Full Text Article
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mountain Resources Expliotation For
International Journal of Geography and Régional Planning Research Vol.1,No.1,pp.1-12, March 2014 Published by European Centre for Research Training and Development UK (www.eajournals.org) MONTANE RESOURCES EXPLOITATION AND THE EMERGENCE OF GENDER ISSUES IN SANTA ECONOMY OF THE WESTERN BAMBOUTOS HIGHLANDS, CAMEROON Zephania Nji FOGWE Department of Geography, Box 3132, F.L.S.S., University of Douala ABSTRACT: Highlands have played key roles in the survival history of humankind. They are refuge heavens of valuable resources like fresh water endemic floral and faunal sanctuaries and other ecological imprints. The mountain resource base in most tropical Africa has been mined rather than managed for the benefit of the low-lying areas. The world over an appreciable population derives its sustenance directly from mountain resources and this makes for about one-tenth of the world’s poorest.The Western highlands of Cameroon are an archetypical territory of a high population density and an economically very active population. The highlands are characterised by an ecological fragility and a multi-faceted socio-economic dynamism at varied levels of poverty, malnutrition and under employment, yet about 80 percent of the Santa highlands’ population depends on its natural resource base of vast fertile land, fresh water and montane refuge forest for their livelihood. KEYWORDS: Montane Resources, Gender Issues, Santa Economy, Western Bamboutos, Cameroon INTRODUCTION The volcanic landscape on the western slopes of the Bamboutos mountain range slopes to the Santa Highlands is an area where agriculture in the form of crop production and animal rearing thrives with remarkable success. Arabica coffee cultivation was in extensive hectares cultivated at altitudes of about 1700m at the Santa Coffee Estate at Mile 12 in the 1970s and 1980s. -

An Inventory of Short Horn Grasshoppers in the Menoua Division, West Region of Cameroon
AGRICULTURE AND BIOLOGY JOURNAL OF NORTH AMERICA ISSN Print: 2151-7517, ISSN Online: 2151-7525, doi:10.5251/abjna.2013.4.3.291.299 © 2013, ScienceHuβ, http://www.scihub.org/ABJNA An inventory of short horn grasshoppers in the Menoua Division, West Region of Cameroon Seino RA1, Dongmo TI1, Ghogomu RT2, Kekeunou S3, Chifon RN1, Manjeli Y4 1Laboratory of Applied Ecology (LABEA), Department of Animal Biology, Faculty of Science, University of Dschang, P.O. Box 353 Dschang, Cameroon, 2Department of Plant Protection, Faculty of Agriculture and Agronomic Sciences (FASA), University of Dschang, P.O. Box 222, Dschang, Cameroon. 3 Département de Biologie et Physiologie Animale, Faculté des Sciences, Université de Yaoundé 1, Cameroun 4 Department of Biotechnology and Animal Production, Faculty of Agriculture and Agronomic Sciences (FASA), University of Dschang, P.O. Box 222, Dschang, Cameroon. ABSTRACT The present study was carried out as a first documentation of short horn grasshoppers in the Menoua Division of Cameroon. A total of 1587 specimens were collected from six sites i.e. Dschang (265), Fokoue (253), Fongo – Tongo (267), Nkong – Ni (271), Penka Michel (268) and Santchou (263). Identification of these grasshoppers showed 28 species that included 22 Acrididae and 6 Pyrgomorphidae. The Acrididae belonged to 8 subfamilies (Acridinae, Catantopinae, Cyrtacanthacridinae, Eyprepocnemidinae, Oedipodinae, Oxyinae, Spathosterninae and Tropidopolinae) while the Pyrgomorphidae belonged to only one subfamily (Pyrgomorphinae). The Catantopinae (Acrididae) showed the highest number of species while Oxyinae, Spathosterninae and Tropidopolinae showed only one species each. Ten Acrididae species (Acanthacris ruficornis, Anacatantops sp, Catantops melanostictus, Coryphosima stenoptera, Cyrtacanthacris aeruginosa, Eyprepocnemis noxia, Gastrimargus africanus, Heteropternis sp, Ornithacris turbida, and Trilophidia conturbata ) and one Pyrgomorphidae (Zonocerus variegatus) were collected in all the six sites. -

