula Source: FEWS NET This map represents acute food insecurity and Cabo Delgado due to erratic and poor rainfall, and to a lesser extent in outcomes relevant for emergency decision-making. -

Mozambique: Floods 000028-Moz
Revised Appeal no. MDRMZ002 GLIDE no. FL-2006-000198-TC-2007- MOZAMBIQUE: FLOODS 000028-MOZ 14 March 2007 The Federation’s mission is to improve the lives of vulnerable people by mobilizing the power of humanity. It is the world’s largest humanitarian organization and its millions of volunteers are active in over 185 countries. In Brief THIS REVISED EMERGENCY APPEAL SEEKS CHF 20,633,392 (USD 16.9m/EUR 12.8m) IN CASH, KIND, OR SERVICES TO ASSIST 117,235 BENEFICIARIES FOR 6 MONTHS <Click here to go directly to the attached Appeal budget or here to go directly to the attached map> Appeal history: · Preliminary Appeal launched on 16 February 2007 for CHF 7,464,923 (USD 5,971,938 or EUR 4,524,196) in cash, in kind or in services, for 6 months to assist 100,000 beneficiaries (20,000 families). · Disaster Relief Emergency Funds (DREF) allocated: CHF 187,000. This operation is aligned with the International Federation's Global Agenda, which sets out four broad goals to meet the Federation's mission to "improve the lives of vulnerable people by mobilizing the power of humanity". Global Agenda Goals: · Reduce the numbers of deaths, injuries and impact from disasters. · Reduce the number of deaths, illnesses and impact from diseases and public health emergencies. · Increase local community, civil society and Red Cross Red Crescent capacity to address the most urgent situations of vulnerability. · Reduce intolerance, discrimination and social exclusion and promote respect for diversity and human dignity. The situation Since December 2006, torrential rains throughout southern Africa region (from Angola in the west to Mozambique in the east with Malawi, Zambia and Zimbabwe in between) have led to overflowing of rivers and pressure on dams, resulting in wide spread flooding in central and southern parts of Mozambique. -

View of Entomology 53:387–408
International Journal of Agriculture and Environmental Research ISSN: 2455-6939 Volume:03, Issue:02 "March-April 2017" FIRST RECORD OF PARASITOIDS ASSOCIATED WITH THE INVASIVE COCONUT WHITEFLY IN INHAMBANE PROVINCE, MOZAMBIQUE 1*Ronald Kityo, 1Domingos Cugala and 2Paul Nampala 1Faculty of Agronomy and Forestry Engineering, Eduardo Mondlane University, Maputo, Mozambique 2Regional Universities Forum for Capacity Building in Agriculture (RUFORUM), Makerere University main Campus, Kampala, Uganda *Corresponding author ABSTRACT The coconut whitefly, Aleurotrachelus atratus Hempel (Homoptera; Aleyrodidea) is a highly invasive pest of coconut and ornamental palms (Arecaceae). In Mozambique, it was first detected in 2011 and 100% of infested plants have been reported. Currently, biological control is the most preferred, safest and nontoxic method in controlling invasive pest species, such as A. atratus. A study was conducted to evaluate the occurrence of parasitoids associated with A. atratus as a basis for the introduction of classical biological control in Inhambane province. Coconut leaflets were collected from five districts of the province including; Zavala, Inharrime, Jangamo, Morrumbene and Massinga districts in September and December 2015. Whitefly pupae were counted after which samples were kept in the laboratory for at least 15 days. Emerged parasitoids were identified, counted and recorded. Four parasitoid species were recovered during the study period including; Encarsia basicincta, Eretmocerus cocois, Encarsia sp. and Signiphora sp. with parasitism rates of; 4.08%, 0.22%, 5.99% and 0.45% respectively. Overall parasitism was 10.74+2.03% varying significantly among districts. The recovery of Encarsia basicincta and Eretmocerus cocois for the first time in Mozambique from the coconut whitefly is an indication that A. -
Questions on Productive Development in Mozambique
Questions on productive development in Mozambique Carlos Nuno Castel-Branco, Nelsa Massingue & Carlos Muianga (editors) IESE Questions on productive development in Mozambique Carlos Nuno Castel-Branco, Nelsa Massingue and Carlos Muianga (editors) Questions on productive development in Mozambique BACKGROUND PAPERS FOR THE DANIDA PROJECT, ‘ADVOCACY AND RESEARCH FOR PRIVAte-secTOR BUSINESS DEVELOPMENT programme’ (PSBDP 2011–2015), COORDINATED BY THE BUSINESS ENVIRONMENT Fund (FAN) Carlos Nuno Castel-Branco, Nelsa Massingue and Carlos Muianga (editors) www.iese.ac.mz Títle Questions on productive development in Mozambique Editors Carlos Nuno Castel-Branco, Nelsa Massingue and Carlos Muianga Design and layout COMPRESS.dsl Proofreading COMPRESS.dsl Printing and finishing Compress.dsl Register No. 8378/RLINLD/2015 ISBN 978–989–8464–25–5 Print run 500 Editor’s address Av. Tomás Nduda 1375 Maputo Mozambique September 2015 ACKNOWLEDGEMENTS This collection is a result of collaboration between the Institute for Social and Economic Studies (IESE) and the Business Environment Fund (FAN) and aims to transform the results of the research that has been carried out by the IESE in order to promote public-policy debate related to the development of productive capacities and business in Mozambique. The editiors of this collection would like to thank the authors of the papers and the FAN team and its partners for their valuable and critical contributions and for the suggestions. Acknowledgement is also extended to business associations, the Confederation of Business Associations (CTA), unions, the media, and all who contributed to the production and diffusion of, and debate on, the selected topics. In particular, we would like to thank the following IESE partners for their continuing institutional support: the Swiss Agency for Development and Cooperation (SDC), the Royal Danish Embassy, the Ministry for Foreign Affairs of Finland, the Irish Department of Foreign Affairs (Irish Cooperation), IBIS Mozambique, and the Embassy of Sweden. -

