Nerve Ultrasound in Traumatic and Iatrogenic Peripheral Nerve Injury
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Schwann Cell Supplementation in Neurosurgical Procedures After Neurotrauma Santiago R
ll Scienc Ce e f & o T l h a e Unda, J Cell Sci Ther 2018, 9:2 n r a r a p p u u DOI: 10.4172/2157-7013.1000281 y y o o J J Journal of Cell Science & Therapy ISSN: 2157-7013 Review Open Access Schwann Cell Supplementation in Neurosurgical Procedures after Neurotrauma Santiago R. Unda* Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina *Corresponding author: Santiago R. Unda, Instituto de Biotecnología, Centro de Investigación e Innovación Tecnológica, Universidad Nacional de La Rioja, Argentina, Tel: 3804277348; E-mail: [email protected] Rec Date: January 12, 2018, Acc Date: March 13, 2018, Pub Date: March 16, 2018 Copyright: © 2018 Santiago R. Unda. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Nerve trauma is a common cause of quality of life decline, especially in young people. Causing a high impact in personal, psychological and economic issues. The Peripheral Nerve Injury (PNI) with a several grade of axonotmesis and neurotmesis represents a real challenge for neurosurgeons. However, the basic science has greatly contribute to axonal degeneration and regeneration knowledge, making possible to implement in new protocols with molecular and cellular techniques for improve nerve re-growth and to restore motor and sensitive function. The Schwann cell transplantation from different stem cells origins is one of the potential tools for new therapies. In this briefly review is included the recent results of animal and human neurosurgery protocols of Schwann cells transplantation for nerve recovery after a PNI. -

Types and Classification of Nerve Injury: a Review
Indian Journal of Clinical Practice, Vol. 31, No. 5, October 2020 REVIEW ARTICLE Types and Classification of Nerve Injury: A Review R JAYASRI KRUPAA*, KMK MASTHAN†, ARAVINTHA BABU N‡, SONA B# ABSTRACT Nerve injuries are the most common conditions with varying symptoms, depending on the severity, intensity and nerves involved. Though much information is available on the mechanisms of injury and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve injuries and their classification. Keywords: Axonotmesis, neurotmesis, neurapraxia, Wallerian degeneration erve injuries are the most common conditions bundles of fibers called fascicles, which are covered with varying symptoms depending on the by perineurium. severity, intensity and nerves involved. N Â Epineurium: Finally, groups of fascicles are bundled Recovery after any nerve injury is variable. Though together to form the peripheral nerve (such as the much information exists on the mechanisms of injury median nerve), which is covered by epineurium. and regeneration, reliable treatments that ensure full functional recovery are limited. The type of nerve CLASSIFICATION injury alters the treatment and prognosis. This review article aims to summarize the various types of nerve Classification by Type of Nerve Injury injuries and classification of nerve injuries, which is There are three types of nerve injuries: useful in understanding their pathological basis, and to evaluate the prognosis for recovery. Nerve section Understanding the basic nerve anatomy is important Nerve section can be partial or complete, sharp or for the classification and also essential to evaluate blunt. -