Occlusionocclusion The KEY to Dentistry
OcclusionOcclusion The KEY to dentistry. The KEY to total health. The KEY to this website. A1 Basics of Occlusion Simplistic definition of occlusion: The way teeth meet and function. A2 The BEST textbook on dentistry. Every dentist should read. Peter E. Dawson. Evaluation, Diagnosis, and Treatment of Occlusal Problems, 2nd ed.. Mosby. A3 I am standing beside, in my opinion, one of the best dentists in the world, Dr. Peter Dawson. A4 Centric Relation (CR) Refers to the RELATIONSHIP of the MANDIBLE TO THE SKULL as it rotates around the ‘hinge-axis” before any translatory movement of the condyles from their “upper-most and mid-most position”. It is irrespective of tooth position or vertical dimension. Peter E. Dawson. Evaluation, Diagnosis, and Treatment A5 of Occlusal Problems, 2nd ed.. Mosby. Left TMJ Condyles in socket. Condyles advanced. Right TMJ Green arrows: Head of condyle. Transcranial radiograph of TMJ. White arrows: Articular tubercle. A6 Red arrows: Glenoid fossa. Condyle: The rounded articular surface at the end of the mandible (lower jaw). Glenoid fossa: A deep concavity in the temporal bone a the root of the zygomatic arch that receives the condyle of the mandible. Tubercle: A slight elevation from the surface of the bone giving attachment to a muscle or ligament. A7 Balancing side. Working side. Condyle has downward path. Condyle pivots. Mandible &TMJ A8 Working side: (Mandible moving toward the cheek) Working side condyle pivots within the socket and is better supported. Balancing side: (Mandible moving toward the tongue) Balancing side condyle has a downward orbiting path. It is traveling a greater distance in ‘space’ and is more prone to injury or damage. -

Assessing Cost Efficiency Among Small Scale Rice Producers in the West Region of Cameroon: a Stochastic Frontier Model Approach
International Journal of Humanities Social Sciences and Education (IJHSSE) Volume 3, Issue 6, June 2016, PP 1-7 ISSN 2349-0373 (Print) & ISSN 2349-0381 (Online) http://dx.doi.org/10.20431/2349-0381.0306001 www.arcjournals.org Assessing Cost Efficiency among Small Scale Rice Producers in the West Region of Cameroon: A Stochastic Frontier Model Approach Djomo, Raoul Fani*1, Ewung, Bethel1, Egbeadumah, Maryanne Odufa2 1Department of Agricultural Economics. University of Agriculture, Makurdi. Benue-State, Nigeria PMB 2373, Makurdi 2Department of Agricultural Economics and Extension, Federal University Wukari, PMB 1020 Wukari. Taraba State, Nigeria *[email protected] Abstract: Local farmers’ techniques and knowledge in rice cultivation being deficient and the aid system and research to support such farmers’ activities likewise insufficient, technological progress and increase in rice production are not yet assured. Therefore, this Study was undertaken to assess cost efficiency among small scale rice farmers in the West Region of Cameroon using stochastic frontier model approach. A purposive, multistage and stratified random sampling technique was used in selecting the respondents. A total of 192 small scale rice farmers were purposively selected from four (4) out of eight divisions. Data were collected using structured questionnaires and interview schedule, administered on the respondents were analyzed using descriptive statistics and stochastic frontier cost functions. The result indicates that the coefficient of cost of labour was found positive and significantly influence cost of production in small scale rice production at 1 percent level of probability, implying that increases in cost of labour by one unit will also increase cost of production in small scale rice farming by the value of it coefficient. -
Occlusion, Function, and Parafunction: Understanding the Dynamics of a Healthy Stomatagnathic System a Peer-Reviewed Publication Written by Steven D
Earn 4 CE credits This course was written for dentists, dental hygienists, and assistants. Occlusion, Function, and Parafunction: Understanding the Dynamics of a Healthy Stomatagnathic System A Peer-Reviewed Publication Written by Steven D. Bender, DDS This course has been made possible through an unrestricted educational grant. The cost of this CE course is $59.00 for 4 CE credits. Cancellation/Refund Policy: Any participant who is not 100% satisfied with this course can request a full refund by contacting PennWell in writing. Educational Objectives Since it is probable that sleep bruxism differs in terms of etiology Upon completion of this course, the clinician will be able to do from daytime parafunctional jaw muscle activity, it should be the following: distinguished from teeth clenching, bracing, or grinding while 1. Define parafunction and the activities associated with this awake.7,8 It has been estimated that 8 percent of adults in the 2. Identify the signs and symptoms of parafunctional activity general population are aware of teeth grinding during sleep, usu- 3. Know the considerations and steps involved in diagnosing ally as reported by their sleep partners or roommates.9 According parafunctional activity to parental reports, the incidence of teeth grinding noises during 4. Identify the types of appliances that can be used to manage sleep in children younger than 11 years of age is between 14 and parafunction, their advantages and disadvantages, and 20 percent.10,11 Dental signs of bruxism can be seen in approxi- considerations in selecting an appliance for individual patients mately 10 to 20 percent of children.12 Studies have shown that approximately 60 percent of “normal” sleepers exhibit rhythmic Abstract masticatory muscle activity (RMMA) during sleep. -