2 Human Interest Stories
CARE Mozambique PROSAN Human Interest Stories 2012 - 2018 PROSAN Human Interest Stories Acknowledgements CARE Mozambique wishes to acknowledge and thank the many project participants of PROSAN interviewed in the districts of Funhalouro and Homoíne, in the Inhambane province, who bravely shared their stories on how CARE, through PROSAN, brought change in their lives. Their stories generate a unique image of how the project helped the commu- nities in drought affected areas to increase the productivity and profita- bility of crops. We also want to thank the PROSAN team who wrote these stories. 2 PROSAN: Human Interest Stories : 2018 Published in February 2019 About PROSAN PROSAN is a 5 year Food and Nutrition Security Programme (2012 - 2017) that was implemented in the Funhalouro and Homoíne districts of the In- hambane Province in southern Mozambique. PROSAN has six components: conservation agriculture, Farmer Field Schools (FFS) extension model, im- proved chicken health, Village Savings and Loans Associations (VSLA), gen- der and nutrition. PROSAN also works with farmers to promote the produc- tion of the drought-resistant cashew nut as an alternative source of income, helping them become more resilient to climate change. The project is supported by the Government of Ireland, through the Irish Aid programme. PROSAN works with more than 5000 families, 69 per cent of which are women. The programme focused on women who are socially, economically and politically excluded; they are highly dependent on natural resources and are more likely to experience food and nutritional insecurity. The Embassy of Ireland has also funded the Massinga initiative on Gender and Disaster Risk Reduction (DRR), which aims to reduce the levels of gen- der based violence, and empower women to deal with natural disasters and climate change. -

Service Delivery and Support for Orphans and Vulnerable Children
Service Delivery and Support for Orphans and Vulnerable Children Quarterly Report January 1, 2018 - March 31, 2018 Submitted April 30, 2018 Award No. 656-15-00010 FHI 360 Reference No. 102248.001.001.001 Contents ACRONYMS 4 1 PROJECT OVERVIEW 6 2 HIGHLIGHTS 7 3 SUMMARY OF THE REPORTING PERIOD 7 3.1 CBO Selection, Sub-award Negotiation, Start-up and Close-out 8 3.2 CBO Management 9 3.3 Monitoring and Evaluation Systems 9 4 PROJECT IMPLEMENTATION 11 4.1 IR 1: Increased Utilization of Quality Health, Social and Nutritional Services 11 4.1.1 Mapping existing services 11 4.1.2 Identification of beneficiaries 12 4.1.3 Capacity development for high-quality case management services 13 4.1.4 Case management and service delivery 14 4.1.5 Caseload management 15 4.1.6 Transition assessment and graduation 15 4.1.7 Referrals to HIV and basic health care and other social services 16 4.1.7.1 Linkages and referrals to health providers 16 4.1.7.2 Linkages and referrals with other services 17 4.1.8 Support for adolescents 17 4.1.9 Supportive environment for OVC and healthy life choices 18 4.1.10 Provide structured TA at all levels to support operationalization of guidance and protocols 18 4.2 IR 2: Reduced Economic Vulnerability of OVC Households 19 4.2.1 Meeting basic consumption needs 19 4.2.2 Improve capacity of families to manage money and generate income 19 4.2.3 Transform resources allocation in the household in favor of OVC 20 4.2.4 Technical assistance and supervision 20 4.3 IR 3: Improved Capacity to Provide ECD Services for Vulnerable Children