Pulmonary-Embolism-Flyer.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Pleural Effusion and Ventilation/Perfusion Scan Interpretation for Acute Pulmonary Embolus
ventricular function by radionuclide angiography during exercise in normal subjects 33. Verani MS. Myocardial perfusion imaging versus two-dimensional echocardiography: and patients with chronic coronary heart disease. J Am Coll Cardiol 1983;1:1518- comparative value in the diagnosis of coronary artery disease. J NucÃCardiol 1529. 1994;1:399-414. 29. Adam WE. Tarkowska A, Bitter F, Stauch M, Geffers H. Equilibrium (gated) 34. Foster T, McNeill AJ, Salustri A, et al. Simultaneous dobutamine stress echocardiog radionuclide ventriculography. Cardiovasc Radial 1979;2:161-173. raphy and technetium-99m SPECT in patients with suspected coronary artery disease. 30. Hurwitz RA, TrêvesS, Kuroc A. Right ventricular and left ventricular ejection fraction J Am Coll Cardiol I993;21:1591-I596. in pediatrie patients with normal hearts: first pass radionuclide angiography. Am 35. Marwick TH, D'Hondt AM, Mairesse GH, Baudhuin T, Wijins W, Detry JM, Meiin Heart J 1984;107:726-732. 31. Freeman ML, Palac R, Mason J, et al. A comparison of dobutamine infusion and JA. Comparative ability of dobutamine and exercise stress in inducing myocardial ischemia in active patients. Br Heart J 1994:72:31-38. supine bicycle exercise for radionuclide cardiac stress testing. Clin NucÃMed 1984:9:251-255. 36. Senior R, Sridhara BS, Anagnostou E, Handler C, Raftery EB, Lahiri A. Synergistic 32. Cohen JL, Greene TO, Ottenweller J, Binebaum SZ, Wilchfort SD, Kim CS. value of simultaneous stress dobutamine sestamibi single-photon-emission computer Dobutamine digital echocardiography for detecting coronary artery disease. Am J ized tomography and echocardiography in the detection of coronary artery disease. -

Diagnosing Pulmonary Embolism M Riedel
309 Postgrad Med J: first published as 10.1136/pgmj.2003.007955 on 10 June 2004. Downloaded from REVIEW Diagnosing pulmonary embolism M Riedel ............................................................................................................................... Postgrad Med J 2004;80:309–319. doi: 10.1136/pgmj.2003.007955 Objective testing for pulmonary embolism is necessary, embolism have a low long term risk of subse- quent VTE.2 5–7 because clinical assessment alone is unreliable and the consequences of misdiagnosis are serious. No single test RISK FACTORS AND RISK has ideal properties (100% sensitivity and specificity, no STRATIFICATION risk, low cost). Pulmonary angiography is regarded as the The factors predisposing to VTE broadly fit Virchow’s triad of venous stasis, injury to the final arbiter but is ill suited for diagnosing a disease vein wall, and enhanced coagulability of the present in only a third of patients in whom it is suspected. blood (box 1). The identification of risk factors Some tests are good for confirmation and some for aids clinical diagnosis of VTE and guides decisions about repeat testing in borderline exclusion of embolism; others are able to do both but are cases. Primary ‘‘thrombophilic’’ abnormalities often non-diagnostic. For optimal efficiency, choice of the need to interact with acquired risk factors before initial test should be guided by clinical assessment of the thrombosis occurs; they are usually discovered after the thromboembolic event. Therefore, the likelihood of embolism and by patient characteristics that risk of VTE is best assessed by recognising the may influence test accuracy. Standardised clinical presence of known ‘‘clinical’’ risk factors. estimates can be used to give a pre-test probability to However, investigations for thrombophilic dis- orders at follow up should be considered in those assess, after appropriate objective testing, the post-test without another apparent explanation. -