Occlusion and Articulation in Bruxism and Bruxomania Investigated with the System T-Scan Iii
http://dx.doi.org/10.5272/jimab.2014205.655 Journal of IMAB Journal of IMAB - Annual Proceeding (Scientific Papers) 2014, vol. 20, issue 5 ISSN: 1312-773X http://www.journal-imab-bg.org OCCLUSION AND ARTICULATION IN BRUXISM AND BRUXOMANIA INVESTIGATED WITH THE SYSTEM T-SCAN III Mariana Dimova Department of Prosthetic Dental Medicine, Faculty of Dental Medicine, Medical University-Sofia, Bulgaria SUMMARY: istration with articulation paper or impression materials does Aim: To be analyzed common features of occlusal not have quantitative timing and descriptive power capac- relationships in patients with bruxism and bruxomania at ity, while computerized occlusal analysis allows identifica- maximum intercuspation (MIP) and eccentric jaw tion and documentation of the sequence of occurrence, du- movements. ration, distribution and power of all contacts. According to Materials and Methods: 30 patients (22 women and several authors [9 - 11] computerized occlusal analysis pro- 8 men, mean aged of 42,8 ± 13,3) with bruxism and/or vides valuable diagnostic capabilities for measuring and re- bruxomania are examined with the system T-Scan III. producing both the positions of occlusal contacts in maxi- Sequence of records is - at maximum intercuspation (MIP); mum intercuspation and during articulation. in manual leading to central relation and in eccentric jaw These advantages of the digital study of occlusion movements. may be used in diagnosis of patients with bruxism and In the same sequence is investigated control group - bruxomania. 30 people (15 women and 15 men) aged between 21 and 45 who didn’t have bruxism and/or bruxomania and AIM: To analyze occlusal relationships in patients dentition is preserved. -

A Collection of 100 Proverbs and Wise Sayings of the Medumba (Cameroon)
A COLLECTION OF 100 PROVERBS AND WISE SAYINGS OF THE MEDUMBA (CAMEROON) BY CIKURU BISHANGI DEVOTHA AFRICAN PROVERBS WORKING GROUP NAIROBI KENYA MAY 2019 i ACKNOWLEDGEMENT I wish to thank sincerely all those who contributed towards the completion of this document. My greatest thanks go to Fr. Joseph G. Healey for the financial and moral support. My special thanks go to Cephas Agbemenu, Margret Wambere Ireri and Father Joseph Healey. I also thank all the publishers of African Proverbs whose publications gave me good resource and inspiration to do this work. I appreciate the support of the African Proverbs Working Group for reviewing the progress of my work during their meetings. Find in this work all my gratitude. DEDICATION I dedicate this work to God for protecting and strengthening me while working on the Medumba. To HONDI M. Placide, my husband and my mentor who encouraged me to complete this research, To my collaborator Emmanuel Fandja who helped me to collect the 100 Medumba Proverbs. To all the members of my community in Nairobi and to all those who will appreciate in finding out the wisdom that it contains. i A COLLECTION OF 100 MEDUMBA PROVERBS AND WISE SAYINGS (CAMEROOON) INTRODUCTION Location The Bamileke is the native group which is now dominant in Cameroon's West and Northwest Regions. It is part of the Semi-Bantu (or Grassfields Bantu) ethnic group. The Bamileke are regrouped under several groups, each under the guidance of a chief or fon. Nonetheless, all of these groups have the same ancestors and thus share the same history, culture, and languages. -