Strategies to Improve Nerve Regeneration After Radical Prostatectomy: a Narrative Review
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Institutional Research Information System University of Turin Strategies to improve nerve regeneration after radical prostatectomy: a narrative review Stefano Geuna 1, 2, Luisa Muratori1, 2, Federica Fregnan 1, 2, Matteo Manfredi4 , Riccardo Bertolo 3, 4 , Francesco Porpiglia4. 1 Department of Clinical and Biological Sciences, University of Turin, Orbassano (To), 10043, Italy. 2 Neuroscience Institute Cavalieri Ottolenghi (NICO), Orbassano (To), 10043, Italy. 3 Urological and Kidney Institute, Cleveland Clinic, Cleveland, OH, US. 4 Department of Oncology, University of Turin, Orbassano (To), 10043, Italy. Abstract Peripheral nerves are complex organs that spread throughout the entire human body. They are frequently affected by lesions not only as a result of trauma but also following radical tumor resection. In fact, despite the advancement in surgical techniques, such as nerve- sparing robot assisted radical prostatectomy, some degree of nerve injury may occur resulting in erectile dysfunction with significant impairment of the quality of life. The aim of this review is to provide an overview on the mechanisms of the regeneration of injured peripheral nerves and to describe the potential strategies to improve the regeneration process and the functional recovery. Yet, the recent advances in bio- engineering strategies to promote nerve regeneration in the urological field are outlined with a view on the possible future regenerative therapies which might ameliorate the functional outcome after radical prostatectomy. 1 Introduction Radical prostatectomy is the gold standard surgical treatment for organ-confined prostate cancer. The employment of innovative surgical technique such as nerve-sparing robot assisted radical prostatectomy allowed to magnify the anatomical field leading to a three- dimensional perspective obtained through the robotic lenses and a better anatomical knowledge. -
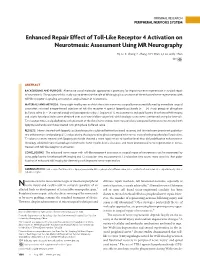
Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography
ORIGINAL RESEARCH PERIPHERAL NERVOUS SYSTEM Enhanced Repair Effect of Toll-Like Receptor 4 Activation on Neurotmesis: Assessment Using MR Neurography H.J. Li, X. Zhang, F. Zhang, X.H. Wen, L.J. Lu, and J. Shen ABSTRACT BACKGROUND AND PURPOSE: Alternative use of molecular approaches is promising for improving nerve regeneration in surgical repair of neurotmesis. The purpose of this study was to determine the role of MR imaging in assessment of the enhanced nerve regeneration with toll-like receptor 4 signaling activation in surgical repair of neurotmesis. MATERIALS AND METHODS: Forty-eight healthy rats in which the sciatic nerve was surgically transected followed by immediate surgical coaptation received intraperitoneal injection of toll-like receptor 4 agonist lipopolysaccharide (n ϭ 24, study group) or phosphate buffered saline (n ϭ 24, control group) until postoperative day 7. Sequential T2 measurements and gadofluorine M-enhanced MR imaging and sciatic functional index were obtained over an 8-week follow-up period, with histologic assessments performed at regular intervals. T2 relaxation times and gadofluorine enhancement of the distal nerve stumps were measured and compared between nerves treated with lipopolysaccharide and those treated with phosphate buffered saline. RESULTS: Nerves treated with lipopolysaccharide injection achieved better functional recovery and showed more prominent gadofluo- rine enhancement and prolonged T2 values during the degenerative phase compared with nerves treated with phosphate buffered saline. T2 values in nerves treated with lipopolysaccharide showed a more rapid return to baseline level than did gadofluorine enhancement. Histology exhibited more macrophage recruitment, faster myelin debris clearance, and more pronounced nerve regeneration in nerves treated with toll-like receptor 4 activation. -

Some Aspects of Facial Nerve Paralysis* PART Li
13 Januarie 1973 S.-A. MEDIESE TVDSKRIF 65 Some Aspects of Facial Nerve Paralysis* PART lI. ELECTRICAL TESTS AND THE SUBMAXILLARY SALlYARY TEST M. G. POTGIETER,t M.B. CH.B. UNIV. PRET., M.MED. OTOL. UNIV. CAPE TOWN, Department of Otolaryngology, Groote Schuur Hospital, Observatory, Cape SUMMARY fibres are the first to be affected and when there is re generation, the new fibres conduct slowly.' The submaxillary salivary flow test gives reliable in The maintenance of nerve and muscle excitability de formation as to whether neurapraxia, axono:mesis, or pends greatly upon sodium and potassium cations. States neurotmesis of the facial nerve is present. This can be of polarization and depolarization are dependent on the corroborated by electrical studies. This test can make an shift of sodium and potassium cations across the cell important contribution to the topognosis and prognosis of membranes. With injury to the nerve;" elimination of facial paralysis, especially when elaborate electrical the membrane potential takes place and this causes a lack equipment for nerve excitability tests and electromyo of electrical conduction. A shift of potassium from the graphy is not available. cell takes place. An over-all increase in the potassium content of the injured nerve exists where, for instance, S. Afr. Med. J., 47, 65 (1973). bone fragments cause a foreign body reaction. Hyaluronic acid from an inflammatory response, occurs as a potas sium hyaluronate. Fibroblast and mast-cell activities in ELECTRlCAL TESTS crease and elaborate mucopolysaccharides. This may explain the high potassium values, maintained in the In 1872 Duchenne described the technique of nerve ex injured area of the nerve, inhibiting transmission. -

Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging
741 Wallerian Degeneration and Inflammation in Rat Peripheral Nerve Detected by in Vivo MR Imaging DavidS. Titelbaum 1 To investigate the role of MR imaging in wallerian degeneration, a series of animal Joel L. Frazier 2 models of increasingly complex peripheral nerve injury were studied by in vivo MR. Robert I. Grossman 1 Proximal tibial nerves in brown Norway rats were either crushed, transected (neurotomy), Peter M. Joseph 1 or transected and grafted with Lewis rat (allograft) or brown Norway (isograft) donor Leonard T. Yu 2 nerves. The nerves distal to the site of injury were imaged at intervals of 0-54 days after surgery. Subsequent histologic analysis was obtained and correlated with MR Eleanor A. Kassab 1 3 findings. Crush injury, neurotomy, and nerve grafting all resulted in high signal intensity William F. Hickey along the course of the nerve observed on long TR/TE sequences, corresponding to 2 Don LaRossa edema and myelin breakdown from wallerian degeneration. The abnormal signal inten 4 Mark J. Brown sity resolved by 30 days after crush injury and by 45-54 days after neurotomy, when the active changes of wallerian degeneration had subsided. These changes were not seen in sham-operated rats. Our findings suggest that MR is capable of identifying traumatic neuropathy in a peripheral nerve undergoing active wallerian degeneration. The severity of injury may be reflected by the corresponding duration of signal abnormality. With the present methods, MR did not distinguish inflammatory from simple posttraumatic neuropathy. Wallerian degeneration is the axonal degeneration and loss of myelin that occurs when an axon is separated from its cell body. -

Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies
Anatomical, Clinical, and Electrodiagnostic Features of Radial Neuropathies a, b Leo H. Wang, MD, PhD *, Michael D. Weiss, MD KEYWORDS Radial Posterior interosseous Neuropathy Electrodiagnostic study KEY POINTS The radial nerve subserves the extensor compartment of the arm. Radial nerve lesions are common because of the length and winding course of the nerve. The radial nerve is in direct contact with bone at the midpoint and distal third of the humerus, and therefore most vulnerable to compression or contusion from fractures. Electrodiagnostic studies are useful to localize and characterize the injury as axonal or demyelinating. Radial neuropathies at the midhumeral shaft tend to have good prognosis. INTRODUCTION The radial nerve is the principal nerve in the upper extremity that subserves the extensor compartments of the arm. It has a long and winding course rendering it vulnerable to injury. Radial neuropathies are commonly a consequence of acute trau- matic injury and only rarely caused by entrapment in the absence of such an injury. This article reviews the anatomy of the radial nerve, common sites of injury and their presentation, and the electrodiagnostic approach to localizing the lesion. ANATOMY OF THE RADIAL NERVE Course of the Radial Nerve The radial nerve subserves the extensors of the arms and fingers and the sensory nerves of the extensor surface of the arm.1–3 Because it serves the sensory and motor Disclosures: Dr Wang has no relevant disclosures. Dr Weiss is a consultant for CSL-Behring and a speaker for Grifols Inc. and Walgreens. He has research support from the Northeast ALS Consortium and ALS Therapy Alliance. -

