Intestinal Parasites
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bulletin Leading the Fight Against Heartworm Disease
BULLETIN LEADING THE FIGHT AGAINST HEARTWORM DISEASE SEPTEMBER HEARTWORM 2017 Q&A VOLUME 44 No. 3 Heartworm History: In What Year Was Heartworm First INSIDE THIS ISSUE Treated? Page 4 From the President Page 8 Research Update Abstracts from the Literature Page 14 Heartworm Hotline: Role of Heat Treatment in Diagnostics Page 19 NEW! Best Practices: Minimizing Heartworm Transmission in Relocated Dogs uestions from members, prac- published in the 1998 AHS Symposium 1 titioners, technicians, and the Proceedings. Dr. Roncalli wrote, “The Page 21 Qgeneral public are often submit- first trial to assess the efficacy of a Welcome Our New AHS ted to the American Heartworm Society microfilaricide (natrium antimonyl tar- Student Liaisons (AHS) via our website. Two of our AHS trate) was conducted some 70 years Board members, Dr. John W.McCall and ago (1927) in Japan by S. Itagaki and R. Page 25 Dr. Tom Nelson, provided the resources Makino.2 Fuadin (stibophen), a trivalent In the News: Surgeons to answer this question: In What Year antimony compound, was tested, intra- Remove a Heartworm from Was Heartworm First Treated? venously, as a microfilaricide by Popescu the Femoral Artery of a Cat The first efforts to treat canine heart- in 1933 in Romania and by W.H. Wright worm disease date back to the 1920s. Dr. and P.C. Underwood in 1934 in the USA. Page 26 Nelson referenced a review article by Dr. In 1949, I.C. Mark evaluated its use Quarterly Update Raffaele Roncalli, “Tracing the History of intraperitoneally.” What’s New From AHS? Heartworms: A 400 Year Perspective,” Continues on page 7 American Heartworm Society / PO Box 8266, Wilmington, DE 19803-8266 Become an American Heartworm Society www.heartwormsociety.org / [email protected] fan on Facebook! Follow us on Twitter! OUR GENEROUS SPONSORS PLATINUM LEVEL PO Box 8266 Wilmington, DE 19803-8266 [email protected] www.heartwormsociety.org Mission Statement The mission of the American Heartworm Society is to lead the vet- erinary profession and the public in the understanding of heartworm disease. -

Index Vol. 12-15
353 INDEX VOL. 12-15 Die Stichworte des Sachregisters sind in der jeweiligen Sprache der einzelnen Beitrage aufgefiihrt. Les termes repris dans la Table des matieres sont donnes selon la langue dans laquelle l'ouvrage est ecrit. The references of the Subject Index are given in the language of the respective contribution. 14 AAG (Alpha-acid glycoprotein) 120 14 Adenosine 108 12 Abortion 151 12 Adenosine-phosphate 311 13 Abscisin 12, 46, 66 13 Adenosine-5'-phosphosulfate 148 14 Absorbierbarkeit 317 13 Adenosine triphosphate 358 14 Absorption 309, 350 15 S-Adenosylmethionine 261 13 Absorption of drugs 139 13 Adipaenin (Spasmolytin) 318 14 - 15 12 Adrenal atrophy 96 14 Absorptionsgeschwindigkeit 300, 306 14 - 163, 164 14 Absorptionsquote 324 13 Adrenal gland 362 14 ACAI (Anticorticocatabolic activity in 12 Adrenalin(e) 319 dex) 145 14 - 209, 210 12 Acalo 197 15 - 161 13 Aceclidine (3-Acetoxyquinuclidine) 307, 13 {i-Adrenergic blockers 119 308, 310, 311, 330, 332 13 Adrenergic-blocking activity 56 13 Acedapsone 193,195,197 14 O(-Adrenergic blocking drugs 36, 37, 43 13 Aceperone (Acetabutone) 121 14 {i-Adrenergic blocking drugs 38 12 Acepromazin (Plegizil) 200 14 Adrenergic drugs 90 15 Acetanilid 156 12 Adrenocorticosteroids 14, 30 15 Acetazolamide 219 12 Adrenocorticotropic hormone (ACTH) 13 Acetoacetyl-coenzyme A 258 16,30,155 12 Acetohexamide 16 14 - 149,153,163,165,167,171 15 1-Acetoxy-8-aminooctahydroindolizin 15 Adrenocorticotropin (ACTH) 216 (Slaframin) 168 14 Adrenosterone 153 13 4-Acetoxy-1-azabicyclo(3, 2, 2)-nonane 12 Adreson 252 -

