COVID-19 Associated Pulmonary Embolism in Pediatric Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Diagnosing Pulmonary Embolism M Riedel
309 Postgrad Med J: first published as 10.1136/pgmj.2003.007955 on 10 June 2004. Downloaded from REVIEW Diagnosing pulmonary embolism M Riedel ............................................................................................................................... Postgrad Med J 2004;80:309–319. doi: 10.1136/pgmj.2003.007955 Objective testing for pulmonary embolism is necessary, embolism have a low long term risk of subse- quent VTE.2 5–7 because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. No single test RISK FACTORS AND RISK has ideal properties (100% sensitivity and specificity, no STRATIFICATION risk, low cost). Pulmonary angiography is regarded as the The factors predisposing to VTE broadly fit Virchow’s triad of venous stasis, injury to the final arbiter but is ill suited for diagnosing a disease vein wall, and enhanced coagulability of the present in only a third of patients in whom it is suspected. blood (box 1). The identification of risk factors Some tests are good for confirmation and some for aids clinical diagnosis of VTE and guides decisions about repeat testing in borderline exclusion of embolism; others are able to do both but are cases. Primary ‘‘thrombophilic’’ abnormalities often non-diagnostic. For optimal efficiency, choice of the need to interact with acquired risk factors before initial test should be guided by clinical assessment of the thrombosis occurs; they are usually discovered after the thromboembolic event. Therefore, the likelihood of embolism and by patient characteristics that risk of VTE is best assessed by recognising the may influence test accuracy. Standardised clinical presence of known ‘‘clinical’’ risk factors. estimates can be used to give a pre-test probability to However, investigations for thrombophilic dis- orders at follow up should be considered in those assess, after appropriate objective testing, the post-test without another apparent explanation. -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
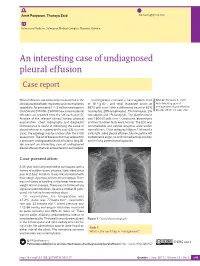
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Diagnosis of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism
Early View Review Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud, Marion Delcroix, Marc Humbert Please cite this article as: Klok FA, Couturaud F, Delcroix M, et al. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00189-2020). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2020 Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud F2, Marion Delcroix M3, Marc Humbert4-6 1 Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands 2 Département de Médecine Interne et Pneumologie, Centre Hospitalo-Universitaire de Brest, Univ Brest, EA 3878, CIC INSERM1412, Brest, France 3 Department of Respiratory Diseases, University Hospitals and Respiratory Division, Department of Chronic Diseases, Metabolism & Aging, KU Leuven – University of Leuven, Leuven, Belgium 4 Université Paris-Saclay, Faculté de Médecine, Le Kremlin-Bicêtre, France 5 Service de Pneumologie et Soins Intensifs Respiratoires, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France 6 INSERM UMR S 999, Hôpital Marie Lannelongue, Le Plessis Robinson, France Corresponding author: Frederikus A. Klok, MD, FESC; Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands; Albinusdreef 2, 2300RC, Leiden, the Netherlands; Phone: +31- 715269111; E-mail: [email protected] Abstract Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). -

Acute Pulmonary Embolism in Patients with and Without COVID-19
Journal of Clinical Medicine Article Acute Pulmonary Embolism in Patients with and without COVID-19 Antonin Trimaille 1,2 , Anaïs Curtiaud 1, Kensuke Matsushita 1,2 , Benjamin Marchandot 1 , Jean-Jacques Von Hunolstein 1 , Chisato Sato 1,2, Ian Leonard-Lorant 3, Laurent Sattler 4 , Lelia Grunebaum 4, Mickaël Ohana 3 , Patrick Ohlmann 1 , Laurence Jesel 1,2 and Olivier Morel 1,2,* 1 Division of Cardiovascular Medicine, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (A.T.); [email protected] (A.C.); [email protected] (K.M.); [email protected] (B.M.); [email protected] (J.-J.V.H.); [email protected] (C.S.); [email protected] (P.O.); [email protected] (L.J.) 2 INSERM (French National Institute of Health and Medical Research), UMR 1260, Regenerative Nanomedicine, FMTS, 67000 Strasbourg, France 3 Radiology Department, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (I.L.-L.); [email protected] (M.O.) 4 Haematology and Haemostasis Laboratory, Centre for Thrombosis and Haemostasis, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (L.S.); [email protected] (L.G.) * Correspondence: [email protected] Abstract: Introduction. Acute pulmonary embolism (APE) is a frequent condition in patients with Citation: Trimaille, A.; Curtiaud, A.; COVID-19 and is associated with worse outcomes. Previous studies suggested an immunothrombosis Matsushita, K.; Marchandot, B.; instead of a thrombus embolism, but the precise mechanisms remain unknown. -