Evaluating the Constraints and Opportunities of Maize Production in the West Region of Cameroon for Sustainable Development
Journal of Sustainable Development in Africa (Volume 13, No.4, 2011) ISSN: 1520-5509 Clarion University of Pennsylvania, Clarion, Pennsylvania EVALUATING THE CONSTRAINTS AND OPPORTUNITIES OF MAIZE PRODUCTION IN THE WEST REGION OF CAMEROON FOR SUSTAINABLE DEVELOPMENT Godwin Anjeinu Abu1, Raoul Fani Djomo-Choumbou1 and Stephen Adogwu Okpachu2 1. Department of Agricultural Economics, University of Agriculture PMB 2373, Makurdi Benue State- Nigeria 2. Federal College of Education (Technical), Potiskum, Yobe State, Nigeria ABSTRACT A study of Evaluating the constraints and opportunities of Maize production in the West Region of Cameroon was carried out using primary and secondary data collected. One hundred and twenty (120) maize farmers randomly selected from eight (8) villages were interviewed using structured questionnaire. Data from the study were analyzed using descriptive statistics such as frequency distribution, percentages, and inferential statistics such as multiple linear regressions. The study found that most maize farmers in the study area were small scale farmers and are full time farmers, the major maize production constraints was poor access to credit facilities. it was also found any unit increase in the quantity of any of the resources used for maize production will increase maize output by the value of their estimated coefficients respectively , however to raise maize production, the study recommend that financial institutions such as agricultural and community banks should be established in the study area with the simple procedure of securing loans. The relevant government agencies and non- governmental organization should mobilize the maize farmers to form themselves into formidable group so that they can derive maximum benefit of collective union. -
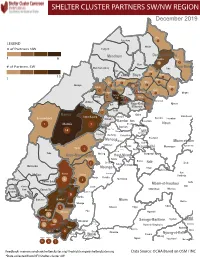
NW SW Presence Map Complete Copy
SHELTER CLUSTER PARTNERS SW/NWMap creation da tREGIONe: 06/12/2018 December 2019 Ako Furu-Awa 1 LEGEND Misaje # of Partners NW Fungom Menchum Donga-Mantung 1 6 Nkambe Nwa 3 1 Bum # of Partners SW Menchum-Valley Ndu Mayo-Banyo Wum Noni 1 Fundong Nkum 15 Boyo 1 1 Njinikom Kumbo Oku 1 Bafut 1 Belo Akwaya 1 3 1 Njikwa Bui Mbven 1 2 Mezam 2 Jakiri Mbengwi Babessi 1 Magba Bamenda Tubah 2 2 Bamenda Ndop Momo 6b 3 4 2 3 Bangourain Widikum Ngie Bamenda Bali 1 Ngo-Ketunjia Njimom Balikumbat Batibo Santa 2 Manyu Galim Upper Bayang Babadjou Malentouen Eyumodjock Wabane Koutaba Foumban Bambo7 tos Kouoptamo 1 Mamfe 7 Lebialem M ouda Noun Batcham Bafoussam Alou Fongo-Tongo 2e 14 Nkong-Ni BafouMssamif 1eir Fontem Dschang Penka-Michel Bamendjou Poumougne Foumbot MenouaFokoué Mbam-et-Kim Baham Djebem Santchou Bandja Batié Massangam Ngambé-Tikar Nguti Koung-Khi 1 Banka Bangou Kekem Toko Kupe-Manenguba Melong Haut-Nkam Bangangté Bafang Bana Bangem Banwa Bazou Baré-Bakem Ndé 1 Bakou Deuk Mundemba Nord-Makombé Moungo Tonga Makénéné Konye Nkongsamba 1er Kon Ndian Tombel Yambetta Manjo Nlonako Isangele 5 1 Nkondjock Dikome Balue Bafia Kumba Mbam-et-Inoubou Kombo Loum Kiiki Kombo Itindi Ekondo Titi Ndikiniméki Nitoukou Abedimo Meme Njombé-Penja 9 Mombo Idabato Bamusso Kumba 1 Nkam Bokito Kumba Mbanga 1 Yabassi Yingui Ndom Mbonge Muyuka Fiko Ngambé 6 Nyanon Lekié West-Coast Sanaga-Maritime Monatélé 5 Fako Dibombari Douala 55 Buea 5e Massock-Songloulou Evodoula Tiko Nguibassal Limbe1 Douala 4e Edéa 2e Okola Limbe 2 6 Douala Dibamba Limbe 3 Douala 6e Wou3rei Pouma Nyong-et-Kellé Douala 6e Dibang Limbe 1 Limbe 2 Limbe 3 Dizangué Ngwei Ngog-Mapubi Matomb Lobo 13 54 1 Feedback: [email protected]/ [email protected] Data Source: OCHA Based on OSM / INC *Data collected from NFI/Shelter cluster 4W. -