(12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 De Juan Et Al
US 200601 10428A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2006/0110428A1 de Juan et al. (43) Pub. Date: May 25, 2006 (54) METHODS AND DEVICES FOR THE Publication Classification TREATMENT OF OCULAR CONDITIONS (51) Int. Cl. (76) Inventors: Eugene de Juan, LaCanada, CA (US); A6F 2/00 (2006.01) Signe E. Varner, Los Angeles, CA (52) U.S. Cl. .............................................................. 424/427 (US); Laurie R. Lawin, New Brighton, MN (US) (57) ABSTRACT Correspondence Address: Featured is a method for instilling one or more bioactive SCOTT PRIBNOW agents into ocular tissue within an eye of a patient for the Kagan Binder, PLLC treatment of an ocular condition, the method comprising Suite 200 concurrently using at least two of the following bioactive 221 Main Street North agent delivery methods (A)-(C): Stillwater, MN 55082 (US) (A) implanting a Sustained release delivery device com (21) Appl. No.: 11/175,850 prising one or more bioactive agents in a posterior region of the eye so that it delivers the one or more (22) Filed: Jul. 5, 2005 bioactive agents into the vitreous humor of the eye; (B) instilling (e.g., injecting or implanting) one or more Related U.S. Application Data bioactive agents Subretinally; and (60) Provisional application No. 60/585,236, filed on Jul. (C) instilling (e.g., injecting or delivering by ocular ion 2, 2004. Provisional application No. 60/669,701, filed tophoresis) one or more bioactive agents into the Vit on Apr. 8, 2005. reous humor of the eye. Patent Application Publication May 25, 2006 Sheet 1 of 22 US 2006/0110428A1 R 2 2 C.6 Fig. -
Computational Studies of Drug Repurposing Targeting P-Glycoprotein Mediated Multidrug-Resistance Phenotypes in Agents of Neglect
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.12.147926; this version posted June 12, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Computational studies of drug repurposing targeting P- glycoprotein mediated multidrug-resistance phenotypes in agents of neglected tropical diseases Nivedita Jaishankar 1, Sangeetha Muthamilselvan 2, Ashok Palaniappan 1,2* 1 Department of Biotechnology, Sri Venkateswara College of Engineering, Post Bag No. 1, Pennalur, Sriperumbudur Tk 602117. India 2 Department of Bioinformatics, School of Chemical and BioTechnology, SASTRA Deemed University, Thanjavur 613401. India * Corresponding author: [email protected] ABSTRACT Mammalian ABCB1 P-glycoprotein is an ATP- dependent efflux pump with broad substrate specificity associated with cellular drug resistance. Homologous to this role in mammalian biology, the P-glycoprotein of agents of neglected tropical diseases (NTDs) mediates the emergence of multidrug- resistance phenotypes. The clinical and socioeconomic implications of NTDs are exacerbated by the lack of research interest among Big Pharma for treating such conditions. This work aims to characterise P-gp homologues in certain agents of key NTDs, namely (1) Protozoa: Leishmania major, Trypanosoma cruzi; (2) Helminths: Onchocerca volvulus, Schistosoma mansoni. PSI-BLAST searches against the genome of each of these organisms confirmed the presence of P-gp homologues. Each homologue was aligned against five P- gp sequences of known structure, to identify the most suitable template based on sequence homology, phylogenetic nearest neighbor, and query coverage. -

ANTIPARASITAIRES Mécanismes D’Action