Bronchiolitis Obliterans After Severe Adenovirus Pneumonia:A Review of 46 Cases
Bronchiolitis obliterans after severe adenovirus pneumonia:a review of 46 cases Yuan-Mei Lan medical college of XiaMen University Yun-Gang Yang ( [email protected] ) Xiamen University and Fujian Medical University Aliated First Hospital Xiao-Liang Lin Xiamen University and Fujian Medical University Aliated First Hospital Qi-Hong Chen Fujian Medical University Research article Keywords: Bronchiolitis obliterans, Adenovirus, Pneumonia, Children Posted Date: October 26th, 2020 DOI: https://doi.org/10.21203/rs.3.rs-93838/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/13 Abstract Background:This study aimed to investigate the risk factors of bronchiolitis obliterans caused by severe adenovirus pneumonia. Methods: The First Aliated Hospital of Xiamen University in January, 2019 was collected The clinical data of 229 children with severe adenovirus pneumonia from January to January 2020 were divided into obliterative bronchiolitis group (BO group) and non obstructive bronchiolitis group (non BO group) according to the follow-up clinical manifestations and imaging data. The clinical data, laboratory examination and imaging data of the children were retrospectively analyzed. Results: Among 229 children with severe adenovirus pneumonia, 46 cases were in BO group. The number of days of hospitalization, oxygen consumption time, LDH, IL-6, AST, D-dimer and hypoxemia in BO group were signicantly higher than those in non BO group; The difference was statistically signicant (P < 0.05). Univariate logistic regression analysis showed that there were signicant differences in the blood routine neutrophil ratio, platelet level, Oxygen supply time, hospitalization days, AST level, whether there was hypoxemia, timing of using hormone, more than two bacterial feelings were found in the two groups, levels of LDH, albumin and Scope of lung imaging (P < 0.05). -
An Interesting Case of Undiagnosed Pleural Effusion Case Report
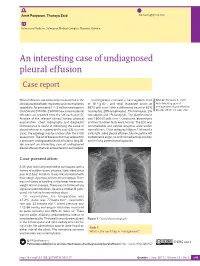
Amit Panjwani, Thuraya Zaid [email protected] Pulmonary Medicine, Salmaniya Medical Complex, Manama, Bahrain. An interesting case of undiagnosed pleural effusion Case report Pleural effusions are commonly encountered in the Investigations revealed a haemoglobin level Cite as: Panjwani A, Zaid T. clinical practise of both respiratory and nonrespiratory of 16.4 g⋅dL−1, and total leukocyte count of An interesting case of specialists. An estimated 1–1.5 million new cases in 8870 cells⋅mm−3 with a differential count of 62% undiagnosed pleural effusion. the USA and 200 000–250 000 new cases of pleural neutrophils, 28% lymphocytes, 7% monocytes, 2% Breathe 2017; 13: e46–e52. effusions are reported from the UK each year [1]. eosinophils and 1% basophils. The platelet count Analysis of the relevant clinical history, physical was 160 000 cells⋅mm−3. Creatinine, electrolytes examination, chest radiography and diagnostic and liver function tests were normal. The ECG was thoracentesis is useful in identifying the cause of unremarkable and cardiac enzymes were within pleural effusion in majority of the cases [2]. In a few normal limits. Chest radiograph (figure 1) showed a cases, the aetiology may be unclear after the initial mild, right-sided pleural effusion, blunting of the left assessment. The list of diseases that may account for costophrenic angle, no shift of mediastinal position a persistent undiagnosed pleural effusion is long [3]. and no lung parenchymal opacities. We present an interesting case of undiagnosed pleural effusion that was encountered in our hospital. R Case presentation A 33-year-old male presented to our hospital with a history of sudden-onset, pleuritic, right-sided chest pain of 2 days’ duration. -

Diagnosis of Chronic Thromboembolic Pulmonary Hypertension After Acute Pulmonary Embolism
Early View Review Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud, Marion Delcroix, Marc Humbert Please cite this article as: Klok FA, Couturaud F, Delcroix M, et al. Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Eur Respir J 2020; in press (https://doi.org/10.1183/13993003.00189-2020). This manuscript has recently been accepted for publication in the European Respiratory Journal. It is published here in its accepted form prior to copyediting and typesetting by our production team. After these production processes are complete and the authors have approved the resulting proofs, the article will move to the latest issue of the ERJ online. Copyright ©ERS 2020 Diagnosis of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism Fredrikus A. Klok, Francis Couturaud F2, Marion Delcroix M3, Marc Humbert4-6 1 Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, The Netherlands 2 Département de Médecine Interne et Pneumologie, Centre Hospitalo-Universitaire de Brest, Univ Brest, EA 3878, CIC INSERM1412, Brest, France 3 Department of Respiratory Diseases, University Hospitals and Respiratory Division, Department of Chronic Diseases, Metabolism & Aging, KU Leuven – University of Leuven, Leuven, Belgium 4 Université Paris-Saclay, Faculté de Médecine, Le Kremlin-Bicêtre, France 5 Service de Pneumologie et Soins Intensifs Respiratoires, Hôpital Bicêtre, AP-HP, Le Kremlin-Bicêtre, France 6 INSERM UMR S 999, Hôpital Marie Lannelongue, Le Plessis Robinson, France Corresponding author: Frederikus A. Klok, MD, FESC; Department of Thrombosis and Hemostasis, Leiden University Medical Center, Leiden, the Netherlands; Albinusdreef 2, 2300RC, Leiden, the Netherlands; Phone: +31- 715269111; E-mail: [email protected] Abstract Chronic thromboembolic pulmonary hypertension (CTEPH) is the most severe long-term complication of acute pulmonary embolism (PE). -