Pulmonary Embolism Or Pneumocystis Jiroveci Pneumonia?
breathe case presentations.qxd 26/07/2006 12:03 Page 5 CASE PRESENTATION Pulmonary embolism or Pneumocystis jiroveci pneumonia? Case report Table 1 Vital signs and F. Braiteh1,2 A 33-year-old male presented to the emergency laboratory test results at I. Nash3 department with a 5-day history of exertional dys- presentation pnoea, dry cough, lethargy and an ongoing fever of 38.9°C. He had been previously diagnosed Investigation Result Normal 1Medical Oncology, Division of with left-frontal oligodendroglioma during a range Cancer Medicine, The University work-up following a new-onset seizure 4 months Vital signs of Texas M.D. Anderson Cancer Temperature °C 36.6 earlier. After successful tumour resection and Center, 2University of Texas Respiratory rate cycles·min-1 22 adjuvant radiotherapy, the patient totally recov- Graduate School of Biomedical Heart rate beats·min-1 88 ered without any residual paresis. He was main- Sciences, Houston, TX, and Blood pressure mmHg 126/64 3Dept of Pathology, Hospital of tained on valproic acid and dexamethasone at a O2 saturation % 91 Saint Raphael, Yale School of -1 dose that was tapered down to 2 mg·day . Haematological counts and coagulation Medicine, New Haven, CT, USA. The physical examination was unremarkable. White cells ×109·L -1 6.8 4.0–10.0 The patient was haemodynamically stable but Platelets ×109·L -1 123 150–350 hypoxaemic and anaemic (table 1). Chest radio- Haemoglobin g·dL-1 9.3 12.0–16.0 Correspondence: graphy and computed tomography (CT) were Prothrombine time s 12.8 <13.0 F. -

Pulmonary Embolism (Pe): Diagnosis
PULMONARY EMBOLISM (PE): DIAGNOSIS OBJECTIVE: To provide a diagnostic approach to patients with suspected acute pulmonary embolism (PE). BACKGROUND: Venous thromboembolism (VTE), which comprises deep vein thrombosis (DVT) and pulmonary embolism (PE), is a common disease, affecting approximately 1-2 in 1,000 adults per year. The diagnosis of PE has increased significantly since the advent of computed tomography pulmonary angiography (CTPA) with its widespread availability and enhanced sensitivity. The majority of PE originates in the proximal deep veins of the leg, despite the observation that only 25-50% of patients with PE have clinically evident DVT at the time of PE diagnosis. While active malignancy, surgery (especially orthopedic), hospitalization, air travel >8 hours, and hormone use/pregnancy are common transient provoking factors, approximately 50% of first-time PEs appear to be unprovoked. Symptoms of PE may include sudden onset dyspnea, pleuritic chest pain, and syncope. Signs of PE may include tachypnea, tachycardia, hypoxemia, hypotension, and features of right ventricular dysfunction (distended jugular veins). There may be accompanying signs and symptoms of DVT. The ECG may show right ventricular strain (S1Q3T3, right bundle branch block and T-inversion in leads V1- V4). Up to 10% of symptomatic PEs are fatal within the first hour of symptom onset. Independent predictors of mortality within the first few days after diagnosis of PE include hypotension (systolic blood pressure [SBP] <90 mmHg), clinical right heart failure, right ventricular dilatation on CTPA/echocardiography, positive troponin, and elevated brain natriuretic peptide (BNP). Early diagnosis and treatment of PE reduces morbidity and mortality. DIAGNOSIS OF PE: The constellation of symptoms and signs may be suggestive of PE but do not alone have the sensitivity or specificity to rule in or rule out the diagnosis. -

Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE)
How can it be prevented? You can take steps to prevent deep vein thrombosis (DVT) and pulmonary embolism (PE). If you're at risk for these conditions: • See your doctor for regular checkups. • Take all medicines as your doctor prescribes. • Get out of bed and move around as soon as possible after surgery or illness (as your doctor recommends). Moving around lowers your chance of developing a blood clot. References: • Exercise your lower leg muscles during Deep Vein Thrombosis: MedlinePlus. (n.d.). long trips. Walking helps prevent blood Retrieved October 18, 2016, from clots from forming. https://medlineplus.gov/deepveinthrombos is.html If you've had DVT or PE before, you can help prevent future blood clots. Follow the steps What Are the Signs and Symptoms of Deep above and: Vein Thrombosis? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from • Take all medicines that your doctor http://www.nhlbi.nih.gov/health/health- prescribes to prevent or treat blood clots topics/topics/dvt/signs • Follow up with your doctor for tests and treatment Who Is at Risk for Deep Vein Thrombosis? - • Use compression stockings as your DEEP NHLBI, NIH. (n.d.). Retrieved October 18, doctor directs to prevent leg swelling 2016, from http://www.nhlbi.nih.gov/health/health- VEIN topics/topics/dvt/atrisk THROMBOSIS How Can Deep Vein Thrombosis Be Prevented? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from (DVT) http://www.nhlbi.nih.gov/health/health- topics/topics/dvt/prevention How Is Deep Vein Thrombosis Treated? - NHLBI, NIH. (n.d.). Retrieved October 18, 2016, from http://www.nhlbi.nih.gov/health/health- topics/topics/dvt/treatment Trinity Surgery Center What is deep vein Who is at risk? What are the thrombosis (DVT)? The risk factors for deep vein thrombosis symptoms? (DVT) include: Only about half of the people who have DVT A blood clot that forms in a vein deep in the • A history of DVT. -

COVID19 and Pulmonary Embolism
COVID19 and Pulmonary Embolism Timothy Morris, MD Pulmonary/Critical Care, University of California, San Diego Timothy Fernandes, MD Pulmonary/Critical Care, University of California, San Diego Richard Channick, MD Pulmonary/Critical Care, University of California, Los Angeles Victor Tapson, MD Pulmonary and Critical Care, Cedars-Sinai Nicolas Gallastegui Crestani, MD Hematology, University of California, San Diego Daniel Bond, MD Pulmonary/Critical Care, University of California, San Diego COVID19 • Pathological features • Macro vs Micro • Serological markers • Epidemiology • Case presentations COVID19 • Pathological features • Macro vs Micro • Serological markers • Epidemiology • Case presentations Alveolar fibrin in COVID19-ARDS (like most ARDS) 1. Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. Lancet Respir Med. 2020;8(7):681-686. Small in situ thrombosis in COVID19-ARDS 1. Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. Lancet Respir Med. 2020;8(7):681-686. Big RV dilatation in COVID19-ARDS 1. Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. Lancet Respir Med. 2020;8(7):681-686. In situ arteriolar thrombosis in COVID19-ARDS Platelet IIIa stain megakaryocyte 1. Fox SE, Akmatbekov A, Harbert JL, Li G, Quincy Brown J, Vander Heide RS. Pulmonary and cardiac pathology in African American patients with COVID-19: an autopsy series from New Orleans. -