ANTIPARASITAIRES Mécanismes d’action Pr Ag Anis KLOUZ Service de Pharmacologie Clinique, Centre National de Pharmacovigilance & Faculté de Médecine de Tunis DDÉÉFINITIONSFINITIONS Antiparasitaires : substances d’origine naturelle ou de synthèse capables de détruire différents organismes ayant un développement parasite Regroupe des médicaments et des pesticides : insecticides, anthelminthiques, antifongiques, protozoocides Critères d’efficacité 1- Agir sur le parasite 2- Atteindre des localisations parfois profondes 3- Etre actif sur différents stades Critères de sélectivité 1- Mécanisme d’action spécifique 2- Pharmacocinétique particulière Facteurs liés à l’hôte • Anatomie, physiologie –mammifères – oiseaux (reptiles …) • Diversité des espèces atteintes – animaux de compagnie – animaux de production • Diversité de localisation • Impératifs économiques • Protection de l’environnement • Absence de toxicité Facteurs liés aux parasites • Anatomie, physiologie • Diversité des espèces pathogènes – Insectes, acariens – Nématodes, trématodes, cestodes • Diversité de localisation – Ex des gales: invasion variable de l’épiderme – Ex des nématodes: digestifs, respiratoires, sanguins … • Diversité des stades d’évolution – œufs, larves, adultes – contamination de l’hôte et de l’environnement • Difficulté des études in vitro Anatomie Organe de prédation, fixation TD, organe de reproduction Cuticule CT Helminthe Structure de la cuticule Perméabilité de la cuticule • Perméabilité : – Aux composés lipophiles (diffusion des acides gras volatils à travers -

Lecture 5: Emerging Parasitic Helminths Part 2: Tissue Nematodes
Readings-Nematodes • Ch. 11 (pp. 290, 291-93, 295 [box 11.1], 304 [box 11.2]) • Lecture 5: Emerging Parasitic Ch.14 (p. 375, 367 [table 14.1]) Helminths part 2: Tissue Nematodes Matt Tucker, M.S., MSPH [email protected] HSC4933 Emerging Infectious Diseases HSC4933. Emerging Infectious Diseases 2 Monsters Inside Me Learning Objectives • Toxocariasis, larva migrans (Toxocara canis, dog hookworm): • Understand how visceral larval migrans, cutaneous larval migrans, and ocular larval migrans can occur Background: • Know basic attributes of tissue nematodes and be able to distinguish http://animal.discovery.com/invertebrates/monsters-inside- these nematodes from each other and also from other types of me/toxocariasis-toxocara-roundworm/ nematodes • Understand life cycles of tissue nematodes, noting similarities and Videos: http://animal.discovery.com/videos/monsters-inside- significant difference me-toxocariasis.html • Know infective stages, various hosts involved in a particular cycle • Be familiar with diagnostic criteria, epidemiology, pathogenicity, http://animal.discovery.com/videos/monsters-inside-me- &treatment toxocara-parasite.html • Identify locations in world where certain parasites exist • Note drugs (always available) that are used to treat parasites • Describe factors of tissue nematodes that can make them emerging infectious diseases • Be familiar with Dracunculiasis and status of eradication HSC4933. Emerging Infectious Diseases 3 HSC4933. Emerging Infectious Diseases 4 Lecture 5: On the Menu Problems with other hookworms • Cutaneous larva migrans or Visceral Tissue Nematodes larva migrans • Hookworms of other animals • Cutaneous Larva Migrans frequently fail to penetrate the human dermis (and beyond). • Visceral Larva Migrans – Ancylostoma braziliense (most common- in Gulf Coast and tropics), • Gnathostoma spp. Ancylostoma caninum, Ancylostoma “creeping eruption” ceylanicum, • Trichinella spiralis • They migrate through the epidermis leaving typical tracks • Dracunculus medinensis • Eosinophilic enteritis-emerging problem in Australia HSC4933. -

)&F1y3x PHARMACEUTICAL APPENDIX to THE