New Jersey Chapter American College of Physicians
NEW JERSEY CHAPTER AMERICAN COLLEGE OF PHYSICIANS ASSOCIATES ABSTRACT COMPETITION 2015 SUBMISSIONS 2015 Resident/Fellow Abstracts 1 1. ID CATEGORY NAME ADDITIONAL PROGRAM ABSTRACT AUTHORS 2. 295 Clinical Abed, Kareem Viren Vankawala MD Atlanticare Intrapulmonary Arteriovenous Malformation causing Recurrent Cerebral Emboli Vignette FACC; Qi Sun MD Regional Medical Ischemic strokes are mainly due to cardioembolic occlusion of small vessels, as well as large vessel thromboemboli. We describe a Center case of intrapulmonary A-V shunt as the etiology of an acute ischemic event. A 63 year old male with a past history of (Dominik supraventricular tachycardia and recurrent deep vein thrombosis; who has been non-compliant on Rivaroxaban, presents with Zampino) pleuritic chest pain and was found to have a right lower lobe pulmonary embolus. The deep vein thrombosis and pulmonary embolus were not significant enough to warrant ultrasound-enhanced thrombolysis by Ekosonic EndoWave Infusion Catheter System, and the patient was subsequently restarted on Rivaroxaban and discharged. The patient presented five days later with left arm tightness and was found to have multiple areas of punctuate infarction of both cerebellar hemispheres, more confluent within the right frontal lobe. Of note he was compliant at this time with Rivaroxaban. The patient was started on unfractionated heparin drip and subsequently admitted. On admission, his vital signs showed a blood pressure of 138/93, heart rate 65 bpm, and respiratory rate 16. Cardiopulmonary examination revealed regular rate and rhythm, without murmurs, rubs or gallops and his lungs were clear to auscultation. Neurologic examination revealed intact cranial nerves, preserved strength in all extremities, mild dysmetria in the left upper extremity and an NIH score of 1. -

Problem Based Review: Pleuritic Chest Pain
172 Acute Medicine 2012; 11(3): 172-182 Trainee Section 172 Problem based review: Pleuritic Chest Pain RW Lee, LE Hodgson, MB Jackson & N Adams Abstract Pleuritic pain, a sharp discomfort near the chest wall exacerbated by inspiration is associated with a number of pathologies. Pulmonary embolus and infection are two common causes but diagnosis can often be challenging, both for experienced physicians and trainees. The underlying anatomy and pathophysiology of such pain and the most common aetiologies are presented. Clinical symptoms and signs that may arise alongside pleuritic pain are then discussed, followed by an introduction to the diagnostic tools such as the Wells’ score and current guidelines that can help to select the most appropriate investigation(s). Management of pulmonary embolism and other common causes of pleuritic pain are also discussed and highlighted by a clinical vignette. Keywords Pleuritic pain, pulmonary embolus, pleurisy, chest pain Key Points 1. Pleuritic chest pain is a common reason for presentation to hospital. 2. Pulmonary embolism is a common, potentially life-threatening cause but can be difficult to diagnose, with clear overlap Richard William Lee between typical presentations. MBBS, MRCP, MA 3. Excluding other differential diagnoses can be difficult without definitive investigation e.g. CT Pulmonary Angiography (Cantab.) (CTPA). Respiratory Registrar, 4. Clinical probability and scoring systems (e.g. Wells’ score) can assist the physician in further management. Darent Valley Hospital 5. Several key guidelines from the thoracic and cardiological societies provide useful algorithms for investigation and further reading. Luke Eliot Hodgson MBBS, MRCP, MSc Respiratory Registrar, Introduction Brighton & Sussex Case History University Hospitals NHS Pleuritic pain is a sharp, ‘catching’ pain perceived A 37 year-old male smoker, with no previous medical Trust. -