Nerve Injury After Peripheral Nerve Block: Allbest Rights Practices Reserved
PRINTER-FRIENDLY VERSION AVAILABLE AT ANESTHESIOLOGYNEWS.COM Nerve Injury After Peripheral Nerve Block: AllBest rights Practices reserved. Reproduction and Medical-Legal in whole or in part without Protection permission isStrategies prohibited. Copyright © 2015 McMahon Publishing Group unless otherwise noted. DAVID HARDMAN, MD, MBA Professor of Anesthesiology Vice Chair for Professional Affairs Department of Anesthesiology University of North Carolina at Chapel Hill Chapel Hill, North Carolina Dr. Hardman reports no relevant financial conflicts of interest. he risk for permanent or severe nerve injury after peripheral nerve blocks (PNBs) is Textremely low, irrespective of its etiology (ie, related to anesthesia, surgery or the patient). The risk inherent in a procedure should always be explicitly discussed with the patient (sidebar, page 4). In fact, it may be better to define this phenomenon ultrasound-guided axillary blocks were used, demon- as postoperative neurologic symptoms (PONS) or peri- strated a very low nerve injury rate of 0.0037% at hos- operative nerve injuries (PNI) in order to help stan- pital discharge.1-7 dardize terminology. Permanent injury rates, as defined A 2009 prospective case series involving more than by a neurologic abnormality present at or beyond 12 7,000 PNBs, conducted in Australia and New Zealand, months after the procedure, have consistently ranged demonstrated that when a postoperative neurologic from 0.029% to 0.2%, although the results of a recent symptom was diagnosed, it was 9 times more likely to multicenter Web-based survey in France, in which be due to a non–anesthesia-related cause than a nerve ANESTHESIOLOGY NEWS • JULY 2015 1 block–related cause.6 On the other hand, it is well doc- PNI rate of 1.7% in patients who received a single-injec- umented in the orthopedic and anesthesia literature tion interscalene block (ISB). -

Neuropathology Category Code List
Neuropathology Page 1 of 27 Neuropathology Major Category Code Headings Revised 10/2018 1 General neuroanatomy, pathology, and staining 65000 2 Developmental neuropathology, NOS 65400 3 Epilepsy 66230 4 Vascular disorders 66300 5 Trauma 66600 6 Infectious/inflammatory disease 66750 7 Demyelinating diseases 67200 8 Complications of systemic disorders 67300 9 Aging and neurodegenerative diseases 68000 10 Prion diseases 68400 11 Neoplasms 68500 12 Skeletal Muscle 69500 13 Peripheral Nerve 69800 14 Ophthalmic pathology 69910 Neuropathology Page 2 of 27 Neuropathology 1 General neuroanatomy, pathology, and staining 65000 A Neuroanatomy, NOS 65010 1 Neocortex 65011 2 White matter 65012 3 Entorhinal cortex/hippocampus 65013 4 Deep (basal) nuclei 65014 5 Brain stem 65015 6 Cerebellum 65016 7 Spinal cord 65017 8 Pituitary 65018 9 Pineal 65019 10 Tracts 65020 11 Vascular supply 65021 12 Notochord 65022 B Cell types 65030 1 Neurons 65031 2 Astrocytes 65032 3 Oligodendroglia 65033 4 Ependyma 65034 5 Microglia and mononuclear cells 65035 6 Choroid plexus 65036 7 Meninges 65037 8 Blood vessels 65038 C Cerebrospinal fluid 65045 D Pathologic responses in neurons and axons 65050 1 Axonal degeneration/spheroid/reaction 65051 2 Central chromatolysis 65052 3 Tract degeneration 65053 4 Swollen/ballooned neurons 65054 5 Trans-synaptic neuronal degeneration 65055 6 Olivary hypertrophy 65056 7 Acute ischemic (hypoxic) cell change 65057 8 Apoptosis 65058 9 Protein aggregation 65059 10 Protein degradation/ubiquitin pathway 65060 E Neuronal nuclear inclusions 65100 -

The Usefulness of Proximal Radial Motor Conduction in Acute Compressive Radial Neuropathy
JCN Open Access ORIGINAL ARTICLE pISSN 1738-6586 / eISSN 2005-5013 / J Clin Neurol 2015;11(2):178-182 / http://dx.doi.org/10.3988/jcn.2015.11.2.178 The Usefulness of Proximal Radial Motor Conduction in Acute Compressive Radial Neuropathy Kun Hyun Kima b Background and PurposezzThe objective of this study was to determine diagnostic and Kee-Duk Park a prognostic values of proximal radial motor conduction in acute compressive radial neuropathy. Pil-Wook Chung a MethodszzThirty-nine consecutive cases of acute compressive radial neuropathy with radial Heui-Soo Moon conduction studies–including stimulation at Erb’s point–performed within 14 days from a Yong Bum Kim clinical onset were reviewed. The radial conduction data of 39 control subjects were used as a Won Tae Yoon reference data. b Hyung Jun Park ResultszzThirty-one men and eight women (age, 45.2±12.7 years, mean±SD) were enrolled. Bum Chun Suha All 33 patients in whom clinical follow-up data were available experienced complete recov- ery, with a recovery time of 46.8±34.3 days. Partial conduction block was found frequently a Department of Neurology, Kangbuk Samsung Hospital, (17 patients) on radial conduction studies. The decrease in the compound muscle action po- Sungkyunkwan University tential area between the arm and Erb’s point was an independent predictor for recovery time. School of Medicine, Seoul, Korea zzProximal radial motor conduction appears to be a useful method for the early b Conclusions Department of Neurology, detection and prediction of prognosis of acute compressive radial neuropathy. Mokdong Hospital, Ewha Womans University Key Wordszz radial neuropathy, nerve conduction study, conduction block, diagnosis, School of Medicine, Seoul, Korea prognosis. -

Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know
Anaesthesia & Critical Care Medicine Journal ISSN: 2577-4301 Perioperative Upper Extremity Peripheral Nerve Injury and Patient Positioning: What Anesthesiologists Need to Know Kamel I* and Huck E Review Article Lewis Katz School of Medicine at Temple University, USA Volume 4 Issue 3 Received Date: June 20, 2019 *Corresponding author: Ihab Kamel, Lewis Katz School of Medicine at Temple Published Date: August 01, 2019 University, MEHP 3401 N. Broad street, 3rd floor outpatient building ( Zone-B), DOI: 10.23880/accmj-16000155 Philadelphia, United States, Tel: 2158066599; Email: [email protected] Abstract Peripheral nerve injury is a rare but significant perioperative complication. Despite a variety of investigations that include observational, experimental, human cadaveric and animal studies, we have an incomplete understanding of the etiology of PPNI and the means to prevent it. In this article we reviewed current knowledge pertinent to perioperative upper extremity peripheral nerve injury and optimal intraoperative patient positioning. Keywords: Nerve Fibers; Proprioception; Perineurium; Epineurium; Endoneurium; Neurapraxia; Ulnar Neuropathy Abbreviations: PPNI: Perioperative Peripheral Nerve 2018.The most common perioperative peripheral nerve Injury; MAP: Mean Arterial Pressure; ASA CCP: American injuries involve the upper extremity with ulnar Society of Anesthesiology Closed Claims Project; SSEP: neuropathy and brachial plexus injury being the most Somato Sensory Evoked Potentials frequent [3,4]. In this article we review upper extremity PPNI with regards to anatomy and physiology, Introduction mechanisms of injury, risk factors, and prevention of upper extremity PPNI. Perioperative peripheral nerve injury (PPNI) is a rare complication with a reported incidence of 0.03-0.1% [1,2]. Anatomy and Physiology of Peripheral PPNI is a significant source of patient disability and is the Nerves second most common cause of anesthesia malpractice claims [3,4]. -
069-Workshop-Food Allergy
WORKSHOP Practical Pointers For Your Practice Short Snappers in Neurology: Clinical Strategies and Problems Alan E. Goodridge , MD, FRCPC Presented at Memorial University’s Wednesday at Noon Ask the Consultant Seminar, January 17, 2007. Scenario 1 The approach to the neurological hen faced with a examination Wneurological The neurological exam can be daunting, but strate - problem, it is helpful, gies can be developed to target the key aspects of the during the history, to n neurological exam to answer the clinical questions make ©a judgment utio raised by the history. When faced with a neurologi - ht rib ig ist ad, cal problem, it is helpful, during the history, to mayke rregarding Dwhetwhnelor the p ial n do a judgment regarding whether the probleom is more rc rs ca use C proeblemuseis monoarl e likely likely to be of peripheral or central nervous system mm rised pers o utho y for (CNS) origin. r C ed. Ato bceopof peripheral or o hibit ingle When there are localizianglseymptomprs,osuch ats a s S use prin CNS origin. acute presentatiofnoofra hemirpisleegdia, the ceanntrdal origin t utho view of theNprooblem wUilnl abe obvioluasy. ,With clinical prob - This approach contrasts with problems that, disp lems where there are usually no localizing symp - based on the history, suggest a peripheral nervous toms, such as a headache or a seizure, the clinical system origin. For example, when the symptoms are exam is primarily directed towards the question of a localized to one limb ( i.e., with pain and numbness possible problem of central origin. in one arm).