Pulmonary Infarction Due to Pulmonary Embolism
SYMPTOMS TO DIAGNOSIS GREGORY W. RUTECKI, MD, Section Editor MELDA SONMEZ, MD LOUTFI S. ABOUSSOUAN, MD CAROL FARVER, MD Medical Student, Koc University Department of Pulmonary, Allergy, and Critical Care Department of Pathology, Cleveland Clinic; Professor of School of Medicine, Istanbul, Turkey Medicine, Cleveland Clinic; Associate Professor of Medicine, Pathology, Cleveland Clinic Lerner College of Medicine Cleveland Clinic Lerner College of Medicine of Case Western of Case Western Reserve University, Cleveland, OH Reserve University, Cleveland, OH SUDISH C. MURTHY, MD, PhD ROOP KAW, MD Department of Thoracic and Cardiovascular Departments of Hospital Medicine and Outcomes Research Surgery, Cleveland Clinic; Professor of Surgery, Anesthesiology, Cleveland Clinic; Associate Professor of Cleveland Clinic Lerner College of Medicine of Medicine, Cleveland Clinic Lerner College of Medicine of Case Western Reserve University, Cleveland, OH Case Western University, Cleveland, OH Pulmonary infarction due to pulmonary embolism 76-year-old man whose history included □ It is rarely, if ever, associated with A abdominal aortic aneurysm repair, bilat- pulmonary embolism eral femoral artery bypass for popliteal artery □ Most patients with pleural effusion due to aneurysm, hypertension, and peptic ulcer pulmonary embolism do not have disease was admitted to a community hospi- pleuritic chest pain tal with pleuritic chest pain and shortness of □ Pulmonary embolism should be excluded breath. Two days earlier, he had undergone in all cases of pleural effusion without a repair of a ventral hernia. clear cause At the time of that admission, he reported Pulmonary embolism should be excluded in no fever, chills, night sweats, cough, or his- all cases of pleural effusion that do not have tory of heart or lung disease. -

Spontaneous Chylothorax Following Septic Pulmonary Embolization
Hindawi Case Reports in Pulmonology Volume 2020, Article ID 3979507, 3 pages https://doi.org/10.1155/2020/3979507 Case Report Spontaneous Chylothorax following Septic Pulmonary Embolization Michael Agustin , Michele Yamamoto, Chawat Tongma, Leslie Anne Chua, Michael Torres, and Scott Shay Guam Regional Medical City, 133 Route 3, Dededo Guam, USA 96929 Correspondence should be addressed to Michael Agustin; [email protected] Received 30 October 2019; Revised 19 January 2020; Accepted 12 February 2020; Published 22 February 2020 Academic Editor: Nobuyuki Koyama Copyright © 2020 Michael Agustin et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Chylothorax is the occurrence of chyle (lymph) in the pleural cavity secondary to damage of the thoracic duct. It is a rare form of pleural effusion which appears as a milky white turbid fluid. Malignancy is the leading cause of nontraumatic chylothorax while inadvertent surgical injury to the thoracic duct is the major cause of traumatic chylothorax. We report a case of spontaneous left-side chylothorax following septic pulmonary embolization (SPE) with Methicillin-Resistant Staphylococcus aureus (MRSA). This is a rare case of a nonmalignant, nontraumatic, and nontuberculous spontaneous chylothorax which was conservatively treated with fibrinolysis and diet modification. 1. Introduction with no mediastinal hilar adenopathy and no pleural effu- sion. There was no pulmonary artery filling defect or cardiac The accumulation of lymph in the pleural space due to dam- filling defect. We did not see any symptoms suggestive of age or obstruction of the thoracic duct results in chylothorax. -

Bilateral Pleural Effusions
what-mcgrath_Layout 1 03/11/10 1:49 PM Page 1879 CMAJ Practice What is your call? Bilateral pleural effusions Emmet E. McGrath MB PhD, Chris Barber MD Previously published at www.cmaj.ca See also clinical image by Yang and Liu, page 1883 Figure 1: Chest radiograph and contrast-enhanced computed tomography scan of the thorax showing bilateral pleural effusion in a 50- year-old woman with diffuse large B-cell lymphoma. 50-year-old woman presented with a short history no history or clinical evidence of cardiac, liver or renal fail- of loss of weight and appetite, constipation, right- ure, thoracentesis was performed. Milky off-white to yellow A sided abdominal pain, unsteady gait and headache. fluid was aspirated (Figure 2). It had a protein level of 10 g/L, Physical examination revealed a soft nontender abdomen a lactate dehydrogenase level of 152 IU/L, a glucose level of with normal bowel sounds. The results of respiratory, car- 8.1 mmol/L and a normal pH level. In serum samples, the diovascular and neurologic examinations were normal, as total protein level was 48 (normal 60–85) g/L and the lactate were the findings of a colonoscopy. dehydrogenase level was 858 (normal 105–333) U/L. A computed tomography (CT) scan of the abdomen showed a large solid mass in the region of the superior What is your diagnosis? mesenteric vessels. A radiograph and CT scan of the thorax were normal. A contrast-enhanced CT scan of the brain a. Cardiac failure showed a large tumour on the left side of the posterior cra- b.