Systemic Pulmonary Events Associated with Myelodysplastic Syndromes: a Retrospective Multicentre Study
Journal of Clinical Medicine Article Systemic Pulmonary Events Associated with Myelodysplastic Syndromes: A Retrospective Multicentre Study Quentin Scanvion 1 , Laurent Pascal 2, Thierno Sy 3, Lidwine Stervinou-Wémeau 4, Anne-Laure Lejeune 5, Valérie Deken 6, Éric Hachulla 1, Bruno Quesnel 2 , Arsène Mékinian 7, David Launay 1,8,9 and Louis Terriou 1,2,* 1 Department of Internal Medicine and Clinical Immunology, National Reference Centre for Rare Systemic Autoimmune Disease North and North-West of France, University of Lille, CHU Lille, F-59000 Lille, France; [email protected] (Q.S.); [email protected] (É.H.); [email protected] (D.L.) 2 Department of Haematology, Hôpital Saint-Vincent de Lille, Catholic University of Lille, F-59000 Lille, France; [email protected] (L.P.); [email protected] (B.Q.) 3 Internal Medicine Department, Armentières Hospital, F-59280 Armentières, France; [email protected] 4 Service de Pneumologie et ImmunoAllergologie, Centre de Référence Constitutif des Maladies Pulmonaires Rares, CHU Lille, F-59000 Lille, France; [email protected] 5 Department of Thoracic Imagining, University of Lille, CHU Lille, F-59000 Lille, France; [email protected] 6 ULR 2694—METRICS: Évaluation des Technologies de Santé et des Pratiques Médicales, University of Lille, CHU Lille, F-59000 Lille, France; [email protected] 7 Department of Internal Medicine, AP-HP, Saint-Antoine Hospital, F-75012 Paris, France; [email protected] 8 INFINITE—Institute for Translational Research in Inflammation, University of Lille, F-59000 Lille, France 9 Inserm, U1286, F-59000 Lille, France * Correspondence: [email protected] Citation: Scanvion, Q.; Pascal, L.; Sy, T.; Stervinou-Wémeau, L.; Lejeune, A.-L.; Deken, V.; Hachulla, É.; Abstract: Although pulmonary events are considered to be frequently associated with malignant Quesnel, B.; Mékinian, A.; Launay, D.; haemopathies, they have been sparsely studied in the specific context of myelodysplastic syndromes et al. -

Acute Pulmonary Embolism in Patients with and Without COVID-19
Journal of Clinical Medicine Article Acute Pulmonary Embolism in Patients with and without COVID-19 Antonin Trimaille 1,2 , Anaïs Curtiaud 1, Kensuke Matsushita 1,2 , Benjamin Marchandot 1 , Jean-Jacques Von Hunolstein 1 , Chisato Sato 1,2, Ian Leonard-Lorant 3, Laurent Sattler 4 , Lelia Grunebaum 4, Mickaël Ohana 3 , Patrick Ohlmann 1 , Laurence Jesel 1,2 and Olivier Morel 1,2,* 1 Division of Cardiovascular Medicine, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (A.T.); [email protected] (A.C.); [email protected] (K.M.); [email protected] (B.M.); [email protected] (J.-J.V.H.); [email protected] (C.S.); [email protected] (P.O.); [email protected] (L.J.) 2 INSERM (French National Institute of Health and Medical Research), UMR 1260, Regenerative Nanomedicine, FMTS, 67000 Strasbourg, France 3 Radiology Department, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (I.L.-L.); [email protected] (M.O.) 4 Haematology and Haemostasis Laboratory, Centre for Thrombosis and Haemostasis, Nouvel Hôpital Civil, Strasbourg University Hospital, 67000 Strasbourg, France; [email protected] (L.S.); [email protected] (L.G.) * Correspondence: [email protected] Abstract: Introduction. Acute pulmonary embolism (APE) is a frequent condition in patients with Citation: Trimaille, A.; Curtiaud, A.; COVID-19 and is associated with worse outcomes. Previous studies suggested an immunothrombosis Matsushita, K.; Marchandot, B.; instead of a thrombus embolism, but the precise mechanisms remain unknown. -