)&f1y3X PHARMACEUTICAL APPENDIX TO THE HARMONIZED TARIFF SCHEDULE )&f1y3X PHARMACEUTICAL APPENDIX TO THE TARIFF SCHEDULE 3 Table 1. This table enumerates products described by International Non-proprietary Names (INN) which shall be entered free of duty under general note 13 to the tariff schedule. The Chemical Abstracts Service (CAS) registry numbers also set forth in this table are included to assist in the identification of the products concerned. For purposes of the tariff schedule, any references to a product enumerated in this table includes such product by whatever name known. Product CAS No. Product CAS No. ABAMECTIN 65195-55-3 ACTODIGIN 36983-69-4 ABANOQUIL 90402-40-7 ADAFENOXATE 82168-26-1 ABCIXIMAB 143653-53-6 ADAMEXINE 54785-02-3 ABECARNIL 111841-85-1 ADAPALENE 106685-40-9 ABITESARTAN 137882-98-5 ADAPROLOL 101479-70-3 ABLUKAST 96566-25-5 ADATANSERIN 127266-56-2 ABUNIDAZOLE 91017-58-2 ADEFOVIR 106941-25-7 ACADESINE 2627-69-2 ADELMIDROL 1675-66-7 ACAMPROSATE 77337-76-9 ADEMETIONINE 17176-17-9 ACAPRAZINE 55485-20-6 ADENOSINE PHOSPHATE 61-19-8 ACARBOSE 56180-94-0 ADIBENDAN 100510-33-6 ACEBROCHOL 514-50-1 ADICILLIN 525-94-0 ACEBURIC ACID 26976-72-7 ADIMOLOL 78459-19-5 ACEBUTOLOL 37517-30-9 ADINAZOLAM 37115-32-5 ACECAINIDE 32795-44-1 ADIPHENINE 64-95-9 ACECARBROMAL 77-66-7 ADIPIODONE 606-17-7 ACECLIDINE 827-61-2 ADITEREN 56066-19-4 ACECLOFENAC 89796-99-6 ADITOPRIM 56066-63-8 ACEDAPSONE 77-46-3 ADOSOPINE 88124-26-9 ACEDIASULFONE SODIUM 127-60-6 ADOZELESIN 110314-48-2 ACEDOBEN 556-08-1 ADRAFINIL 63547-13-7 ACEFLURANOL 80595-73-9 ADRENALONE -
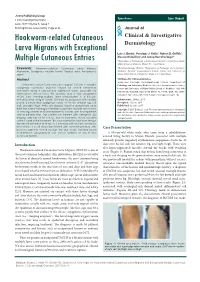
Hookworm-Related Cutaneous Larva Migrans with Exceptional Multiple Cutaneous Entries
Open Access Case Report J Clin Investigat Dermatol June 2017 Volume 5, Issue 1 © All rights are reserved by Vega et al. Journal of Hookworm-related Cutaneous Clinical & Investigative Larva Migrans with Exceptional Dermatology Luis J. Borda1, Penelope J. Kallis1, Robert D. Griffith1, Alessio Giubellino1 and Jeong Hee Cho-Vega2* Multiple Cutaneous Entries 1Department of Dermatology and Cutaneous Surgery, University of Miami Miller School of Medicine, Miami, FL, United States Keywords: Hookworm-related Cutaneous Larva Migrans; 2Dermatopathology Division, Department of Pathology and Laboratory Hookworm; Serpiginous multiple tracks; Tropical area; Anti-parasite Medicine, Sylvester Comprehensive Cancer Center and University of agent Miami Miller School of Medicine, Miami, FL, United States Abstract *Address for Correspondence Jeong Hee Cho-Vega, Dermatopathology Division, Department of Hookworm-related Cutaneous Larva Migrans (HrCLM) is a pruritic Pathology and Laboratory Medicine Sylvester Comprehensive Cancer serpiginous cutaneous eruption caused by animal hookworms Center and University of Miami Miller School of Medicine 1120 NW commonly found in tropical and subtropical areas, especially the 14th Street, Holtz ET, Suite 2146 Miami, FL 33136, USA, Tel: (305)- Southeastern United States. We describe here a very exceptional 243-6433; Fax: (305)-243-1624; E-mail: [email protected] HrCLM case showing multiple larva entries/lesions in a 63-year- old white male living in Miami. Clinically he presented with multiple Submission: 25 May, 2017 pruritic erythematous serpiginous tracks on his left anterior leg, left Accepted: 15 June, 2017 calf, and right thigh. While skin biopsies failed to demonstrate larva Published: 22 June, 2017 itself, the overall histological features supported multiple larva tracks Copyright: © 2017 Borda LJ, et al. -

A Parasite of Red Grouse (Lagopus Lagopus Scoticus)