The All-On-Four Treatment Concept: Systematic Review
J Clin Exp Dent. 2017;9(3):e474-88. All-on-four: Systematic review Journal section: Prosthetic Dentistry doi:10.4317/jced.53613 Publication Types: Review http://dx.doi.org/10.4317/jced.53613 The all-on-four treatment concept: Systematic review David Soto-Peñaloza 1, Regino Zaragozí-Alonso 2, María Peñarrocha-Diago 3, Miguel Peñarrocha-Diago 4 1 Collaborating Lecturer, Master in Oral Surgery and Implant Dentistry, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain Peruvian Army Officer, Stomatology Department, Luis Arias Schreiber-Central Military Hospital, Lima-Perú 2 Dentist, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain 3 Assistant Professor of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain 4 Professor and Chairman of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain Correspondence: Unidad de Cirugía Bucal Facultat de Medicina i Odontologìa Universitat de València Gascó Oliag 1 46010 - Valencia, Spain [email protected] Soto-Peñaloza D, Zaragozí-Alonso R, Peñarrocha-Diago MA, Peñarro- cha-Diago M. The all-on-four treatment concept: Systematic review. J Clin Exp Dent. 2017;9(3):e474-88. http://www.medicinaoral.com/odo/volumenes/v9i3/jcedv9i3p474.pdf Received: 17/11/2016 Accepted: 16/12/2016 Article Number: 53613 http://www.medicinaoral.com/odo/indice.htm © Medicina Oral S. L. C.I.F. B 96689336 - eISSN: 1989-5488 eMail: [email protected] Indexed in: Pubmed Pubmed Central® (PMC) Scopus DOI® System Abstract Objectives: To systematically review the literature on the “all-on-four” treatment concept regarding its indications, surgical procedures, prosthetic protocols and technical and biological complications after at least three years in function. -

Skeeling 1.Pdf
Musicking Tradition in Place: Participation, Values, and Banks in Bamiléké Territory by Simon Robert Jo-Keeling A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy (Anthropology) in The University of Michigan 2011 Doctoral Committee: Professor Judith T. Irvine, Chair Emeritus Professor Judith O. Becker Professor Bruce Mannheim Associate Professor Kelly M. Askew © Simon Robert Jo-Keeling, 2011 acknowledgements Most of all, my thanks go to those residents of Cameroon who assisted with or parti- cipated in my research, especially Theophile Ematchoua, Theophile Issola Missé, Moise Kamndjo, Valerie Kamta, Majolie Kwamu Wandji, Josiane Mbakob, Georges Ngandjou, Antoine Ngoyou Tchouta, Francois Nkwilang, Epiphanie Nya, Basil, Brenda, Elizabeth, Julienne, Majolie, Moise, Pierre, Raisa, Rita, Tresor, Yonga, Le Comité d’Etudes et de la Production des Oeuvres Mèdûmbà and the real-life Association de Benskin and Associa- tion de Mangambeu. Most of all Cameroonians, I thank Emanuel Kamadjou, Alain Kamtchoua, Jules Tankeu and Elise, and Joseph Wansi Eyoumbi. I am grateful to the Wenner-Gren Foundation for Anthropological Research for fund- ing my field work. For support, guidance, inspiration, encouragement, and mentoring, I thank the mem- bers of my dissertation committee, Kelly Askew, Judith Becker, Judith Irvine, and Bruce Mannheim. The three members from the anthropology department supported me the whole way through my graduate training. I am especially grateful to my superb advisor, Judith Irvine, who worked very closely and skillfully with me, particularly during field work and writing up. Other people affiliated with the department of anthropology at the University of Michigan were especially helpful or supportive in a variety of ways. -

Forets Sacres Au Cameroun.Pdf
M.E.M Millennium Ecologic Museum Ministère des Forêts et de la Faune Inventaire, cartographie et étude diagnostic des forêts sacrées du Cameroun : contribution à l’élaboration d’une stratégie nationale de gestion durable RAPPORT FINAL D’EXECUTION Avec l’appui financier du Programme CARPE-IUCN Juin 2010 0 Millennium Ecologic Museum MEM BP : 8038 Yaoundé, Cameroun Tel : (237) 99 99 54 08 / 96 68 11 34 e-mail : [email protected] Site web: www.ecologicalmuseum.netsons.org 1 L’EQUIPE DU PROJET Conseiller Technique Principal Prof. Bernard-Aloys NKONGMENECK, Directeur du MEM Point Focal MINFOF M. NOBANZA Francis, MINFOF/SDIAF - Service Cartographie Conseillers Scientifiques Guy Merlin NGUENANG Vincent BELIGNE Coordination des activités terrain et rapportage Evariste FONGNZOSSIE Collecte des données Victor Aimé KEMEUZE et René Bernadin JIOFACK Assistés de : JOHNSON Madeleine MAKEMTEU Junelle KAMDEM Gyslène WONKAM Christelle TABI Paule Pamela TAJEUKEM Vice Clotex MVETUMBO Moise KENNE Florette Base de Données et GIS Victor KEMEUZE et Francis NOBANZA 2 SOMMAIRE DU RAPPORT LISTE DES ACRONYMES....................................................................................................................................... 6 LISTE DES FIGURES .............................................................................................................................................. 7 LISTE DES TABLEAUX .........................................................................................................................................