COVID-19 Associated Pulmonary Embolism in Pediatric Patients
Prepublication Release A N O F F I C I A L J O U R N A L O F T H E A M E R I C A N A C A D E M Y O F P E D I A T R I C S COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, Duane Williams, Neal J. Thomas, Conrad Krawiec DOI: 10.1542/hpeds.2021-005866 Journal: Hospital Pediatrics Article Type: Original Article Citation: Chima M, et al. COVID-19 Associated Pulmonary Embolism in Pediatric Patients. Hosp Pediatr. 2021; doi: 10.1542/hpeds.2021-005866 This is a prepublication version of an article that has undergone peer review and been accepted for publication but is not the final version of record. This paper may be cited using the DOI and date of access. This paper may contain information that has errors in facts, figures, and statements, and will be corrected in the final published version. The journal is providing an early version of this article to expedite access to this information. The American Academy of Pediatrics, the editors, and authors are not responsible for inaccurate information and data described in this version. Downloaded©202 from1 www.aappublications.org/news American Academy byof guest Pediatrics on October 1, 2021 Prepublication Release COVID-19 Associated Pulmonary Embolism in Pediatric Patients Melissa Chima, BS1, Duane Williams, MD2, Neal J. Thomas, MD2,3, Conrad Krawiec, MD2 Authors’ Affiliations and Addresses: 1Penn State College of Medicine, 500 University Drive, P.O. Box 850, Hershey, PA, USA 17033-0850, Tel: (717)-531-5337, Fax: (717)-531-8985. -

Acute Pleurisy in Sarcoidosis
Thorax: first published as 10.1136/thx.33.1.124 on 1 February 1978. Downloaded from Thorax, 1978, 33, 124-127 Acute pleurisy in sarcoidosis I. T. GARDINER AND J. S. UFF From the Departments of Medicine and Histopathology, Royal Postgraduate Medical School, Hammersmith Hospital, Du Cane Road, London W12 OHS, UK Gardiner, I. T., and Uff, J. S. (1978). Thorax, 33, 124-127. Acute pleurisy in sarcoidosis. A 47-year-old white man with sarcoidosis presented with a six-week history of acute painful pleurisy. On auscultation a loud pleural rub was heard at the left base together with bilateral basal crepitations. The chest radiograph showed hilar enlargement as well as diffuse lung shadowing. A lung biopsy showed the presence of numerous epithelioid and giant-cell granulomata, particularly subpleurally. A patchy interstitial pneumonia was also present. He was given a six-month course of prednisolone, and lung function returned to normal. Pleural involvement by sarcoid was thought to be were unhelpful, an open lung biopsy was per- very infrequent (Chusid and Siltzbach, 1974) until formed on 19 July 1974. Small white nodules, one recent report which gave an incidence of 1 mm across, were scattered over the visceral nearly 18% (Wilen et al., 1974). However, histo- pleura, and the lung felt firmer than normal. The logically confirmed cases remain small in number, hilar lymph nodes were enlarged and a biopsy even from very large series. Beekman et al. (1976) specimen was taken from one. have stressed that it is so unusual that pleural Two weeks later he was started on prednisolone, disease in a patient with sarcoidosis is very likely 30 mg per day. -

Pulmonary Embolism Or Pneumocystis Jiroveci Pneumonia?
breathe case presentations.qxd 26/07/2006 12:03 Page 5 CASE PRESENTATION Pulmonary embolism or Pneumocystis jiroveci pneumonia? Case report Table 1 Vital signs and F. Braiteh1,2 A 33-year-old male presented to the emergency laboratory test results at I. Nash3 department with a 5-day history of exertional dys- presentation pnoea, dry cough, lethargy and an ongoing fever of 38.9°C. He had been previously diagnosed Investigation Result Normal 1Medical Oncology, Division of with left-frontal oligodendroglioma during a range Cancer Medicine, The University work-up following a new-onset seizure 4 months Vital signs of Texas M.D. Anderson Cancer Temperature °C 36.6 earlier. After successful tumour resection and Center, 2University of Texas Respiratory rate cycles·min-1 22 adjuvant radiotherapy, the patient totally recov- Graduate School of Biomedical Heart rate beats·min-1 88 ered without any residual paresis. He was main- Sciences, Houston, TX, and Blood pressure mmHg 126/64 3Dept of Pathology, Hospital of tained on valproic acid and dexamethasone at a O2 saturation % 91 Saint Raphael, Yale School of -1 dose that was tapered down to 2 mg·day . Haematological counts and coagulation Medicine, New Haven, CT, USA. The physical examination was unremarkable. White cells ×109·L -1 6.8 4.0–10.0 The patient was haemodynamically stable but Platelets ×109·L -1 123 150–350 hypoxaemic and anaemic (table 1). Chest radio- Haemoglobin g·dL-1 9.3 12.0–16.0 Correspondence: graphy and computed tomography (CT) were Prothrombine time s 12.8 <13.0 F.