THE ECOLOGY AND PATHOLOGY OF TRICHOSTRONGYLUS TENUIS (NEMATODA), A PARASITE OF RED GROUSE (LAGOPUS LAGOPUS SCOTICUS) A thesis submitted to the University of Leeds in fulfilment for the requirements for the degree of Doctor of Philosophy By HAROLD WATSON (B.Sc. University of Newcastle-upon-Tyne) Department of Pure and Applied Biology, The University of Leeds FEBRUARY 198* The red grouse, Lagopus lagopus scoticus I ABSTRACT Trichostrongylus tenuis is a nematode that lives in the caeca of wild red grouse. It causes disease in red grouse and can cause fluctuations in grouse pop ulations. The aim of the work described in this thesis was to study aspects of the ecology of the infective-stage larvae of T.tenuis, and also certain aspects of the pathology and immunology of red grouse and chickens infected with this nematode. The survival of the infective-stage larvae of T.tenuis was found to decrease as temperature increased, at temperatures between 0-30 C? and larvae were susceptible to freezing and desiccation. The lipid reserves of the infective-stage larvae declined as temperature increased and this decline was correlated to a decline in infectivity in the domestic chicken. The occurrence of infective-stage larvae on heather tips at caecal dropping sites was monitored on a moor; most larvae were found during the summer months but very few larvae were recovered in the winter. The number of larvae recovered from the heather showed a good correlation with the actual worm burdens recorded in young grouse when related to food intake. Examination of the heather leaflets by scanning electron microscopy showed that each leaflet consists of a leaf roll and the infective-stage larvae of T.tenuis migrate into the humid microenvironment' provided by these leaf rolls. -

Waterborne Zoonotic Helminthiases Suwannee Nithiuthaia,*, Malinee T
Veterinary Parasitology 126 (2004) 167–193 www.elsevier.com/locate/vetpar Review Waterborne zoonotic helminthiases Suwannee Nithiuthaia,*, Malinee T. Anantaphrutib, Jitra Waikagulb, Alvin Gajadharc aDepartment of Pathology, Faculty of Veterinary Science, Chulalongkorn University, Henri Dunant Road, Patumwan, Bangkok 10330, Thailand bDepartment of Helminthology, Faculty of Tropical Medicine, Mahidol University, Ratchawithi Road, Bangkok 10400, Thailand cCentre for Animal Parasitology, Canadian Food Inspection Agency, Saskatoon Laboratory, Saskatoon, Sask., Canada S7N 2R3 Abstract This review deals with waterborne zoonotic helminths, many of which are opportunistic parasites spreading directly from animals to man or man to animals through water that is either ingested or that contains forms capable of skin penetration. Disease severity ranges from being rapidly fatal to low- grade chronic infections that may be asymptomatic for many years. The most significant zoonotic waterborne helminthic diseases are either snail-mediated, copepod-mediated or transmitted by faecal-contaminated water. Snail-mediated helminthiases described here are caused by digenetic trematodes that undergo complex life cycles involving various species of aquatic snails. These diseases include schistosomiasis, cercarial dermatitis, fascioliasis and fasciolopsiasis. The primary copepod-mediated helminthiases are sparganosis, gnathostomiasis and dracunculiasis, and the major faecal-contaminated water helminthiases are cysticercosis, hydatid disease and larva migrans. Generally, only parasites whose infective stages can be transmitted directly by water are discussed in this article. Although many do not require a water environment in which to complete their life cycle, their infective stages can certainly be distributed and acquired directly through water. Transmission via the external environment is necessary for many helminth parasites, with water and faecal contamination being important considerations. -

Public Health Significance of Intestinal Parasitic Infections*
Articles in the Update series Les articles de la rubrique give a concise, authoritative, Le pointfournissent un bilan and up-to-date survey of concis et fiable de la situa- the present position in the tion actuelle dans les do- Update selectedfields, coveringmany maines consideres, couvrant different aspects of the de nombreux aspects des biomedical sciences and sciences biomedicales et de la , po n t , , public health. Most of santepublique. Laplupartde the articles are written by ces articles auront donc ete acknowledged experts on the redigeis par les specialistes subject. les plus autorises. Bulletin of the World Health Organization, 65 (5): 575-588 (1987) © World Health Organization 1987 Public health significance of intestinal parasitic infections* WHO EXPERT COMMITTEE' Intestinal parasitic infections are distributed virtually throughout the world, with high prevalence rates in many regions. Amoebiasis, ascariasis, hookworm infection and trichuriasis are among the ten most common infections in the world. Other parasitic infections such as abdominal angiostrongyliasis, intestinal capil- lariasis, and strongyloidiasis are of local or regional public health concern. The prevention and control of these infections are now more feasible than ever before owing to the discovery of safe and efficacious drugs, the improvement and sim- plification of some diagnostic procedures, and advances in parasite population biology. METHODS OF ASSESSMENT The amount of harm caused by intestinal parasitic infections to the health and welfare of individuals and communities depends on: (a) the parasite species; (b) the intensity and course of the infection; (c) the nature of the interactions between the parasite species and concurrent infections; (d) the nutritional and immunological status of the population; and (e) numerous socioeconomic factors. -

Hymenolepiasis in a Pregnant Woman: a Case Report of Hymenolepis Nana Infection
Open Access Case Report DOI: 10.7759/cureus.3810 Hymenolepiasis in a Pregnant Woman: A Case Report of Hymenolepis nana Infection Venkataramana Kandi 1 , Sri Sandhya Koka 1 , Mohan Rao Bhoomigari 1 1. Microbiology, Prathima Institute of Medical Sciences, Karimnagar, IND Corresponding author: Venkataramana Kandi, [email protected] Abstract Hymenolepiasis is an infection caused by Hymenolepis nana (H. nana) and H. diminuta (H. diminuta). Hymenolepiasis is prevalent throughout the world with human infections with H. nana being frequently reported in the literature as compared to H. diminuta. Hymenolepiasis is more frequent among children, and most human infections remain asymptomatic and self-limited. Symptoms including abdominal pain, diarrhea, and vomiting are frequently noted in the cases of heavy infections. We report a case of hymenolepiasis caused by H. nana in a pregnant woman. Categories: Obstetrics/Gynecology, Infectious Disease, Public Health Keywords: hymenolepiasis, hymenolepis nana, h. nana, h. diminuta, children, adults, asymptomatic, pregnant woman Introduction Human infection caused by the cestodes belonging to the genus Hymenolepis is called as hymenolepiasis. The cestodes are broadly classified as pseudophyllidean and cyclophyllidean cestodes. Hymenolepis species (spp.) fall into the cyclophyllidean group, which is characterized by the presence of four cup-like structures in the scolex/head called as suckers. The suckers are either armed (presence of hook-like structures) or unarmed (no hooks). Hymenolepis spp. are armed with the presence of a single round of hooks around the suckers. Among the Hymenolepis spp., H. nana is commonly called as a dwarf tapeworm and H. diminuta is referred to as a rat tapeworm. H. nana frequently causes human infections and may also cause infections in rats, whereas H.